Facial Asymmetry
Facial Asymmetry Surgery
Can My Facial Asymmetry Be Fixed?
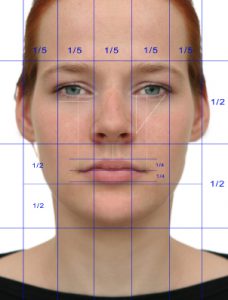 The importance of facial symmetry is well known to have a major influence on how attractive one’s face is. The more symmetric two facial halves are, the more they are perceived as attractive, regardless if one is male or female. Of all the factors that contribute to the judgment of beauty, facial symmetry is typically rated the most important — even though most human faces have some form of asymmetry, which is often referred to as “character.”
The importance of facial symmetry is well known to have a major influence on how attractive one’s face is. The more symmetric two facial halves are, the more they are perceived as attractive, regardless if one is male or female. Of all the factors that contribute to the judgment of beauty, facial symmetry is typically rated the most important — even though most human faces have some form of asymmetry, which is often referred to as “character.”
While some facial asymmetry is acceptable to most people, maybe even desired, significant facial asymmetry can cause distress or even lead to low self-esteem in others. There is no precise quantitative measure of acceptable vs. non-acceptable amounts of facial asymmetry other than how bothersome it is to the patient. Regardless of how it is perceived by others, individual perception of facial asymmetry is the most important determinant of whether surgical correction should be attempted.
Facial Asymmetry Types and Assessment

Facial asymmetries can affect any of one’s facial features. With over twenty distinct features on a face, this creates a wide variety of facial asymmetry presentations. But in my experience in treating facial asymmetry patients, they are very distinct patterns in which they occur. While it can happen that only one anatomic feature is different between the two facial sides, this is the exception and not what normally occurs. Barring traumatic injury or changes from surgical reconstruction, the vast majority of facial asymmetries are developmental in origin.
Looking at the embryologic development of the face and their brachial arch origins with midline merging of the developmental processes, it is actually a miracle that most faces develop with little to no significant asymmetries. In some uncommon cases the developmental aberrations are severe (e.g., hemifacial microsomia) and are what can be termed Craniofacial Facial Asymmetries. These more major facial problems require craniosurgical techniques for reconstruction and are beyond the scope of this discussion.
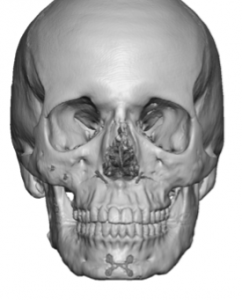
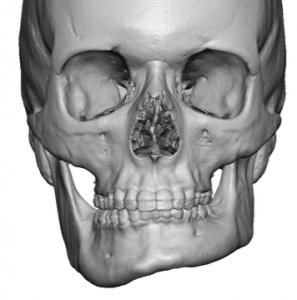
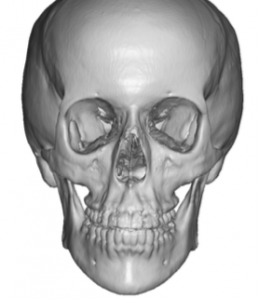
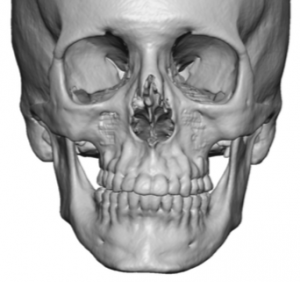
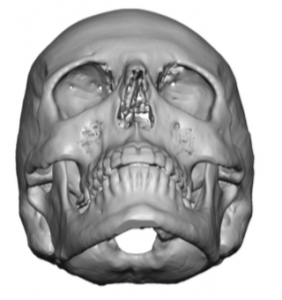
Far more common are the category of Aesthetic Facial Asymmetries, which are much smaller in magnitude than the more severe Craniofacial ones, but share the underlying cause of facial development side differences. (not severe enough to be called malformations) As a result, most aesthetic facial asymmetry problems rarely affect just one facial feature or area. Often it usually affects the whole side of the face from the forehead down to the chin. It usually requires close inspection to see the full extent of the facial involvement. In most cases the asymmetry is caused by underdevelopment (hypoplasia) of one side of the face rather than overgrowth (hyperplasia) of a facial side. Patients may only see the facial feature that is most asymmetric but almost always other feature asymmetries exist. One of the best ways to see the extent of facial asymmetries are 3D CT scans. With the bone as the foundation of most of the external facial features, such scans usually provide meaningful insight into what is seen on the outside.
Because of their developmental origin Aesthetic Facial Asymmetries occur in patterns which can be divided into complete and incomplete types.
 Incomplete facial asymmetries are where just one facial feature is affected. The single most common incomplete facial asymmetry is that of the lower jaw. The upper two-thirds of the face are symmetric but the lower jaw is asymmetric. This may appear as just a deviated chin or the entire one side of the lower jaw is less wide. Or the chin may be straight but one jaw angle is higher and less full. Either way one side of the jaw will be more developed and defined, which the patient typically prefers, and the less developed jaw side needs to be augmented. (at least for men) In some women they may prefer the smaller asymmetric side and then the larger side of the jaw needs to be reduced.
Incomplete facial asymmetries are where just one facial feature is affected. The single most common incomplete facial asymmetry is that of the lower jaw. The upper two-thirds of the face are symmetric but the lower jaw is asymmetric. This may appear as just a deviated chin or the entire one side of the lower jaw is less wide. Or the chin may be straight but one jaw angle is higher and less full. Either way one side of the jaw will be more developed and defined, which the patient typically prefers, and the less developed jaw side needs to be augmented. (at least for men) In some women they may prefer the smaller asymmetric side and then the larger side of the jaw needs to be reduced.
 In rare cases, which start to become closer to lesser forms of Craniofacial Facial Asymmetries, the jaw asymmetry is more severe and actually both sides of the lower jaw are at fault. Closer inspection of other facial features will that the asymmetry does involve other facial features as well albeit to a much lesser degree which may not even be recognized by the patient.
In rare cases, which start to become closer to lesser forms of Craniofacial Facial Asymmetries, the jaw asymmetry is more severe and actually both sides of the lower jaw are at fault. Closer inspection of other facial features will that the asymmetry does involve other facial features as well albeit to a much lesser degree which may not even be recognized by the patient.
Complete facial asymmetries are when the entire side of the face is involved and they typically present in two types, a top to bottom pattern (superior facial asymmetry) or a bottom to top pattern. (inferior facial asymmetry). In both types the most affected facial features are either at the top or the bottom of the face and their degree of involvement fades in severity as one moves away from the more severely affected area.
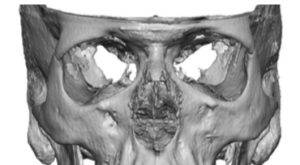 In the superior facial asymmetry, the eyes are seen as the major asymmetric feature. This is easy to see because your first focus on any face is to look at the eyes. It is even more obvious in pictures due to their static nature. The eyes are at two different levels as judged by a horizontal line drawn through the pupils. Almost always the affected side is the lower eye. This is caused by the bones around the eye (orbital box) being lower. As a result everything around the eye is lower. The eyebrow and brow bone is lower, the upper and lower eyelids are lower to properly drape around the eye properly, and the cheekbone is less developed. (flatter) This is also called Vertical Orbital Dystopia and those who have aesthetic forms of it are generally 5mms or less of a horizontal eye level difference. But close inspection of the facial features below it can show a downturned mouth corner/lip deviation, nostril asymmetry or even the entire nose pulled toward that side and lower, a fuller jowl on that side as well as chin/jaw lengthening on the asymmetric side. These lower facial asymmetries may be more modest or very subtle but they are present. But in the superior facial asymmetry the affected facial side is pulled down.
In the superior facial asymmetry, the eyes are seen as the major asymmetric feature. This is easy to see because your first focus on any face is to look at the eyes. It is even more obvious in pictures due to their static nature. The eyes are at two different levels as judged by a horizontal line drawn through the pupils. Almost always the affected side is the lower eye. This is caused by the bones around the eye (orbital box) being lower. As a result everything around the eye is lower. The eyebrow and brow bone is lower, the upper and lower eyelids are lower to properly drape around the eye properly, and the cheekbone is less developed. (flatter) This is also called Vertical Orbital Dystopia and those who have aesthetic forms of it are generally 5mms or less of a horizontal eye level difference. But close inspection of the facial features below it can show a downturned mouth corner/lip deviation, nostril asymmetry or even the entire nose pulled toward that side and lower, a fuller jowl on that side as well as chin/jaw lengthening on the asymmetric side. These lower facial asymmetries may be more modest or very subtle but they are present. But in the superior facial asymmetry the affected facial side is pulled down.
 In the inferior facial asymmetry the lower face is the most serenely affected by chin/jaw deviation or decreased fullness from the other side. The occlusal plane may be level (often because of orthodontic treatment) or even slightly tilted upward on the asymmetric facial side. Similarly the nose will show a nostril that is asymmetric but higher with some slight deviation of the nose. The trend here is that, conversely from a superior facial asymmetry, the affected facial side is pulled up. The other difference is that the eye is either barely affected or will show some slight downward pull but almost never will sit higher than the unaffected side
In the inferior facial asymmetry the lower face is the most serenely affected by chin/jaw deviation or decreased fullness from the other side. The occlusal plane may be level (often because of orthodontic treatment) or even slightly tilted upward on the asymmetric facial side. Similarly the nose will show a nostril that is asymmetric but higher with some slight deviation of the nose. The trend here is that, conversely from a superior facial asymmetry, the affected facial side is pulled up. The other difference is that the eye is either barely affected or will show some slight downward pull but almost never will sit higher than the unaffected side
So while facial asymmetries can involve a wide variety of feature differences between the two sides of the fade (chin/jawline deviation, vertical facial shortening, cheek retrusion, orbital floor/eye displacement, eyebrow lowering, forehead and brow bone protrusion or retrusions and nasal deviations) they generally follow patterns that can be explained by their embryologic development.
Facial Asymmetry Surgery
Facial asymmetry surgery consists of well known operations that are used for different types of aesthetic and reconstructive facial problems. These include operations borrowed from skull, forehead, eyebrow, brow bone, temple, ears, orbital and eyelids, nose, cheeks, lips, jowl, chin, and jawline surgeries. Some of the most common facial asymmetry procedures include:
- Browlift
- Otoplasty
- Rhinoplasty
- Chin Implants
- Facelift/Necklift
- Forehead/Brow Augmentation
- Cheek Augmentation/Reduction
- Buccal Lipectomies/Perioral Mound Liposuction
- Jawline/Jaw Angle Reduction and Narrowing
- Temporal Line Augmentation/reduction
- Eyelid Canthoplasties/Canthopexies
- Orbital Floor/Rim Augmentation
- Jawline Implant Augmentation
- Submental/Neck Liposuction
- Lip/Corner of Mouth Lifts
- Orbital Rim Reshaping
- Bony Genioplasty
- Fat Injections
Browlift
 A low and asymmetric eyebrow can be treated by several types of browlift techniques. But the most common one used would be the endoscopic browlift. This offers an effective but minimal incisional brow elevator method for getting the lower eyebrow more symmetric to the opposite eyebrow.
A low and asymmetric eyebrow can be treated by several types of browlift techniques. But the most common one used would be the endoscopic browlift. This offers an effective but minimal incisional brow elevator method for getting the lower eyebrow more symmetric to the opposite eyebrow.
Brow Bone Reduction
![]() The type of brow bone reduction needed in the vertical orbital dystopia type of facial asymmetry is to raise up the lower edge of the brow bone that is too low. The inferior border of the brow bone is removed through an upper eyelid incision (transpalpebral ) by burring to even out the horizontal levels of the bony brow bones.
The type of brow bone reduction needed in the vertical orbital dystopia type of facial asymmetry is to raise up the lower edge of the brow bone that is too low. The inferior border of the brow bone is removed through an upper eyelid incision (transpalpebral ) by burring to even out the horizontal levels of the bony brow bones.
Upper Eyelid (Ptosis) Repair
 In some cases the upper eyelid asymmetry may be due to excessive skin in which an upper blepharoplasty will be corrective. Or the upper eyelid may be hanging lower than the other side relative to its position on the iris of the eye in which an upper eyelid ptosis repair would be needed. But when the eye is being raised in vertical orbital dystopia repair by orbital floor augmentation, it will become more ‘buried’ under the existing position of the upper eyelid in which a ptosis repair will definitely be needed.
In some cases the upper eyelid asymmetry may be due to excessive skin in which an upper blepharoplasty will be corrective. Or the upper eyelid may be hanging lower than the other side relative to its position on the iris of the eye in which an upper eyelid ptosis repair would be needed. But when the eye is being raised in vertical orbital dystopia repair by orbital floor augmentation, it will become more ‘buried’ under the existing position of the upper eyelid in which a ptosis repair will definitely be needed.
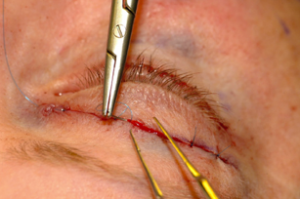
Outer Eye Corner Elevation (Lateral Canthoplasty)
 When the outer corner of the eye is downturned or lower than the opposite side, its position can be lifted by changing the position of the lateral cantonal tendon known as a lateral canthoplasty.
When the outer corner of the eye is downturned or lower than the opposite side, its position can be lifted by changing the position of the lateral cantonal tendon known as a lateral canthoplasty.
![]() But when the entire lower eyelid as it crosses the lower lid needs to elevated (vertical orbital dystopia repair) a lateral canthoplasty will have to be supported by a spacer graft of the lower eyelid. Vertical lengthening/elevation of the lower eyelid needs more tissue to be successfully maintained.
But when the entire lower eyelid as it crosses the lower lid needs to elevated (vertical orbital dystopia repair) a lateral canthoplasty will have to be supported by a spacer graft of the lower eyelid. Vertical lengthening/elevation of the lower eyelid needs more tissue to be successfully maintained.
Orbital Floor Augmentation
 The lower asymmetric eyeball can be safely raised to some degree (up to 5mms) by building up the floor of the eye in vertical orbital dystopia. This can be done by a variety of methods from bone grafts to synthetic materials. Because the cheekbone is often affected as well and there is a need to match the orbital floors as closely as possible, a custom designed orbital floor-rim-cheek implant offers the best chance to do so. Placed through a lower eyelid incision the connected inferior orbital bone and cheek can be treated with a single implant.
The lower asymmetric eyeball can be safely raised to some degree (up to 5mms) by building up the floor of the eye in vertical orbital dystopia. This can be done by a variety of methods from bone grafts to synthetic materials. Because the cheekbone is often affected as well and there is a need to match the orbital floors as closely as possible, a custom designed orbital floor-rim-cheek implant offers the best chance to do so. Placed through a lower eyelid incision the connected inferior orbital bone and cheek can be treated with a single implant.
Cheek Augmentation
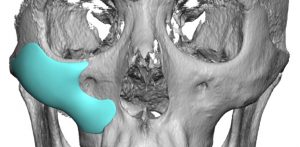 Most cheek asymmetries are best treated by a custom implant design. These cheek asymmetries often consist of only a few millimeters and cover a broader surface than one would think. They may extend up along the orbital rim, down unto the maxilla or out onto the zygomatic arch. Trying to place some form of a standard cheek implant or eyeballing a handmade implant usually just makes the cheek asymmetry different but not better.
Most cheek asymmetries are best treated by a custom implant design. These cheek asymmetries often consist of only a few millimeters and cover a broader surface than one would think. They may extend up along the orbital rim, down unto the maxilla or out onto the zygomatic arch. Trying to place some form of a standard cheek implant or eyeballing a handmade implant usually just makes the cheek asymmetry different but not better.
Cheekbone Reduction
 In cheekbones that are asymmetric by having excessive width, cheekbone reduction osteotomies can be performed. Depending upon the degree and extent back along the zygomatic arch of the excessive width, either an isolated intraoral zygomatic body osteotomy can be done or it may need to be combined with a posterior zygomatic arch osteotomy as well.
In cheekbones that are asymmetric by having excessive width, cheekbone reduction osteotomies can be performed. Depending upon the degree and extent back along the zygomatic arch of the excessive width, either an isolated intraoral zygomatic body osteotomy can be done or it may need to be combined with a posterior zygomatic arch osteotomy as well.
Cheeklift
 A sagging asymmetric cheek pad can be lifted using a variety of techniques. The direct cheeklift is done through the lower eyelid, pulls the cheek pad up vertically and secures it to a bone hole at the orbital rim. This is convenient if other work is already being done through the lower eyelid. Otherwise a temporal-based cheeklift can be done.
A sagging asymmetric cheek pad can be lifted using a variety of techniques. The direct cheeklift is done through the lower eyelid, pulls the cheek pad up vertically and secures it to a bone hole at the orbital rim. This is convenient if other work is already being done through the lower eyelid. Otherwise a temporal-based cheeklift can be done.
Rhinoplasty
 Straightening a deviated nose usually requires a septorhinoplasty to ensure the central support of the nose gets properly aligned. Nasal osteotomies and tip grafting/alignment are also needed. The nostril on the affected side may be higher to wider which can be aligned by a nostril repositioning procedure.
Straightening a deviated nose usually requires a septorhinoplasty to ensure the central support of the nose gets properly aligned. Nasal osteotomies and tip grafting/alignment are also needed. The nostril on the affected side may be higher to wider which can be aligned by a nostril repositioning procedure.
Corner of Mouth Lift
 Downturned corners of the mouth can be lifted and leveled by a pennant skin excision technique with orbicularis wedge muscle excision. In lip asymmetries where the lower position extends beyond just the mouth corner, the length of the pennant can be carried further up along the vermilion-skin edge for a more complete upper lip lifting effect.
Downturned corners of the mouth can be lifted and leveled by a pennant skin excision technique with orbicularis wedge muscle excision. In lip asymmetries where the lower position extends beyond just the mouth corner, the length of the pennant can be carried further up along the vermilion-skin edge for a more complete upper lip lifting effect.
Chin Bone Lengthening/Straightening
 For correction of chin asymmetries associated with a vertical deficiency, an intraorral osteotomy where the shorter side is lengthened and plated is one option. This works by creating a vertical bony opening on the short side which is grafted with tissue bank bone.
For correction of chin asymmetries associated with a vertical deficiency, an intraorral osteotomy where the shorter side is lengthened and plated is one option. This works by creating a vertical bony opening on the short side which is grafted with tissue bank bone.
Chin/Jawline Asymmetry
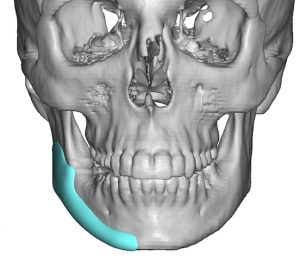 Most chin asymmetries involves the jawline and go all the way back to the jaw angles. (hemi-mandibular hypoplasia) This is best treated by a custom jawline implant that his designed to match the opposite side by computer design.
Most chin asymmetries involves the jawline and go all the way back to the jaw angles. (hemi-mandibular hypoplasia) This is best treated by a custom jawline implant that his designed to match the opposite side by computer design.
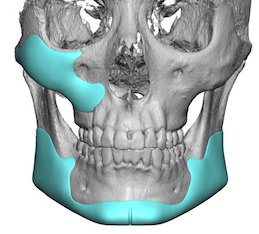 In some jawline asymmetries it may be best treat the entire jawline by a custom implant design if the patient desires overall jawline augmentation. As is often seen in lower jaw asymmetries the cheek that lies above it is also affected. Thus a combination of a custom cheek and jawline implant provides a good combination facial asymmetry treatment.
In some jawline asymmetries it may be best treat the entire jawline by a custom implant design if the patient desires overall jawline augmentation. As is often seen in lower jaw asymmetries the cheek that lies above it is also affected. Thus a combination of a custom cheek and jawline implant provides a good combination facial asymmetry treatment.
Jowl Tuckup
 In sagging lower cheek and jowl full, a limited lower facelift procedure known as a jowl tuckup can be effective soft tissue asymmetry management. Done through retrotragal ear incisions, most of which are behind the tragus and behind the ear a SMAS plication flap can be done to redrape the low hanging facial tissues.
In sagging lower cheek and jowl full, a limited lower facelift procedure known as a jowl tuckup can be effective soft tissue asymmetry management. Done through retrotragal ear incisions, most of which are behind the tragus and behind the ear a SMAS plication flap can be done to redrape the low hanging facial tissues.
Before Facial Asymmetry Surgery
A thorough assessment of the entire face from the skull down through the jawline using photographs and computer imaging is an essential diagnosis and treatment planning step. In most cases, a 3D CT scan is. critical in supplementing the physical examinationandr photographic analysis. These assessments are necessary to determine what exact procedure(s) would be beneficial and which ones would have the greatest impact on improving facial symmetry. A list of all structures contributing to the asymmetry is made and ordered in priority of importance to the patient. Then the appropriate procedures are matched to the diagnosis list. The patient then gets to choose which procedures they value and feel will make the greatest amount of improvement. In some cases, all selected procedures may be done at once and in other cases the patient may choose to do only a few or do a staged approach awaiting the outcome of the most important procedures first.
Facial Asymmetry – The Operation
All facial asymmetry surgery procedures are performed under general anesthesia, and certain patients will require an overnight stay in the facility, depending on the number of facial procedures performed and whether they are traveling alone or with someone. Each facial asymmetry surgery procedure involves different techniques; many include the use of bone or implants while others are performed using more traditional aesthetic surgery techniques such as soft tissue suspension or fat removal.
After Facial Asymmetry Surgery
While facial asymmetry surgery may involve a single procedure, more commonly it includes multiple facial procedures. As a result, the aftereffects such as facial swelling and bruising vary significantly from patient to patient. The length of recovery is not based on pain but rather on swelling and the time it takes to look more normal again. It could take anywhere from two to three weeks for one to feel completely comfortable being in public without having noticeable signs of surgery. Risks and complications from any facial asymmetry surgery procedure are individual; most of these are listed in this website under the individual procedure listings. The most important thing to understand is that facial asymmetry surgery is about lessening the degree of asymmetry; perfect facial symmetry is usually not possible. In many patients, it may take more than one surgery to attain the best possible result.
To view results from Dr. Eppley’s previous patients, visit our asymmetrical face surgery before and after photo gallery.
How Much Does Facial Asymmetry Surgery Cost?
Facial asymmetry surgery cost needs to be determined individually during a one-on-one consultation with your plastic surgeon. Facial asymmetry is unique to each patient so the number and complexity of the procedures required will differ greatly in each case. Additional cost considerations include the experience of the cosmetic surgeon and any hospital or facility fees required.
Learn More:
To learn more about facial asymmetry surgery and the procedures performed by Dr. Eppley or to schedule a consultation, please contact our office to schedule a virtual consultation.



A detailed description and pictures of your concerns allow for the most informed response.
Disclaimer: By submitting a question, you agree that it may be used for educational purposes. Any identifying details or photos will be removed. Responses are general and not a substitute for medical advice.
North Meridian Medical Building
Address:
12188-A North Meridian St.
Suite 310
Carmel, IN 46032
Contact Us:
Phone: (317) 706-4444
WhatsApp: (317) 941-8237