Your Questions
Your Questions
Q: Dr. Eppley, I have worries about a silicone implant for skull augmentation. First I know it can cause cancer. Also, there will be a void between the implant to the actual skull (what will be filled in there I don’t know, and the feeling of it), probably I will need to replace it after a few years.. (it’s not permanent) and I’m scared having metal (screws) in my head.
Also, I am from the Middle East so monitoring after an implant will be hard from here in case any problem will occur.
Do not use at all bone cement?
A: In answer to your skull augmentation questions:
While I am happy to sue whatever skull implantation material the patient desires, and I have used them all, you have some understandable misconceptions about them which I will clarify.
1) There has never been a case, anywhere in the body, where a smooth SOLID silicone implant has ever caused cancer. You are confusing a solid skull implant with non-solid (gel) breast implants.
2) There is no ‘void’ that occurs between the silicone skull implant and the bone. While true bony integration into the implant does not occur, the small millimeter layer is filled with scar tissue. (known as the capsule)
3) Custom silicone skull implants are permanent, just like bone cement, and never have to be replaced due to any type of device failure. Here again you are likely confusing skull implants with breast implants.
4) The use of metal screws in skull implants is not mandatory. There are only put there as an extra layer of positioning security but are not mandatory. Actually screws are also in bone cements as anchorage points where they are more essential than they are in silicone skull implants.
5) The risk of postoperative issues/complications/need for revisions is actually much higher with bone cements in my experience. They have aesthetic higher risks of irregularities/asymmetries and the need for revisions to manage them.
6) The incision needed for a custom implant vs bone cement skull augmentation is significantly different. Bone cement skull augmentation require a full coronal scalp incision, custom skull implants do not.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was hoping to receive some information about getting a revision surgery for my hip augmentation and also potentially getting my current buttock implants replaced with a larger size. I received both hip and buttock augmentation last year using custom implants for my buttocks and custom implants for my hips as well. While the intramuscular buttock surgery went well, the subfascial hip implants have been a huge problem for me. They seemed to be fine at first, but over time they’ve dropped lower on my leg, and are now protruding unnaturally and moving around. Attached are some photos of my protruding hip implants, for reference.
I did some research and saw that you’re an expert at revision surgery and custom implants, so I figured you were the right person to ask about my very specific situation. Are these revisions something that you would be willing to perform, and if so, do you have any other advice or information you could provide (pricing, recovery, etc)? Please let me know, and thanks in advance for your help.
A:Thank you for your inquiry and sending your picture and detailing your surgical history to which I can say the following:
1) Hip implants are very different than buttock implants in terms of pocket location. Buttock implants are locked into place by the intramuscular location. Hip implants, however, can not have an intra- or submuscular location and must be placed above the muscle or technically on top of the TFL fascia. As a result, there is the risk of inferior migration as they heal.
2) With this inferior migration comes an elongated pocket. Since the silicone surface does not adhere to the overlying tissues what you have now is an implant that is too ‘small’ for the pocket and thus can freely slide up and down. (pocket is vertically longer than the implant)
3) The most predictable approach is to work with the existing size of the implant pocket as making hip implant pockets smaller by trying to raise it and stay raised is prone to failure. (not to mention that it also requires a new incision at the bottom end of the pocket to do so)
4) Thus making a new longer implant to fit the length of the pocket width with an improved side profile would be the approach. Your existing hip implant is a version of the CCB7 implant design which has the maximum projection in the upper third of the implant. You would likely be better served by having a mid-implant projection point. (see attachments which shows the basic design file of the implants you currently have in place….although the exact dimensions I do not yet know.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, how much to make top of head taller by 2 inches, head wider by about 2 inches, is it possible to lower upper and lower jaw down about an inch with tache, lips, cheeks? And the nose longer about 1 inch. if so how much. I have short face and want longer. And can you make the eyebrow ridge higher and eyes deeper set then make nose thicker and wider?
A: While all of the skull, nose and lower jaw lengthening changes can be done, they can not be done to the magnitude that you describe due to the limitations of the overlying soft tissues:
1) the skull can be augmented usually by 1/2 to one inch but not two.
2) The nose can be lengthened by 5 to 7mms (1/3 inch) but not one inch.
3) The jawline can be lowered usually up to 8mms at the chin area (longer in the back) but not by one inch at the chin.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was wondering if you have any experience with this new product Volux by Allergan, it seems like it is a higher density and mainly used for the jawline and chin. I have used Radiesse before and it did a good job but its all gone now. Also if you know about Volux since it is a higher density would you know if it is less likely to migrate or inject into a blood vessel since maybe it would not travel far in the bloodstream? Lastly is there any way or diagnostic test to map my arteries in my face so you can see where they lie depth and location before injecting or while injecting in realtime? Anything new that you know about?
A: In answer to your Volux injectable filler questions:
1) Volux has increased cross-linking over that of other hyaluronic-acid based fillers but is still less dense that than of Radiesse. It is designed to be a competitive analogue but is still less dense than any product that contains calcium hydroxyapatite spheres.
2) Like any injectable filler, inadvertent intravascular injection is always possible. There is no clinically usable mapping method for where the smaller arteries and veins lie. The best way to avoid intravascular injection is to use cannulas and not needles to do so.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m contacting you because I would like a better profile of my face. I feel like I’m just going around in circles and I just need good advice. I hate my double chin. I had submental liposuction and it looks worse. Can I realistically get rid of all the fat under my chin? I have a recessive chin, weak jawline and fat neck (I want this neck fat gone pls). I want a clear distinction between neck and jaw because this is beautiful and looks balanced. I have been told to get a necklift to address the issue but I feel too young. And even if I do get a necklift, it doesn’t resolve the weak structure in the jaw; and it won’t hold up for long, I need volume in the jaw. Also does a necklift include a platysmaplasty? I don’t like the implant scar (2 cm). Although a doc told me a flower implant would be a good fit for me. Yet another doc said an implant could move, or make my chin bone smaller. So is a genioplasty the answer? I don’t know what to do. Another thing I’d like is to remove the bags from inside my eye. A certain doctor told me not to do that,to do a treatment instead. Maybe I should consider necklift? otherwise, it feels I’ll never get rid of neck fat. Am I too young for that? I am more confused than ever, please help me!
A: Thank you for your inquiry and sending your pictures and detailing your concerns. It is actually understandable why you would be confused about your lower face/neck because you are not a standard case. Your thicker tissues combined with your natural jawline and neck shape make it difficult to be successfully treated by commonly done standard approaches that most plastic surgeons use. You ideally need a combination of hard tissue augmentation and soft tissue reduction meaning:
1) Your neck would have initially been better treated by a submentoplasty, not just liposuction. A submentoplasty combines liposuction removal of fat above the muscle, excision of subplatysmal fat with midline muscle plication. This always produces a better result in fuller necks than liposuction alone. You do not need a necklift/ower facelift, you are correct int that you are both too young and done have the tissue laxity to justify that effort.
2) Augmenting the jawline in some fashion is always a good complementary procedure to separate the face from the neck. Whether that is just a chin augmentation or a total jawline one can be debated depending upon your desired aesthetic outcome. But even if is just the chin, a sliding genioplasty offers a better neck effect than an implant because of the forward pull of the bone on the upper neck muscles. While your chin augmentation needs can certainly be met by an implant, it is how it would better benefit the neck that sways the bony geniopasty in favor for your aesthetic needs. Pulling the chin/neck forward and tightening cervicomental angle would provide the best possible outcome even if falls a little short of your ideal goals as this provides a maximal anatomic reshaping.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a female in my 20s who is interested in maximizing my facial aesthetics. I did my research and came across much of your transformative work with facial implants. I am potentially interested in receiving a sliding genioplasty and jaw angle implants to beautify my face in hopes of achieving “model-like” bone structure.
I currently have 5mm medpor cheek implants and a 5mm medpor wing chin implant. My medpor implant was never fully adequate but to make matters worse, I had my open bite closed with molar intrusion and the counterclockwise rotation of my jaw has made it look even more recessed by tilting the implant upwards. I am hoping to have the implant removed and replaced for a genioplasty.
Right now I am currently shopping for prices and exploring this possibility. If I do not have sleep apnea and thus do not require jaw surgery, then I will like to pursue this.
I can provide before/after morphs if needed. Would I be able to have a ballpark estimate that includes the hospital stay?
Thank you kindly!
A: Thank you for your inquiry and detailing your surgical history and aesthetic facial objectives. Whether the combination of a sliding genioplasty and jaw angle implants can achieve your goals would require an assessment of our own before and after imaging. I am particularly keen on seeing what kind of connection exists between the front and the back (chin and jaw angles) and determine whether independent ‘corner’ jawline procedures alone can effectively approximate your lower facial reshaping goals.
In the interim, however, we will assume that it can and my assistant Camille will send along the cost of the surgery to you later today.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, What are the mechanics of lowering the brow ridge via a custom brow bone implant? Does the implant wrap around the underside of the supraorbital rim to allow projection from a lower level than the pre-existing bone would naturally allow or do I misunderstand this procedure?
Moreover, I’ve noticed that when it comes to implants for the orbital area in general, some merely project forward while others wrap around the rim or are “saddled” as I remember you putting it. What are the differences between these approaches and what kind of results do they tend to yield?
A: In answer to your custom brow bone implant questions:
1) In regards to lowering the brow ridge you are correct in that the implant must extend down and wrap around the bottom of the brow bone to achieve a lower projecting brow bone.
2) Whether an orbital implant lays on its outer surface or wraps around the rim depends on what one is trying to achieve…one is for horizontal augmentation while the other is for combined vertical and horizontal augmentation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I could see that jawline implants inserted through the inside of the mouth have a higher risk of infections And considering the high price (operation + plane + hotel) of it for me, it is a risk that I cannot afford, unfortunately. However can we consider another option, instead of a single wrap around jaw/chin implant with internal placement, instead we would place 3 implants externally, one chin and two mandibles , each customized and fixed by screws.
– Do you think this is possible, or is it not very reliable?
– For sure the result will not be as good as with a single complete implant, but can it approach it? (For the advancement of the chin I think the result may be similar but for the definition of the jaw the result will be less effective?)
Have a nice day
A: Your question is a reasonable one. It is true that performing the surgery externally would lower the risk of infection as opposed to going intraorally….although no implant operation can have a zero risk of infection. But it would drop it down from around 4% to 1% which is a 4X lower risk.
The key questions about this approach are the following:
1) The acceptance of fine line scar right at the back of the jaw angle area.
2) Going externally does not preclude a wrap around jaw implant. While I have never placed one that way, much of the dissection is actually done from the submental incision. It is the fine details of the dissection around the jaw angle area that need an open approach and I suspect that that all could be done from the small external incision.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in temporal lifts. I have attached the wish pictures of results. Please tell me what do you think of these technique, and if this technique is the same you would do ? Also is there are chance of resulting a bad scar from this on the temporal hairline? And if there is a chance of alopecia?
A: Thank you for sending the pictures of the temporal lifting technique and that is exactly the technique to which I was referring. But when you excise skin only at the temporal hairline such a result is not maintained due to the stretch of the skin. That is why you re not looking any long-terms result. (these pictures were taken right at the completion of the procedure which was done under local anesthesia….I have seen these same pictures many times) While skin excision only at the temporal hairline can be one part of a successful lateral temporal brow-cheek lift, it can not be the only technique down as the result will relapse quickly as it places too much stress on the temporal hairline scar. The temporal part of the lift requires subfascial dissection to the lateral brow bone where the periosteum is released and the same issue applies to the cheeks. Deep suture plication of the brow and cheeks are then done. This requires a small upper and lower eyelid incision as well.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am currently looking for ways to make changes to my face because I am not really satisfied with the shape. I have just discovered your site and am wondering if you can help me. My problem is difficult to explain, but I want to try it. My jaw is generally very square. My jaw angle is almost 90 degrees. As a result, my chin is not really pronounced and the jawline is very flat. I would like a steeper angle from jaw to chin with a gonial angle 120 ° – 130 °. Generally, I would like my face to look more down rather than forwards grown. It is important for me that the surgery should not just be a corrective measure, it should be a big change. How can I do this? Is this possible with implants in the chin and along the jawline?
I have already heard of techniques in which the jawbone is shaved to make the jawline steeper and to put the gonial angle further up. However, I have the feeling that my face is too small in the lower third and therefore there is too little space.
A: Thank you for your inquiry. By description you are referring to changing the mandibular plane angle to a more steep one. This is done by lengthening it of which that length needs to be more in the front (chin) than in the back. (jaw angle) There are two methods available for differential vertical lengthening of the jawline which are: 1) total custom jawline implant, and 2) vertical lengthening genioplasty with custom jaw angle/jawline implant. The key determinant between these two options is how much vertical lengthening is needed in the chin. This will ultimately require computer imaging of your pictures to make that determination.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, the back of my head is completely flat from the top of my skull to my neck. This has always bothered me and thought I’d have to live the rest of my life with it. As a woman I’ve never been able to wear cute short haircuts. I keep my long hair held back with a bandanna. I have to be careful how I tie it and place it because it will slip right off my flat head. I have to make sure the knot is placed to the side so it won’t pop out and show from under my hair at the back of my head. Is there a plastic surgery that can give me a nicely curved “bump” to the back of my head? Thank you in advance for your time.
A: Thank you for your inquiry. Back of the head augmentations are common in my practice and there are two methods to achieve a significant augmentation effect. How much augmentation can be achieved is highly dependent on how much augmentation the patient desires and whether the scalp can stretch to accommodate it. While the placement of a custom occipital skull implant can be done, by itself, it will not achieve the maximum augmentation result that most women desire in my experience due to the limited scalp stretch that you undoubtably have given the congenital nature of the skull flatness. Thus the potential need for a two stage approach with either placement of a first stage scalp expander followed by a second stage skull implant or the use of a layered two piece custom skull implant using a staged approach to the implant placements.
I would need to see a side view picture of the back of your head to do some computer imaging to determine your exact back of head augmentation needs.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have read from some sources that orbital box osteotomies is an extremely risky procedure, but have read elsewhere that the risks are over exaggerated. Can I please ask for your opinion of the risks involved? Also, are there any alternatives that you know of that can increase interpupillary distance?
A: From a medical standpoint I would not consider orbital box osteotomies as particularly risky, although it does require a frontal craniotomy to perform. From an aesthetic standpoint, however, there are going to be some tradeoffs. (bony irregularities, long coronal scalp scar) And 100% of orbital box osteotomy patients (children, teens and adults) are going to need revisional surgery to improve any of the aesthetic tradeoffs. Thus like all aesthetic surgery, which always trading one problem for others, the decision for surgery is balancing the benefits vs the risks.
Dr. Barry Eppley
Indianapolis, Indiana
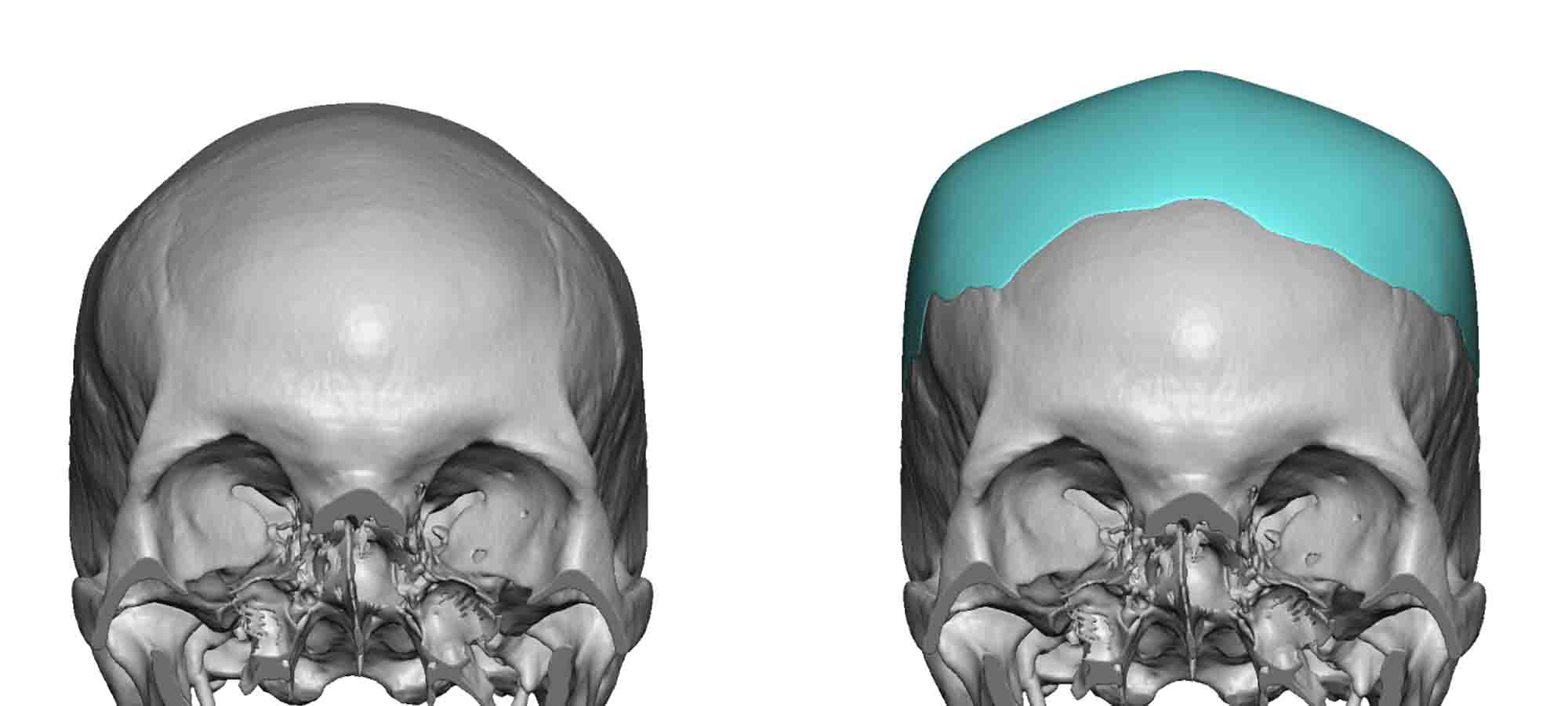
Q: Dr. Eppley, Hello, I have a flat crown/flat back of skull. I figure I would need about an 1 1/2 inches of added depth to the top and back of skull to provide my ideal skull shape. Please advise if this can be attained realistically. Thanks.
A: Thank you for your inquiry and sending your pictures. Crown of skull/back of heads are commonly done using a custom skull implant. However the stretch of the scalp always a controlling factor in how much augmentation can be achieved in a single surgery. While I would question the number of an ‘inch and a half’ or 37mms of augmentation that is actually needed (most people way overestimate their augmentation needs as they do not appreciate the effects that come with the large surface area effect of changing a convex surface), suffice it to say that your optimal augmentation needs could only met with a two stage approach. Such a two stage approach uses either a first stage scalp expansion followed by placement of the definitive implant or designing a two piece implant and placing the layered implants in two stages.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had sliding genioplasty about an year ago. I am not happy with the results as the previous surgeon extended my chin downward by 5mm, but I had asked for an extension around 9-10mm. Is it possible to perform a revision on the prior surgery to give me the desired chin extension?
A: If I understand your sliding genioplasty concerns, you desired a 10mm bony vertical lengthening but ended up with only 5mms. The prior surgery can be repeated to add further desired vertical lengthening. The bone will heal just fine and I always add tissue bank corticocancellous chips to it to ensure healing and fill in any bony gaps.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Im interested in temporal lift to elevate my brows laterally only (not interested in endoscopic or coronal brow lift) including elevating my upper cheek lift, with the same temporal incision .. Will you be so kind to let me know the price for this procedure and what is your technique? Are you going to just remove a little bit of skin and then suture? Or are you going to dissect the whole tissue?
A: While temporal or lateral brow lifts can be done by several techniques, your interest by your own description is in what is known as a more direct or excisional approach. This requires the placement of an incision either right at the hairline or back in the temporal scalp. Either approach requires some tissue dissection and excision for its effect.
Trying to get the more distant cheek tissue lifted through the same identical incision is more challenging because it is an area further away than that of the brows. This falls into the basic principle of the further away the pull area is from the target the less effective it is. Unless a hairline incision is used that extends low in the temporal area concomitant cheek lifting will require use of additional dissection techniques in the subtemporal or lower eyelid areas.
I would need to see pictures of you to better determine how temporal/cheek lifting would be done and what type of result you is seeking….before a cost of the surgery can be provided. There are too many variables here just to just guess.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, 5 months ago I had jaw implants. I feel that the jaw muscles are a bit bulky and I’d like to get Botox to make them slimmer and more chiseled. Is there a legitimate risk of the Botox infecting the implants? I read one of your recent articles regarding placing filler on cheek implants and you recommended that a cannula be used to avoid injecting into the implant pocket. Are there any similar guidelines for infecting Botox into the jaw muscles?
A: Any time you place a needle through the skin and inject anything near an implant that is always some risk of causing an infection. Botox nor jaw implants makes that any different. While the risk is probably low, it can never be zero. Unlike injectable fillers Botox injections have to be done by a needle not a cannula.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Two months ago I had infraorbital rim implants that extended into the mid face/cheek. The augmentation was only about 1.5-2mm for most of the cheek and about 3mm for the under eye area. I’m not happy with them and intend to get them removed.
Beside for not liking how they look, there are two other issues I have:
1) my smile looks distorted. The upper lateral areas near my eyes seem pretty expressionless, and my lower cheeks look off from a 45 degree angle (almost like a little ball sticking out)
2) my midface just feels stiff. Especially the upper area, it just feels like my facial muscles aren’t as soft/versatile as before.
So my questions are:
1) are my above concerns valid? Essentially, have you ever seen them?
2) after getting the implants removed, will my smile return to the way it was before?
3) is it possible for there to be cheek sagging even with the implants in place? The logic in thinking is because the soft tissue is separated from the bone, perhaps it doesn’t always reattach properly even when the implants are there? Especially because silicone implants are slippery and maybe the soft tissue won’t adhere to them the same way it adheres to bone?
4) considering I’m in my mid twenties and only had around 2 mm of augmentation of the implants will only be in place a few months before removal, would you anticipate I will avoid complications associated with implant removal?
A: In answer to your infraorbital-malar implant postoperative questions:
1) Cheek implants are well known to cause the temporary midface stiffness and smile distortions that you have described when put in through the mouth. Infraorbital-malar implants placed through lower eyelid incisions, however, do not in my extensive experience.
2) If the implants are the cause of the smile distortion then removing them, presumably, would be the solution.
3) The elevated cheek soft tissues never reattach as they can’t to a smooth surfaced implant. They are merely held there by the implant’s volumetric displacement. This is the concept of ‘soft tissue float’ in implants.
4) Regardless of the thickness of augmentation the detachment of the soft tissues and the implant’s footprint are the same. You are hoping that a thinner implant has a lower risk of cheek sagging after removal than a thicker one….which is a hope that does not have a sound biologic basis.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Thanks for doing the imaging on my potential shoulder width reduction procedure. From the picture it looks like so much change. But I have the following questions.
If the clavicle is cut, will there be any backbone issues as I have to always have the shoulders moving forward? Will it not create a structural stress on my back in the future? How will my shoulder blades adjust to this pulling forward? Will it impact my range of motion?
A: As I discussed with your husband at length on the virtual consultation and to answer these questions to you directly:
1) Clavicle shortening of 2.5cms per side does not cause any spine or shoulder joint dysfunction. To potentially create such dysfunction it has been shown that it takes greater than 30% reduction in clavicle length to do so. With an average female clavicle length of around 14cms and a reduction of 2.5cms, this is only an 18% change in clavicle bone length….enough to make a visible difference in shoulder width but not enough to cause shoulder joint dysfunction.
2) The clavicle shortening is 90% horizontal reduction and 10% forward movement. Thus their is a very minimal anterior rotation which does not cause a substantial pulling of the shoulders forward.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I saw an article on your website wherein you discuss an orbital floor implant of hydroxyapatite cement. I was wondering if this is something you still do.
I ask because I initially underwent a bridge-of-bone canthopexy with a lower lid skin pinch blepharoplasty. In other words: the canthus of both eyes was secured subperiosteally through a drill hole in the lateral orbital rim. Unfortunately the canthus of each eye was mispositioned thereafter.As a result I underwent a revision bridge-of-bone canthopexy but the
lateral canthus of each eye still seems to be mispositioned. The canthus is placed so lateral that it is removed from the eyeball and there is a gap in between the eyeball and the lower eyelid . In addition the lower lashline seems to be too long vertically (there is a horizontal enlargement of the palpebral fissure), and thus the lower eyelids are a bit droopy. As a result I suffer from dryness and itching eyes. Frankly the result looks rather unnatural to me also.
I was recommended an orbital floor implant since my eyes are deep set, and it was thought an orbital floor implant could resolve some of my issues at the canthal area. After seeing your article about an hydroxyapatite orbital floor implant this raised my interest. Is this something you still perform, and if so, would you potentially consider me a candidate for such bilateral surgery or not?
A: Thank you for your inquiry, sending your picture and detailing your surgical history and current lower eyelid concerns. While I perform a wide variety of orbital procedures, including orbital floor augmentation with hydroxyapatite and custom made implants, these procedures do not seem to be appropriate to improving your lower eyelid malposition in which the lower eyelids lack good apposition against the eyeball due to vertical lower lid shortness and outer corner malposition. While I don’t know exactly how your prior canthoplasty procedures were performed (I know what you said they did) or whom recommended an orbital floor implant for your lower eyelid concerns, trying to bring your eyeball up and forward a bit, in and of itself, would exacerbate your current problems. Orbital floor augmentation may or may not be part of the solution but, more importantly, lower eyelid lengthening with spacer grafts (particularly in the right eye) and better position of the eye corner would be what would be the standard and accepted approach to get your eyelids up and in better position back against the eyeball. That is the key in relieving your eye symptoms and appearance.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I wanted to know if I were to get a hair transplant in the same month as these skull and facial surgeries we were planning, would it be better to get that before or after these other surgeries? Or does it not matter? I figured the incisions would be in mostly different places but I wanted to make sure.
A: When it comes to hair transplantation, that causes by itself a lot of facial swelling and the nature of the hair rafts are tenuous early after the procedure. Thus the prudent approach is to separate these procedures by three months apart of which I would do the hair transplants as the second stage to ensure they are to disrupted by anything from the facial and temporal procedures. They definitely should not be done so close together…that is not good for the best results of either procedure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, About two months ago I had infraorbital-malar implants. It seems most of the swelling is gone (80% or so), but I’m not happy with the results. My doctor tells me recovery takes a full year, but quite frankly I just don’t believe that, and I’ve lost faith that it’ll get better with time and I want to have them removed as soon as possible. Regardless, gambling with a year of my life is harder done than said. I saw a post of yours on Realself where you write that if patients aren’t happy after 6 weeks it’s unlikely their concerns will be resolved with time, and I agree with that.
My main questions are as follows:
1) can the implants be removed after 2 months? The implants were silicone
2) From your experience does the face normally return at least closely to its original state?
3) does removing them early (2-4 months post op) make it more likely for the face to return to its previous state? Because I feel waiting one year as the doctor wants me to may end up distorting my face for good.
4) is there a legitimate concern for facial sagging? I’m concerned that the implant pocket will cause sagging (I’m 26 if it’s relevant). What about scar tissue? Is that likely to change the face?
5) about how long does recovery take for implant removal?
6) how long after removal can I get facial fillers in that area?
7) if my doctor refuses to remove them before a year, can I go to a different doctor?
8) is the cost for removal cheaper than the cost for placing them?
Thanks in advance for the help,
A: In answer to your questions:
1) I think it is a fair statement to say that if patients are unhappy with the outcomes of their facial implants by 6 weeks after surgery, their concerns are rarely resolved by time along and some form of surgery is needed. This is a general statement based one my extensive experience but each case must be assessed individually.
2) Whether the face returns to its original anatomic state, I think that does not occur at the 100% level. The real question is not whether it returns to normal but how come to that can it occur. That is affected by many factors most prominently the size of the implant, how long it has been in and its material composition is.
3) As a general rule removing implants sooner rather than later (as long as one is 100% certain that want them removed), in theory is better for returning the tissues back to normal. But most of the issues that relate to the tissues returning to normal (disruption of osteocutaneous ligaments for their placement and tissue stretch) has already been done by the initial surgery.
4) Sagging is always a concern from any midface implant removal. The best way to prevent such sagging is to performed a cheek lift/fresuspension at the same time as their removal.
5) Implant removal would have a faster recovery than their initial placement.
6) Six months
7) A patient can choose to go to any doctor at any time.
8) Not knowing what your original surgical fee were, I can not say. But since the implant fabrication cost is not needed for their removal that may be less.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am scheduled this summer for a procedure for the removal of an occipital knob on the back side of my skull. Before fully committing to the procedure, I wanted to ask a few questions pertaining to concerns that I have about the operation.
From our consultation and the case studies that you published online, I understand that this is a fairly low-risk procedure. Are there any potential serious implications that could arise from this surgery? I am also concerned about the size of the scar for this operation. I plan on fully shaving my head after the surgery; in your estimation, will the scar be detectable from a few feet away? I understand that the scar size can be variable, but will it appear to be a hairline incision and will it be any wider than two inches? I attached photos of the occipital knob to this message if they may be helpful in gauging the potential size of the scar.
Any information would be greatly appreciated, thank you.
A: In answer to your occipital knob skull reduction questions:
1) The occipital knob is a very thick protrusion of bone which means reducing it entirely still leaves a lot of bone for protection. While I could not imagine it not being very thick bone, the way to absolutely determine if it is indeed as thick as I think it is is to get a 2D CT scan and make measurements.
2) The scalp scar is in the range of 5 cms length and it does heal very well. It is placed in a horizontal skin crease if one exists which in your case would be at the bottom of the knob. I can not say whether it will heal so well that it would be undetectable from a few feet away. But I have yet to have a male patient comment on that they found the scar unacceptable.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, I have been looking to have chin surgery for a while now. My chin is my biggest insecurity. I never smile due to the way my chin pulls down when I smile. I also dislike the dimple in my chin and how wide my chin looks when I smile.
A: Thank you for your inquiry, sending your pictures and detailing your concerns. You have two specific soft tissue chin concerns, 1) hyperdynamic chin ptosis and 2) a vertical chin cleft. They may be anatomically related as a vertical chin cleft occurs due to a midline soft tissue deficiency. For improvement/correction a submental approaches needed as the size of the chin pad must b reduced and the chin cleft managed by a muscle repair in your case. Such soft tissue chin repairs, while not technically challenging to perform, are difficult to predict the outcomes since surgery is done in a static setting while your chin issues mainly appear with dynamic motion. (smiling)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a big complex with my head shape because my head is too wide. When I go a Korean plastic surgery hospital the doctor said most part of side head is bone, there is very slim muscle over the ear. Is that true that there is 7mm to 9mms tmuscle hickness above the ear??
A: In my extensive experience with temporal reduction surgery, most men particularly Asian males, have very thick temporalis muscle in the location above the ears. It is usually in the 7 to 9mm thickness range and sometimes even thicker. However the best way to determine the muscle:bone composition ratio of the side of the head is a CT scan. By looking at how much the thickness of the muscle makes up the sides of the head this will help you to determine if temporal reduction surgery is worth it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Would this mess on the side of my mouth be correctable without a facelift? Just an incision beside mouth? I had filler placed there over a year ago and ever since it looks terrible. I have also had the area melted with devices and I am left like this. I’d take a scar any day over this mess. Thank you.
A: Thank you for your inquiry and sending your picture. With the development of perioral folds I would expect any treatment that involved adding volume (fillers) or skin tightening/fat reduction efforts to merely exaggerate the problem. This is a surgical issue that requires either direct or indirect tissue excision/rearrangement. Even though it is an indirect approach, there is no doubt that a lower facelift is the superior approach to trying to smooth out this area by distant tissue excision and skin pull and is also scar free by the mouth area. However there is a direct approach which is an elliptical tissue excision placed above the perioral folds along the line of the nasolabial fold. (see attached image) It typically is reserved for much older patients who have a very deep nasolabial fold anyway which is the equivalent of a pre-existing scar. Bit it can be done on anyone if they are motivated enough to want to avoid a facelift and can accept the scars.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Greetings, do you by any chance offer cranioynostosis treatment in adults, 19 years old to be specific. I have lived with sagittal craniosynostosis my whole life and I want to get it treated.Please refer me to someone that can perform this procedure if it is not in your field.
A: Almost 100% of the time cranial vault surgery is not done in adults due to the increased thickness of the bone and the magnitude of the surgery. Young children have thin pliable bone and a growing brain to help shape it. In adults we greet the effects of sagittal synostosis used on the aesthetics of it not through craniotomies.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I need this procedure. Can a custom skull implant be made that creates a square shape without increasing the height of the head?
 A: Creating a more square-shaped head requires a custom skull implant that elevated the lateral bony temporal line. While such an implant will cross the sagittal midline of the head it would do so by only adding about 2 to 3mms of height in the middle…which I would call not really substantially increasing the height of the head.
A: Creating a more square-shaped head requires a custom skull implant that elevated the lateral bony temporal line. While such an implant will cross the sagittal midline of the head it would do so by only adding about 2 to 3mms of height in the middle…which I would call not really substantially increasing the height of the head.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Please find attached photos of my face at anterior, oblique and profile angles.
I’m interested in custom paranasal silicone implants to address retrusion in the Lefort 2 area and general lack of definition in my midface. I’m hoping to achieve 5-6mm with paranasal implants.
I’ll be looking into dental veneers down the road to project the teeth out as much as possible as well.
I’m aware that down the road I’ll need implants to address retrusion in the tear trough area too, and other work, but would like to start with the paranasals for now.
I’ve also attached photos of my “ideal” female faces where the mid and lower face areas are very well projected (even though I am aware my lower face is structured very differently to theirs.)
Could you please advise on what the cost of custom paranasal implants, including all surgical costs, would be?
Many thanks.
A: Thank you for your inquiry and sending all of your pictures. The best way to think about your implant design is to look at a typical Asian midface implant that addresses the whole midface retrusion issue and then decide how to reduce it if so desired. I have outlined with the purple lines what would be considered the footprint off the premaxillary-paranasal component of it. Assuming that is the basic design of what you need/desire, my assistant Camille will pass along the cost of the surgery to you later today.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in Vertical Orbital Dystopia surgery obj my right eye. However, there is concern involved, as I have to put in eye drops. Here are the names of the drops:
Vital Tears Eye Drops
AzaSite Eye Drops
Xiidra Eye Drops
Retaine Eye Drops.
These are all for dry eye purposes.
A:Those eye drops are all used to treat dry eye syndrome (keratoconjunctivitis sicca) which I assume this is present in both eyes and not just the vertical orbital dystopia side. But even so that does present some concerns about aggravating that condition with any type of procedure on the eyelids in which their position up against the eyeball is surgically manipulated. I would have to have some input from your ophthalmologist who put you on these medications to better determine the risk of symptomatic aggravation with any orbital surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, One thing that bothers me is the fact that I don’t have hollow cheeks like a lot of models do. Why is this, and how could I get that as well as just get a more angular facial structure overall? I have heard that thick skin tissue plays a part, not sure if that is the case for me?
Best regards.
A: Thank you for sending your pictures. While thicker skin does play a major role in how well the facial bones are seen, you still have some room for improvement in changing some of your facial structure. The two areas that strike me as the most important for you are buccal lipectomies (for hollow cheeks) and jaw angle augmentation. (for more angular facial structure) n This would enhance the already largely good facial bone structure you already have.
Dr. Barry Eppley
Indianapolis, Indiana