Ear Reshaping
Ear Reshaping
Barry L. Eppley, MD, DMD, is one of the few plastic surgeons with years of ear reshaping experience helping patients who have protruding ears or congenital or traumatic ear deformities.
EAR ANATOMY
 Small as the ear is on the side of the head, it has a very complex anatomical shape. Filled with various ridges and valleys created by its cartilaginous component, it is a miracle of genetics and embryologic development that it consistently develops with an overall basic shape and form. A normal shaped and positioned ear is inconspicuous, but when it sticks out too far, has a deformed shape or is even partially absent, it becomes a very evident deformity.
Small as the ear is on the side of the head, it has a very complex anatomical shape. Filled with various ridges and valleys created by its cartilaginous component, it is a miracle of genetics and embryologic development that it consistently develops with an overall basic shape and form. A normal shaped and positioned ear is inconspicuous, but when it sticks out too far, has a deformed shape or is even partially absent, it becomes a very evident deformity.
When changing the shape of the ear it is best to think of it as having three ascending levels (concha, antithelical fold and helical rim) which gives it a series of predictable hills (convexities) and valleys. (concavities) supported by the cartilage framework underneath the skin. The only part of the ear that has no cartilage support is the earlobe.
EAR RESHAPING OPTIONS
Protruding Ear Correction (Pinback Otoplasty)
Ears that abnormally stick out (protruding ears) are the most common ear deformity and are a frequent source of embarrassment for many patients and may make one very self-conscious. This is particularly true for children and teenagers… although it is often no less so in adults. One cause of prominent ears is a congenital absence of a natural curve in the ear’s cartilage which causes it to protrude rather than conform to the side of the head. (lack of antihelical fold) Protruding ears may also occur because the bowl (concha) of the ear is too big, driving the external shape of the ear outward. In some cases of protruding ears, it is a combination of both cartilage abnormalities that make the ears stick out.


 Its surgical correction is an ear reshaping procedure called otoplasty which has often been called a ‘pinning back’ of the ears. In this ear procedure, the antihelical fold of the ear is recreated by sutures, the size of the concha reduced or weakened, or a combination of both techniques is used from an incision on the back of the ear. While it is commonly performed in children (can be done as early as two years old) and teenagers, it can be done just as successfully in older adults. There is no upper age limit at which an otoplasty can be successfully performed. The changes that result from otoplasty can be some of the most dramatic of all ear reshaping surgeries.
Its surgical correction is an ear reshaping procedure called otoplasty which has often been called a ‘pinning back’ of the ears. In this ear procedure, the antihelical fold of the ear is recreated by sutures, the size of the concha reduced or weakened, or a combination of both techniques is used from an incision on the back of the ear. While it is commonly performed in children (can be done as early as two years old) and teenagers, it can be done just as successfully in older adults. There is no upper age limit at which an otoplasty can be successfully performed. The changes that result from otoplasty can be some of the most dramatic of all ear reshaping surgeries.
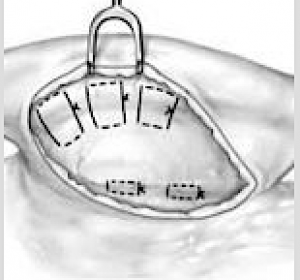
 One of the main techniques used in setback otoplasty surgery is the placement of permanent sutures placed through an incision on the back of the ear to reshape the cartilages. This produces an immediate and dramatic change in ear shape as soon as the sutures are tied down. Such suture placement does not always need to affect the whole cartilage structure of the ear. Some patients need just one or two sutures selecting placed through a very small incision to get the desired change in a ‘mini-otoplasty‘ surgery.
One of the main techniques used in setback otoplasty surgery is the placement of permanent sutures placed through an incision on the back of the ear to reshape the cartilages. This produces an immediate and dramatic change in ear shape as soon as the sutures are tied down. Such suture placement does not always need to affect the whole cartilage structure of the ear. Some patients need just one or two sutures selecting placed through a very small incision to get the desired change in a ‘mini-otoplasty‘ surgery.

 Setback ear reshaping can also be done in select cases by a method known as ‘incisionless otoplasty’. This is a percutaneous method (no incision on the back of the ear) in which permanent sutures are placed to reshape the ear and create an antihelical fold through needle entrances sites. Prior to placing the sutures a needle is used to weaken the cartilage by multiple needle tracks through it. While effective for some patients it has a higher incidence of relapse and asymmetries. To avoid this potential issues I prefer a mini-otoplasty approach which is more reliable.
Setback ear reshaping can also be done in select cases by a method known as ‘incisionless otoplasty’. This is a percutaneous method (no incision on the back of the ear) in which permanent sutures are placed to reshape the ear and create an antihelical fold through needle entrances sites. Prior to placing the sutures a needle is used to weaken the cartilage by multiple needle tracks through it. While effective for some patients it has a higher incidence of relapse and asymmetries. To avoid this potential issues I prefer a mini-otoplasty approach which is more reliable.
Otoplasty Reversal
While the setback otoplasty can bring the ears back closer to the side often head, it is also possible to bring them back too far. Just like ears that can stick out too far (excessive auriculocephalic angle) , it is similarly possible to make them too close to the side of the head. (too small of an auriculocephalic angle) This is most commonly seen in the setback otoplasty patient in which the middle third of the head is pulled back beyond the natural helical rim line and disappears behind the projection of the concha.
 In otoplasty reversal surgery the goal is to restore some of the auriculocephalic angle and create a more visible and smooth helical rim from the front view. To do so it takes a combination of a release of the antihelical fold cartilage from begin the ear and the placement of an interposition graft or some form of a spacer. I have used metal plates and allogeneic rib grafts for the spacer graft.
In otoplasty reversal surgery the goal is to restore some of the auriculocephalic angle and create a more visible and smooth helical rim from the front view. To do so it takes a combination of a release of the antihelical fold cartilage from begin the ear and the placement of an interposition graft or some form of a spacer. I have used metal plates and allogeneic rib grafts for the spacer graft.



 Most otoplasty reversals are not a complete reversal. Rather it is a subtotal reversal to re-establish a more ear shape that looks less pulled back or overdone. Otoplasty reversal can usually be done under local anesthesia through the existing incision on the back of the ear.
Most otoplasty reversals are not a complete reversal. Rather it is a subtotal reversal to re-establish a more ear shape that looks less pulled back or overdone. Otoplasty reversal can usually be done under local anesthesia through the existing incision on the back of the ear.
Earlobe Reductions/Reconstruction
The earlobe occupies a relatively small portion of the ear and is the only part of the ear that has no cartilage. Since it is frequently adorned by variety of metal devices for aesthetic purposes, it is prone to developing a variety of problems due to the easy disruption or stretching of its completely soft tissue composition.. It can develop earlobe tears and lacerations, stretched earlobe tissues (gauging) and pathologic scarring (keloids).



 Since the earlobe has no cartilage and it is just tissue, it is prone to becoming elongated over time due to the effects of ear ring wear and aging. Earlobe ‘rejuvenation’ can be done by shortening and reshaping it through earlobe reduction techniques. Long earlobes can also occur naturally in some patients. But most of the time earlobes do get longer the older we get.
Since the earlobe has no cartilage and it is just tissue, it is prone to becoming elongated over time due to the effects of ear ring wear and aging. Earlobe ‘rejuvenation’ can be done by shortening and reshaping it through earlobe reduction techniques. Long earlobes can also occur naturally in some patients. But most of the time earlobes do get longer the older we get.



 The single most common need for earlobe surgery is to repair a tear from ear rings. This may occur from the ear ring being pulled and tearing through the edge of the earlobe or the ear hole continues to get bigger until it gets close to the edge or actually separates creating the cleft or forked earlobe appearance. Such earlobe tears can occur as a single tear or mutiple tears in patients with double piercings. Either way all such earlobe tears can be repaired under local anesthesia as an office procedure. Earlobes can be re-pierced six weeks after the repair.
The single most common need for earlobe surgery is to repair a tear from ear rings. This may occur from the ear ring being pulled and tearing through the edge of the earlobe or the ear hole continues to get bigger until it gets close to the edge or actually separates creating the cleft or forked earlobe appearance. Such earlobe tears can occur as a single tear or mutiple tears in patients with double piercings. Either way all such earlobe tears can be repaired under local anesthesia as an office procedure. Earlobes can be re-pierced six weeks after the repair.



 Earlobe repair/reconstruction is often need in the gauged ear. Such earlobe surgeries are initiated when the patient decides to remove their gauge devices permanently, the need for an intact earlobe arises due to work requirements or entering the military or the stretched earlobe actually tears. Fortunately the expansion of the earlobe tissues creates the needed tissue to reconstruct an intact and more normal appearing earlobe.
Earlobe repair/reconstruction is often need in the gauged ear. Such earlobe surgeries are initiated when the patient decides to remove their gauge devices permanently, the need for an intact earlobe arises due to work requirements or entering the military or the stretched earlobe actually tears. Fortunately the expansion of the earlobe tissues creates the needed tissue to reconstruct an intact and more normal appearing earlobe.

 One of uncommon cases of a large or elongated earlobe is what can occur after facelift surgery, known as the pixie earlobe deformity. This is the tensing of the facelift has been placed too much emphasis on the skin pull and the tension is transferred to the part of the part that can resist the least…the earlobe which has no cartilage support. In minor cases the earlobe may be repositioned with release and earlobe reshaping But in more major pixie earlobes it require a partial re-do of the facelift to adequately correct.
One of uncommon cases of a large or elongated earlobe is what can occur after facelift surgery, known as the pixie earlobe deformity. This is the tensing of the facelift has been placed too much emphasis on the skin pull and the tension is transferred to the part of the part that can resist the least…the earlobe which has no cartilage support. In minor cases the earlobe may be repositioned with release and earlobe reshaping But in more major pixie earlobes it require a partial re-do of the facelift to adequately correct.
MACROTIA SURGERY (Ear Reduction)
 The large ear typically refers to an ear that is too vertically long. The linear distance between the top of the ear and the bottom of the earlobe is disproportionate in size to other facial features. While the entire ear may be too large overall, surgical reduction techniques focuses on the two areas of the ear where resultant scars are the most aesthetic favorable for ear shortening…the top and bottom 1/3 of the ear.
The large ear typically refers to an ear that is too vertically long. The linear distance between the top of the ear and the bottom of the earlobe is disproportionate in size to other facial features. While the entire ear may be too large overall, surgical reduction techniques focuses on the two areas of the ear where resultant scars are the most aesthetic favorable for ear shortening…the top and bottom 1/3 of the ear.


 At the upper portion of the ear the height can be reduced by a scaphal flap reduction technique. This places the scar inside the helical rim where it is not seen and only has a very small part of the scar crosses the horizontal portion of the middle helical rim. The lower third of the ear is shortened (‘lifted’) by an inferior helical rim reduction technique which places the scar at the favorable location of the bottom of the earlobe. When both methods are combined the vertical length of the ear can usually be reduced by 10 to 15mms. In some patients only the superior or inferior reduction method may be needed.
At the upper portion of the ear the height can be reduced by a scaphal flap reduction technique. This places the scar inside the helical rim where it is not seen and only has a very small part of the scar crosses the horizontal portion of the middle helical rim. The lower third of the ear is shortened (‘lifted’) by an inferior helical rim reduction technique which places the scar at the favorable location of the bottom of the earlobe. When both methods are combined the vertical length of the ear can usually be reduced by 10 to 15mms. In some patients only the superior or inferior reduction method may be needed.



 Macrotia surgery is an effective technique for ear reduction that is typically associated with excellent scar healing that does not detract from the overall ear reshaping result.
Macrotia surgery is an effective technique for ear reduction that is typically associated with excellent scar healing that does not detract from the overall ear reshaping result.
EAR RECONSTRUCTION
The complexity of the ear shape is prone to a highly diverse number of congenital deformities which result in shape malformations of the outer helix (e.g., lop ear, cupped ear, Spock ear, Darwin’s tubercle) to partial or near complete absence of the ear. (microtia) Reconstruction of congenital ear deformities is far removed from most other forms of ear reshaping because of the need to create a partial or complete cartilage framework to support the parts of the ear that are missing combined with methods of skin tissue coverage over it.


 The most severe form of congenital ear deformity its microtia in which the need to harvest rib grafts to fabricate a cartilage framework is the foundation of its reconstruction. Such ear reconstruction is done in early childhood and involves multiple stages to achieve the final result.
The most severe form of congenital ear deformity its microtia in which the need to harvest rib grafts to fabricate a cartilage framework is the foundation of its reconstruction. Such ear reconstruction is done in early childhood and involves multiple stages to achieve the final result.

 Microtia can also be reconstructed using a variety of different synthetic care frameworks made out of either porous polyethylene or ePTFE. The advantages of a preformed framework is the avoidance of harvesting rib grafts and the complexity of hand making a detailed ear framework shape. Very often such ear frameworks produce a better looking ear but do so at a higher risk of infection.
Microtia can also be reconstructed using a variety of different synthetic care frameworks made out of either porous polyethylene or ePTFE. The advantages of a preformed framework is the avoidance of harvesting rib grafts and the complexity of hand making a detailed ear framework shape. Very often such ear frameworks produce a better looking ear but do so at a higher risk of infection.

 The prominence of the ear on the side of the head also makes it prone to traumatic deformities in which part of the ear may be missing from avulsive type injuries. Like congenital ear deformities, reconstruction of parts the ear that are missing from traumatic loss (avulsion) or from irreversible injuries (burns) requires the use of cartilage graft framework fabrication and local tissue flaps and skin grafting for coverage.
The prominence of the ear on the side of the head also makes it prone to traumatic deformities in which part of the ear may be missing from avulsive type injuries. Like congenital ear deformities, reconstruction of parts the ear that are missing from traumatic loss (avulsion) or from irreversible injuries (burns) requires the use of cartilage graft framework fabrication and local tissue flaps and skin grafting for coverage.
Before Ear Surgery
The ears are examined and the form and shape of the ear analyzed. The effectiveness of the procedure can be determined by folding the rim of the ear back and seeing if this gives the desired shape in protruding ear patients. Whether tissue grafts may be needed to reconstruct the ear is determined at this time. Photographs are taken prior to surgery for documentation. Patients should wash their hair the night before surgery.
The Operation
Most ear surgeries are performed as an outpatient under general anesthesia. The otoplasty for protruding ear operation is done through an incision on the back of the ear. The cartilage of the ear is exposed and sutures are placed to provide the proper fold and shape to the ear cartilage. Occasionally, it may be necessary to remove some cartilage to acquire the proper ear shape. When the incision is closed, some skin on the back of the ear may also be removed. A circumferential ear dressing is then applied which is worn for 24 hours after surgery. For those ears that need reconstruction by grafting, the most common areas for cartilage harvesting are the other normal ear or rib grafts for larger reconstruction. (microtia) Skin grafts, if needed, are usually taken from behind the other ear.
After Ear Surgery
Pain is moderate in nature as the ears are sensitive to manipulation. Bruising is very limited although the swelling is more evident. Some bruising and swelling are reduced from the gentle pressure of the head dressing. The head dressing is removed after one week in children and the next day in teenagers and adults. An elastic headband (or ski band) is to be worn at nighttime for several more weeks for protection in the protruding ear patient. The temporary swelling of the ears usually resolves completely in two to three weeks after surgery. The hair may be gently washed when the head dressing is removed. Physical activities such as sports, where the risk of ear trauma exists, should be done cautiously for up to one month after surgery.
Significant complications are exceedingly rare from this procedure. Minor risks include delayed healing of the incisions, infection of the ear cartilage, extrusion of the sutures used to shape the cartilages, and asymmetry in the shape of the ears between the two sides.



A detailed description and pictures of your concerns allow for the most informed response.
Disclaimer: By submitting a question, you agree that it may be used for educational purposes. Any identifying details or photos will be removed. Responses are general and not a substitute for medical advice.
North Meridian Medical Building
Address:
12188-A North Meridian St.
Suite 310
Carmel, IN 46032
Contact Us:
Phone: (317) 706-4444
WhatsApp: (317) 941-8237