Jawline Reshaping
Jawline Reshaping Surgery

 The lower third of the face is dominated by the jawline which extends from one jaw angle around a convex arch (chin) to the other jaw angle. It actually covers the largest surface area of any facial bone and is responsible for more of the facial appearance than any other facial structure. Aesthetically the chin typically leads the way. However, the jaw angles located at the back often play an equally important aesthetic role and occupy more of the jawline due to their paired presence.
The lower third of the face is dominated by the jawline which extends from one jaw angle around a convex arch (chin) to the other jaw angle. It actually covers the largest surface area of any facial bone and is responsible for more of the facial appearance than any other facial structure. Aesthetically the chin typically leads the way. However, the jaw angles located at the back often play an equally important aesthetic role and occupy more of the jawline due to their paired presence.
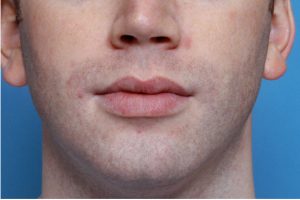
Well-defined chin and jaw angles convey a stronger facial appearance whereas weak chins and jaw angles are perceived less favorably. Weaker chins and an ill-defined jawline often makes the neck appear shorter and fuller with an obtuse neck angle and less distinction between the lower face and neck. Making the jawline more defined is often a combination of either a ‘three corner’ approach (separate chin and jaw angle augmentation) or a complete or total jawline effort. While males used to dominate patients seeking jawline augmentation, females are becoming more commonplace today.
Conversely, a large lower jaw can be disproportionate large compared to the rest of the face and can masculinize a female face. Jaw reductions have become popular today because of V-line surgery which was initially developed in Asia for the very common appearance of large square lower jaws in both women and men. In the U.S. jaw reductions are primarily requested by females and V-line reduction procedures must be often modified for application to the Caucasian face to prevent an over reduced result.
JAW ANGLE IMPLANT AUGMENTATION
Augmentation of the lower face by chin implants has a long history and remains as the initial and still most commonly performed aesthetic facial bone augmentation procedure. But the chin represents only one third of the surface area of the entire jawline that can be augmented. Aesthetic appreciation for the rest of the jawline, primarily the jaw angle areas, has come into focus more recently as an important part of an attractive and youthful face for both men and women.
While jaw angle implants have been commercially available for over twenty five years, they have largely been neglected both in clinical practices and in the medical literature. Newer jaw angle implant styles, a better understanding of the anatomy of the jaw angle region and improvement in surgical techniques allows this type of aesthetic jaw implant to be more successfully used today.
Jaw Angle Aesthetics
The value of a defined and more prominent jaw angle has long been recognized as an attractive male facial feature. By definition a strong male jawline includes a good chin and visible jaw angles. Unlike the chin, where a quantitative assessment of its desired projection and vertical length has long been established, no such specific numerical measurements exist for the jaw angle as it is not a pure profile structure. It is a visible facial landmark that is bounded by the preauricular region in front of it, the submandibular tissues beneath and the retroauricular fossa posteriorly.
But some aesthetic standards are known and certain general facial proportional criteria have been described. A good jaw angle has been defined as one that sits well below the ear, looks long and low in profile and has an angle less than 105 degrees. In the front view its bigonial width should be equal to bitemporal width and just slightly less than bizygomatic width. The soft tissue gonion should be distinctly more lateral than the lateral tissue plane of the neck. And in profile there should be adequate ramus height and a distinct body to ramus transition.
 A more recent study has looked critically at desired male jaw angle aesthetics based on survey results and quantitative measurements. Their findings were that the ideal intergonial width in men approximates the inter-zygomatic width. The inclination of the jawline in the frontal view is parallel to a line extending from the lateral canthus to the ipsilateral ala. The jaw angle should ideally be at the height of the oral commissure in the frontal view and no lower than the lower lip border. The gonial angle (formed by the intersection of the posterior and inferior ramus borders) is ideally at 130 degrees. The angle between the posterior mandibular border and Frankfort horizontal should measure 65 to 75 degrees.
A more recent study has looked critically at desired male jaw angle aesthetics based on survey results and quantitative measurements. Their findings were that the ideal intergonial width in men approximates the inter-zygomatic width. The inclination of the jawline in the frontal view is parallel to a line extending from the lateral canthus to the ipsilateral ala. The jaw angle should ideally be at the height of the oral commissure in the frontal view and no lower than the lower lip border. The gonial angle (formed by the intersection of the posterior and inferior ramus borders) is ideally at 130 degrees. The angle between the posterior mandibular border and Frankfort horizontal should measure 65 to 75 degrees.
 While this study establishes some guidelines for jaw angle shapes for men, no such information for women exists or has been similarly studied. It has only been more recent that the aesthetic value of the jaw angles in women has become more significant. This can readily be appreciated by simply looking at some prominent female news anchors and celebrities as well as women in commercials and ads. The value of a well defined female jawline is an unmistakable presence. The ideal female jaw angle shape and aesthetic goals are, in my experience, somewhat different from men and primarily focus on less jaw angle width.
While this study establishes some guidelines for jaw angle shapes for men, no such information for women exists or has been similarly studied. It has only been more recent that the aesthetic value of the jaw angles in women has become more significant. This can readily be appreciated by simply looking at some prominent female news anchors and celebrities as well as women in commercials and ads. The value of a well defined female jawline is an unmistakable presence. The ideal female jaw angle shape and aesthetic goals are, in my experience, somewhat different from men and primarily focus on less jaw angle width.
In the end, however, patients may want jaw angle augmentation that may or may not fall within these aesthetic standards. This is where the role of preoperative computer imaging is critical in determining what type of change the patient prefers.
Jaw Angle Implant Selection
 The current commercial types of jaw angle implants available are of two types, lateral widening and vertical lengthening. In reality each type also have a bit of the other dimension as well. A widening jaw angle implant can provide a very modest lengthening effect and the vertical lengthening style always provides some width increase. But the dominant effect lies in its style description.
The current commercial types of jaw angle implants available are of two types, lateral widening and vertical lengthening. In reality each type also have a bit of the other dimension as well. A widening jaw angle implant can provide a very modest lengthening effect and the vertical lengthening style always provides some width increase. But the dominant effect lies in its style description.
In selecting the proper jaw angle implant style for a patient, the key is whether a normal or high jaw angle location exists. Technically this is determined by whether a normal or increased mandibular plane angle exists which is primarily a.radiographic/cephalometric assessment While x-rays may help in making that determination, a clinical exam is almost always critical. This is because the natural shape of the jaw angle in Caucasians frequently bends inward. Thus a patient can appear to have a high jaw angle when, in reality, it has adequate vertical length and really lacks width as the inward bend makes it look ‘missing’.
Many men have a decent jaw angle length but lack width and the lateral widening style is a good choice for them. In the high jaw angle patient an inadequate jaw angle length exists and the vertical lengthening style is a better implant choice.

 The historic jaw angle implant design mainly provides width with a minimal vertical lengthening effect created by the roll of the overlying soft tissues in a more outward direction. This is a good choice for the patient with a low or more normal jaw angle length and normal to low mandibular plane angle.
The historic jaw angle implant design mainly provides width with a minimal vertical lengthening effect created by the roll of the overlying soft tissues in a more outward direction. This is a good choice for the patient with a low or more normal jaw angle length and normal to low mandibular plane angle.

 Some men who seek jaw angle augmentation have a high jaw angle location and a steep mandibular plane angle. While some width of the jaw angles may be desired, it is the addition of vertical length that makes the biggest difference in jawline shape improvement. Newer jaw angle implant styles are now available that can create this vertical lengthening effect.
Some men who seek jaw angle augmentation have a high jaw angle location and a steep mandibular plane angle. While some width of the jaw angles may be desired, it is the addition of vertical length that makes the biggest difference in jawline shape improvement. Newer jaw angle implant styles are now available that can create this vertical lengthening effect.

 While men get jaw angle implants in far greater numbers than women, female jaw angle implant surgery is becoming increasingly more common. Driven by the prominent jawlines of female celebrities and models, the aesthetic benefits of a well defined jawline in women are being realized. Some females desire a longer and more prominent jaw angle which can be achieved by vertical lengthening jaw angle implants. This type of jaw angle change is not to be confused with those men who seek much greater flare and width to their jaw shape.
While men get jaw angle implants in far greater numbers than women, female jaw angle implant surgery is becoming increasingly more common. Driven by the prominent jawlines of female celebrities and models, the aesthetic benefits of a well defined jawline in women are being realized. Some females desire a longer and more prominent jaw angle which can be achieved by vertical lengthening jaw angle implants. This type of jaw angle change is not to be confused with those men who seek much greater flare and width to their jaw shape.
In some cases no standard jaw angle implant style or size is adequate to meet the the patient’s aesthetic needs. Be aware of pre-existing jaw angle asymmetries from prior surgeries (e.g., sagittal split osteotomies) or natural development and desired aesthetic outcomes for which standard implants may have no chance to achieve a favorable outcome. This is where the use of custom designed jaw angle implants have a very useful role. They may be more costly up front but one revision from using failed standard implants will more than offset those additional costs.
TOTAL JAWLINE AUGMENTATION
Total jawline augmentation can be done by several techniques, two of which consist of implants and one involving the cutting and moving part of the lower jaw bone. Synthetic jawline augmentation can be done using standard or custom implants. Autologous jawline augmentation can be done using the chin wing osteotomy technique.
The Three Corner Technique (Standard Chin and Jaw Angle Implants)
 The combination of standard chin and jaw angle implants comprises the historic and still commonly used method to a more complete jawline augmentation. It has the advantages of a lower cost and shorter time to surgery with off-the-shelf standard implant designs. This approach can be particularly effective when modest chin and jaw angle augmentations are needed, a completely linear effect between the chin and jaw angles is not needed or of high importance and no significant natural jaw asymmetries or prior jaw bone surgeries have been done.
The combination of standard chin and jaw angle implants comprises the historic and still commonly used method to a more complete jawline augmentation. It has the advantages of a lower cost and shorter time to surgery with off-the-shelf standard implant designs. This approach can be particularly effective when modest chin and jaw angle augmentations are needed, a completely linear effect between the chin and jaw angles is not needed or of high importance and no significant natural jaw asymmetries or prior jaw bone surgeries have been done.
Its major disadvantage is that this requires the placement of three independent implants that are not connected…which is associated with a higher risk of implant malposition. (the orientation of one implants is aided by how the others are positioned)
Wrap Around Custom Jawline Implants
 While standard chin and jaw angle implants enhance the front and back prominences of the lower jaw, they are not connected. (the intervening bone between them remains ‘deficient’) When piecing together standards chin and jaw angle implants, there may be some slight overlap between their edges but this does not constitute a complete or total jawline augmentation. While the use of standard chin and jaw angle implants can work for some patients for a satisfactory lower facial augmentation result, the linear connectivity of a custom jawline implant provides superior aesthetic results. This is of particular interest in men who want to have an overall stronger and/or more defined jawline. It also is of interest for women who seek a linear jawline look that is tapered frontally but with a distinct, altbough not unduly wide, jaw angle appearance.
While standard chin and jaw angle implants enhance the front and back prominences of the lower jaw, they are not connected. (the intervening bone between them remains ‘deficient’) When piecing together standards chin and jaw angle implants, there may be some slight overlap between their edges but this does not constitute a complete or total jawline augmentation. While the use of standard chin and jaw angle implants can work for some patients for a satisfactory lower facial augmentation result, the linear connectivity of a custom jawline implant provides superior aesthetic results. This is of particular interest in men who want to have an overall stronger and/or more defined jawline. It also is of interest for women who seek a linear jawline look that is tapered frontally but with a distinct, altbough not unduly wide, jaw angle appearance.


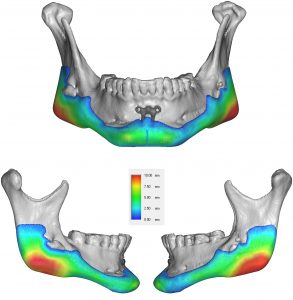
 The design of a custom jawline implant takes into consideration seven (7) different dimensions of the chin and jaw angles as well as the shape and thickness of the connection across the body of the mandible. While there is no exact science in determining the exact size and shape the implant should have to meet the patient’s aesthetic desires, it is important to be aware of the effects of an implant that covers such large bony surface area. With typical custom jawline implant volumes in the 14 to 18ccs range one must be vigilant to avoid creating an oversized implant design.
The design of a custom jawline implant takes into consideration seven (7) different dimensions of the chin and jaw angles as well as the shape and thickness of the connection across the body of the mandible. While there is no exact science in determining the exact size and shape the implant should have to meet the patient’s aesthetic desires, it is important to be aware of the effects of an implant that covers such large bony surface area. With typical custom jawline implant volumes in the 14 to 18ccs range one must be vigilant to avoid creating an oversized implant design.
A custom wrap-around jawline implant is typically inserted through three separate incisions. Bilateral intraoral posterior ascending ramus incisions combined with an anterior submental skin incision provide adequate access for creating the complete inferolateral subperiosteal pocket dissection. Based on the size and material composition of the implant it may be able to inserted as a single piece implant or may need to separated into three or four pieces for placement. Custom implants are available in high durometer solid silicone, PEKK, porous polyethylene or titanium
Bony Jawline Augmentation (The Chin Wing Osteotomy)
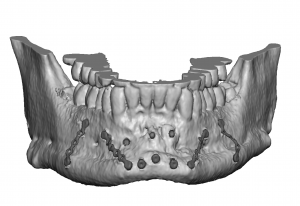
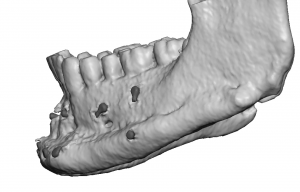 The chin wing osteotomy is a method to provide some augmentation to most of the jawline in an autologous (using your own bone) fashion. It is a modification of the classic sliding genioplasty with the back end of the osteotomy going as far back as the tip of the jaw angle but staying below the course of the inferior alveolar nerve in the bone. The large u-shaped bone segment is then brought forward and down to create a combined forward, vertical and widening effect of the jawline. By the nature of the bone cut and how the bone is moved it can not provide any significant dimensional changes to the jaw angle area. (thinnest part of the bone cut) The bone cut often does go all the way through the entire jaw angle area.
The chin wing osteotomy is a method to provide some augmentation to most of the jawline in an autologous (using your own bone) fashion. It is a modification of the classic sliding genioplasty with the back end of the osteotomy going as far back as the tip of the jaw angle but staying below the course of the inferior alveolar nerve in the bone. The large u-shaped bone segment is then brought forward and down to create a combined forward, vertical and widening effect of the jawline. By the nature of the bone cut and how the bone is moved it can not provide any significant dimensional changes to the jaw angle area. (thinnest part of the bone cut) The bone cut often does go all the way through the entire jaw angle area.
Its main benefit is that it is an autologous operation whose only implants are the numerous small titanium plates and screws used for fixing the bone in its new position. Its disadvantage is that it has a limited 3D effect at the jaw angle area and the outer contour of the newly created chin/jawline is going to be similar to what it was initially…just more of it. But in the properly selected patient who prefers an autologous procedure and can accept the limitations of the jawline dimensional changes, this is a good operation.
Soft Tissue Jaw Angle Implants
One of the aesthetic complications of any form of jaw angle implant augmentation is loss of complete muscle coverage over the implant. This is most commonly known as masseteric muscle dehiscence or implant reveal. It can occur from either loss of a competent muscular skin around the implant during placement or if the implant design exceeds the limits of where complete muscle coverage can occur. Either cause creates an adverse contour change over the jaw angles where a soft tissue muscle bulge is seen above the angle of the implant. (there is no functional problem if it occurs)


 Treatment of a soft tissue contour deficiency over the jaw angle region can be done by efforts at muscle repositioning, injectable fillers or fat injections. If these fail to provide a sustained contour improvement implant augmentation can be considered. Option include thick Alloderm grafts, ePTFE sheets or ultrasoft silicone implants. All three implantable options are done through a very small external skin incision placed either right at the back of the jaw angle or around the base of the earlobe. These small incisions heal extremely well with a negligible scar. As a general rule, small contour jaw angle defects may be treated with Alloderm or ePTFE while large contour defects are more effectively treated by larger ultrasoft silicone implants.
Treatment of a soft tissue contour deficiency over the jaw angle region can be done by efforts at muscle repositioning, injectable fillers or fat injections. If these fail to provide a sustained contour improvement implant augmentation can be considered. Option include thick Alloderm grafts, ePTFE sheets or ultrasoft silicone implants. All three implantable options are done through a very small external skin incision placed either right at the back of the jaw angle or around the base of the earlobe. These small incisions heal extremely well with a negligible scar. As a general rule, small contour jaw angle defects may be treated with Alloderm or ePTFE while large contour defects are more effectively treated by larger ultrasoft silicone implants.
JAW REDUCTION
Jaw reduction is a generic term for a diverse number of lower facial reshaping procedures. Often lumped into one general category, the reality is that a variety of bone and muscle reshaping procedures are available to create a lower jaw that appears more narrow or slimmer. While these jaw reduction procedures are done for largely an aesthetic slimming effect, each technique differs in the specific dimensional changes that are created in the lower face. The two general types of jaw reduction have two different tissue targets, muscle and bone.
Masseter Muscle Reduction
The masseter muscle is a large soft tissue structure that is stretched out between the zygomatic arch (origin) and the bony jaw angle. (insertion) It actually has two heads, superficial and deep. It is the superficial head of the muscle that reaches all the way down and attaches to the inferolateral surface of the bony jaw angle. The deep head is actually thicker and inserts much higher onto the upper ramus near the coronoid process. Thus the thickest part of the muscle is at the mid ramus where the two heads overlap, not down lower around the bony jaw angle.

 When the masseter muscle is overly enlarged due to natural congenital size or hypertrophied due to over activity (e.g., chronic clenching or bruxism) it can be treated non-surgically with Botox injections. (or Dysport or Xeomin) This works by causing a reduction in the size of the muscle fibers which reduces the thickness of the muscle. This reduction occurs at the superficial head of the muscle over the bony jaw angle…which is also the safest place for injection therapy to avoid the buccal branches of the facial nerve which lie further north. The effect of the muscle reduction is usually seen by about three weeks after an injection treatment and will last about 3 months when the size of the muscle slowly returns. The minimum injected drug dose is 25 units per side but often doses of 35 to 50 units per side are needed. In some patients with enough Botox treatments the reduction in the size of the masseter muscles may be more long lasting or even permanent….but this is the exception and does not commonly occur.
When the masseter muscle is overly enlarged due to natural congenital size or hypertrophied due to over activity (e.g., chronic clenching or bruxism) it can be treated non-surgically with Botox injections. (or Dysport or Xeomin) This works by causing a reduction in the size of the muscle fibers which reduces the thickness of the muscle. This reduction occurs at the superficial head of the muscle over the bony jaw angle…which is also the safest place for injection therapy to avoid the buccal branches of the facial nerve which lie further north. The effect of the muscle reduction is usually seen by about three weeks after an injection treatment and will last about 3 months when the size of the muscle slowly returns. The minimum injected drug dose is 25 units per side but often doses of 35 to 50 units per side are needed. In some patients with enough Botox treatments the reduction in the size of the masseter muscles may be more long lasting or even permanent….but this is the exception and does not commonly occur.
There are also other minimally invasive treatments for masseter muscle reduction which are radiofrequency (RF) ablation treatments. By placing electrodes through the oral mucosa inside the mouth and onto the inner surface of the muscle focal areas of muscle necrosis occur. Long term results show that it produces a more pronounced masseter muscle reduction as well as a permanent one compared to Botox injections. But such radio frequency treatments are not widely available and require some form of anesthesia to undergo due to associated discomfort during the treatment.
Surgical masseter muscle reduction can also be done but this does not refer to the excision of segments of the muscle. This is generally not a preferred technique of muscle reduction due to the risks of intraoperaive bleeding and the high likelihood of creating external contour irregularities. Very similar to radiofrequency ablation, an incision is made inside the mouth and the inner surface of the muscle is lifted off of the bone. The inner surface of the lower half of the masseter muscle is then treated by direct electrocautery. Like radiofrequency ablation the thermal effects cause muscle necrosis/atrophy.
Bony Jaw Reduction
Bony jaw reduction consists of different techniques in the location and extent of lower facial reshaping than does masseter muscle reduction. Known as jaw shaving, jaw contouring, or most commonly V-line surgery, this collection of procedures removes bone from the length of the lower jaw to change its shape and size. Jaw bone reshaping can be done at the front (chin), back (jaw angles) or both in which different techniques are used to do so.
Chin Reshaping/Reduction

 At the chin the bone can be reshaped using external contour reductions (shaving) through a submental skin incision or by intraoral osteotomies and removal of internal segments of bone. (t-shaped genioplasty) Each chin reduction/reshaping approach has its advantages and disadvantages. But the most important determinant in choosing a procedure is what dimensions of the chin needs to be changed for the desired look. If the chin only needs to be narrowed, with or without vertical shortening, the outer edges (lateral tubercles) can be removed by bone shaving through either an intraoral or submental approach. However if the chin needs to narrowed, advanced and have any vertical lengthening, these 3D changes requires the chin bone to be sectioned into three pieces and put back together with plate and screw fixation. (this is actually the front end of traditional v-line surgery)
At the chin the bone can be reshaped using external contour reductions (shaving) through a submental skin incision or by intraoral osteotomies and removal of internal segments of bone. (t-shaped genioplasty) Each chin reduction/reshaping approach has its advantages and disadvantages. But the most important determinant in choosing a procedure is what dimensions of the chin needs to be changed for the desired look. If the chin only needs to be narrowed, with or without vertical shortening, the outer edges (lateral tubercles) can be removed by bone shaving through either an intraoral or submental approach. However if the chin needs to narrowed, advanced and have any vertical lengthening, these 3D changes requires the chin bone to be sectioned into three pieces and put back together with plate and screw fixation. (this is actually the front end of traditional v-line surgery)
V Line Jaw Reduction/Reshaping

 Posterior jaw reduction involves removal of bone at the jaw angles which is carried forward to either the mid-body of the lower jaw or all the way to the chin. Jaw bone removal can be done either in a partial thickness (shaving or lateral corticotomies) or full thickness excision. (ostectomies) The indications for either technique depends on the natural shape of the bone and what type of reshaping is needed. For patients with very wide and/or vertically long lower jaw angles, a full-thickness of bone is removed in a curved fashion from the jaw angles up to the sides of the chin. This is typically combined with a siding genioplasty with or without a midline segment of chin bone removed for narrowing.This changes the complete shape of the bone not only in width but in length as well. (changes the mandibular plane angle) It produces the most dramatic amount of jaw reduction but also risks over-resection when applied to the wrong type of jaw shape. This is what is done in traditional v-line surgery. It is no surprise that this type of jaw reduction emanates from Asia where the natural shape of the lower jaw is more square and needs full thickness excisions for a significant shape change and a more noticeable narrowing effect. But with the complete loss of the full thickness bony jaw angle comes the risk of some soft tissue sag in the lower face. Given that most of v line surgery is done in younger patients their more elastic skin and no natural skin laxity makes this risk low. But in older patient v-line surgery may need to be combined with a lower facelift either during or after the jaw reduction.
Posterior jaw reduction involves removal of bone at the jaw angles which is carried forward to either the mid-body of the lower jaw or all the way to the chin. Jaw bone removal can be done either in a partial thickness (shaving or lateral corticotomies) or full thickness excision. (ostectomies) The indications for either technique depends on the natural shape of the bone and what type of reshaping is needed. For patients with very wide and/or vertically long lower jaw angles, a full-thickness of bone is removed in a curved fashion from the jaw angles up to the sides of the chin. This is typically combined with a siding genioplasty with or without a midline segment of chin bone removed for narrowing.This changes the complete shape of the bone not only in width but in length as well. (changes the mandibular plane angle) It produces the most dramatic amount of jaw reduction but also risks over-resection when applied to the wrong type of jaw shape. This is what is done in traditional v-line surgery. It is no surprise that this type of jaw reduction emanates from Asia where the natural shape of the lower jaw is more square and needs full thickness excisions for a significant shape change and a more noticeable narrowing effect. But with the complete loss of the full thickness bony jaw angle comes the risk of some soft tissue sag in the lower face. Given that most of v line surgery is done in younger patients their more elastic skin and no natural skin laxity makes this risk low. But in older patient v-line surgery may need to be combined with a lower facelift either during or after the jaw reduction.

 A more conservative form of posterior jaw reduction is by shaving or by removing the outer layer of bone over the jaw angle area with or without removing the actual jaw angle point. This reduces the width of the jaw but not its vertical length. The jaw angle shape is kept intact but it becomes less wide. The amount of jaw reduction change is less dramatic but is more aesthetically appropriate for jaw shapes that are not unduly wide or flared and doesn’t have a low jaw angle. It is often what is better suited for the patient who has a normal mandibular plane angle and has little risk of resulting in an over resected lower jaw shape. With preservation of vertical jaw angle height there is a much lower risk of skin sag developing afterwards.
A more conservative form of posterior jaw reduction is by shaving or by removing the outer layer of bone over the jaw angle area with or without removing the actual jaw angle point. This reduces the width of the jaw but not its vertical length. The jaw angle shape is kept intact but it becomes less wide. The amount of jaw reduction change is less dramatic but is more aesthetically appropriate for jaw shapes that are not unduly wide or flared and doesn’t have a low jaw angle. It is often what is better suited for the patient who has a normal mandibular plane angle and has little risk of resulting in an over resected lower jaw shape. With preservation of vertical jaw angle height there is a much lower risk of skin sag developing afterwards.
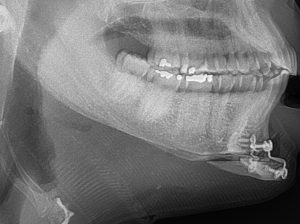
The key to a successful bony lower jaw reduction is to match the technique with the dimensional requirements needed for the desired change. This not only requires preoperative x-rays (panorex, lateral cephalogram or 3D jaw CT scan) but computer imaging to determine what magnitude of jaw reduction change the patient desires. While under- and over resection results can occur, by far the most common revisional jaw reduction patients I see is when too much has been done. This almost always is when traditional v-line surgery has been done leaving the patient with over resected jaw angles and chin that is too narrow or elongated. This can be a function of overly aggressive bone reduction but more commonly occurs because it was not the best technique for the patient’s natural lower jaw shape.
Inferior Border Shave

 One of the least appreciated forms of bony jaw reduction is the inferior border shave. It is almost exclusively done in chin and lower jaw asymmetries where one side of the chin or jawlineis vertically longer. Through a submental approach the inferior border of the longer side is removed to match the height of the lower jaw on the other side if possible. The limit of the inferior border shave reduction is the location of the inferior alveolar nerve in the bone. One can get close by not quite all the way back to the end of the jaw angle through the anterior external submental incision.
One of the least appreciated forms of bony jaw reduction is the inferior border shave. It is almost exclusively done in chin and lower jaw asymmetries where one side of the chin or jawlineis vertically longer. Through a submental approach the inferior border of the longer side is removed to match the height of the lower jaw on the other side if possible. The limit of the inferior border shave reduction is the location of the inferior alveolar nerve in the bone. One can get close by not quite all the way back to the end of the jaw angle through the anterior external submental incision.
Before Jawline Reshaping Surgery
The consideration of any form of jawline enhancement requires a thorough pre-surgical analysis. Because the chin and the jaw angles are “edge” facial features, they are easily viewed on computer imaging technology. Each prospective jawline enhancement surgery patient undergoing chin or jaw angle implants must be assessed with computer analysis to make sure that the predicted facial changes are what the patient desires. Photographs are taken before surgery and computer imaging is provided. This is an essential step in any form of facial implant surgery, particularly in jawline implant surgery.
About Jawline Reshaping – The Operation
Jawline enhancement procedures are performed under general anesthesia as an outpatient procedure. Chin implants are inserted through a very small incision under the chin where the bone is easily reached. Some patients refer an incision-less approach for their chin augmentation and this can be done then from an incision inside the mouth. Jaw angle implants are inserted through incisions inside the mouth so there is no visible scar. Most chin implants and all jaw angle implants are secured into position with permanent small metal screws to prevent the risk of displacement or shifting. Jawline implants are often performed along with other facial structural surgeries such as rhinoplasty and cheek augmentation.
After Jawline Reshaping Surgery
A chin and face strap is almost always used after jawline surgery to control swelling and help the overlying tissues adhere to the implant and bone. After chin implant surgery, swelling is moderate, but there is usually very little if any bruising. Following jaw angle implant surgery, the swelling can be considerable, and some bruising into the neck is not uncommon. Mouth opening will also be stiff for several weeks after surgery. Sutures inside the mouth and under the chin are dissolvable and do not need to be removed.
Chin implants are extremely well tolerated and infection is very rare. Jaw angle implants are equally well tolerated, but they have a slightly higher incidence of infection due to being placed through a mouth incision. All jawline enhancement surgery patients take antibiotics for one week after surgery.
Contact Us
To learn more about jawline enhancement surgery or how you may benefit from jaw surgery, please contact our office to schedule a consultation today. View more of our jaw surgery results in our jawline reshaping surgery before and after photo gallery.
Cost of Jawline Reshaping Surgery
Determined on a case-by-case basis



A detailed description and pictures of your concerns allow for the most informed response.
Disclaimer: By submitting a question, you agree that it may be used for educational purposes. Any identifying details or photos will be removed. Responses are general and not a substitute for medical advice.
North Meridian Medical Building
Address:
12188-A North Meridian St.
Suite 310
Carmel, IN 46032
Contact Us:
Phone: (317) 706-4444
WhatsApp: (317) 941-8237