Cheek Reshaping
Cheek Reshaping Surgery
As one of the leading cheek reshaping specialists in America, Dr. Barry L. Eppley, has years of experience helping his patients achieve a more defined facial profile. Please read on to learn more about the procedure. To see results from our previous patients, visit our cheek before and after photo gallery .
 Well defined and distinct cheeks are part of an aesthetic and well balanced face. They help highlight the middle part of the face, promote a more youthful appearance, and can contribute to making the nose and chin smaller in certain patients. Women know this facial characteristic well by the common method of applying darker make-up underneath the cheekbone area and lighter make-up above it in an effort to highlight its location and shape. Cheeks appear in a variety of undesired aesthetic shapes from being too flat/lacking structure, being too prominent or wide, having fallen over time due to aging or prior surgery and having different cheek shapes between the two sides. (asymmetry)
Well defined and distinct cheeks are part of an aesthetic and well balanced face. They help highlight the middle part of the face, promote a more youthful appearance, and can contribute to making the nose and chin smaller in certain patients. Women know this facial characteristic well by the common method of applying darker make-up underneath the cheekbone area and lighter make-up above it in an effort to highlight its location and shape. Cheeks appear in a variety of undesired aesthetic shapes from being too flat/lacking structure, being too prominent or wide, having fallen over time due to aging or prior surgery and having different cheek shapes between the two sides. (asymmetry)

 When considering cheek reshaping surgery, particularly that of cheek augmentation, it is extremely important to appreciate the differences between the female and male cheekbone structures and what makes them look aesthetically better. Such cheekbone differences are well depicted in the art world with males having a higher and extended cheek prominences while women will have a lower and more anterior cheek fullness with a more angulated sweep backwards. This is a general statement about gender differences and in contemporary times these historic distinctions are becoming more blurred.
When considering cheek reshaping surgery, particularly that of cheek augmentation, it is extremely important to appreciate the differences between the female and male cheekbone structures and what makes them look aesthetically better. Such cheekbone differences are well depicted in the art world with males having a higher and extended cheek prominences while women will have a lower and more anterior cheek fullness with a more angulated sweep backwards. This is a general statement about gender differences and in contemporary times these historic distinctions are becoming more blurred.
CHEEKBONE AUGMENTATION
Injectable Cheek Enhancement
By far the most common form of cheek augmentation done is through the use of injectable synthetic fillers and fat. These minimally invasive methods offer immediate results without any downtime of significance and exacting placement of the augmentation materials. Synthetic fillers offer good results and are completely reversible when using hyaluron-based fillers. Fat injections can also be effective but their results are not always predictable (how much will survive) and are difficult to reverse. For many people synthetic fillers are a good starting point into cheek augmentation as a trial to determine whether they like it and where is the best augmentation location. Fat injections are often done as a matter of surgical convenience when performed along with other surgical procedures and if one is doing fat injections elsewhere on the face or body. The cheeks usually have one of the highest take rates in the face with the exception of thinner faces in younger people.
Cheek Implants
The cheek area can have permanent volume addedby the placement of an implant that sits either entirely on its bone surface and/or partially extends beneath it. While the concept of placing a cheek implant can seem simple, it is much more challenging than most think because of the 3D shape of the cheek and how it is positioned on the face to get a satisfying aesthetic result. This is illustrated by the wide range of contemporary cheek implant styles which selectively highlight specific portions or all of the cheek area.
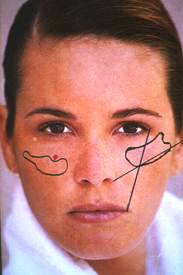 To help select the cheek implant that best creates the patient’s desired look, it is important to know which of the zones of cheek enhancement (malar, submalar, and zygomatic tail) needs to be covered. Such standard cheek implant options include the following:
To help select the cheek implant that best creates the patient’s desired look, it is important to know which of the zones of cheek enhancement (malar, submalar, and zygomatic tail) needs to be covered. Such standard cheek implant options include the following:
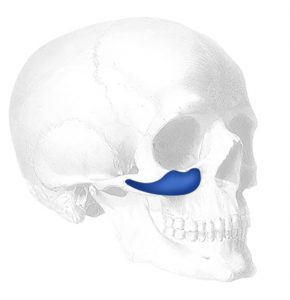
Malar Cheek Implants
 This cheek implant style provides complete coverage of the front and sides of the main body of the cheekbone. (zygomatic proper) It is designed to sit completely on the bone and provides anterolateral cheek fullness. It is most commonly used cheek implant style in patients seeking enhancement of their flatter cheeks.
This cheek implant style provides complete coverage of the front and sides of the main body of the cheekbone. (zygomatic proper) It is designed to sit completely on the bone and provides anterolateral cheek fullness. It is most commonly used cheek implant style in patients seeking enhancement of their flatter cheeks.
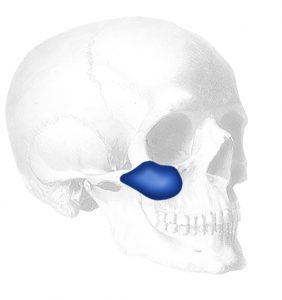
Submalar Cheek Implants
 This unique cheek implant sits mainly on the underside of the cheekbone and was originally designed to correct submalar hollowness from aging or in facial lipoatrophy. As a result it is the implant alternative to a soft tissue midface lift and creates a very similar and often more effective midface lift result. It is also used in conjunction with facelift surgery as the alternative to a deep plane technique in the cheek area.
This unique cheek implant sits mainly on the underside of the cheekbone and was originally designed to correct submalar hollowness from aging or in facial lipoatrophy. As a result it is the implant alternative to a soft tissue midface lift and creates a very similar and often more effective midface lift result. It is also used in conjunction with facelift surgery as the alternative to a deep plane technique in the cheek area.
Malar-Submalar Shell Cheek Implants
 As the name implies this cheek implant style combines the features of the malar and submalar areas in a single. This allows the implant to both address both cheekbone deficiencies as well as soft tissue sagging.
As the name implies this cheek implant style combines the features of the malar and submalar areas in a single. This allows the implant to both address both cheekbone deficiencies as well as soft tissue sagging.
Midface Cheek Implant

 This cheek implant style has similar properties as the malar-submalar shell but has a grid-like undersurface (Conform) which allows a fuller but softer look due to the adaptability of the implant to the bone.
This cheek implant style has similar properties as the malar-submalar shell but has a grid-like undersurface (Conform) which allows a fuller but softer look due to the adaptability of the implant to the bone.
Regardless of the cheek implant style, these implants are usually placed from an incision inside the mouth up under the upper lip. Cheek implants can also be placed through a lower eyelid incision which may be part of an overall midface lifting strategy. (with the exception of the submalar implant. While cheek implant surgery is fairly straightforward, there is a certain risk of asymmetry for two reasons. First, it is hard to see if they are positioned evenly because one can not see the placement of both implants at the same time. The use of bone landmarks is the only intraoperative guide for their placement. This is not always completely accurate however. Secondly, if the implants are not firmly secured onto their placed position on the bone they may shift after surgery. Their position is best assured by using self-tapping microscrews through the cheek implants to the underlying bone when possible or an external bolster for a few days after surgery.
Custom Cheek Implants
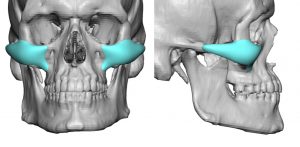
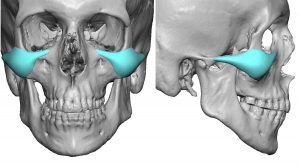 While the different styles and sizes of standard cheek implants can fulfill many cheek augmentation needs, the use of preformed implants can not satisfy every patient’s aesthetic needs. Custom cheek implants, designed from the 3D CT scan of the patient, has a useful role to play in several specify needs such as a specific aesthetic effect (e.g., high cheekbone bone look or extended cheek-arch styles), when cheekbone asymmetries exist (e.g., facial asymmetry) and for revision of previously unsatisfactory cheek augmentation results using preformed implants.
While the different styles and sizes of standard cheek implants can fulfill many cheek augmentation needs, the use of preformed implants can not satisfy every patient’s aesthetic needs. Custom cheek implants, designed from the 3D CT scan of the patient, has a useful role to play in several specify needs such as a specific aesthetic effect (e.g., high cheekbone bone look or extended cheek-arch styles), when cheekbone asymmetries exist (e.g., facial asymmetry) and for revision of previously unsatisfactory cheek augmentation results using preformed implants.
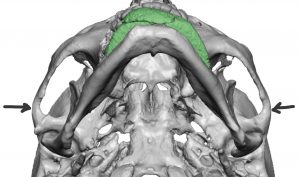
Zygomatic Sandwich Osteotomy (ZSO)
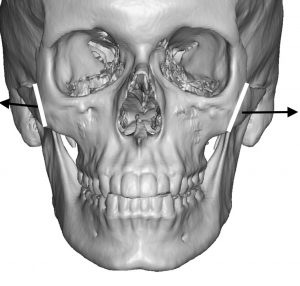
 One very unique form of non-implant or autologous cheek augmentation is by moving the main body of the cheekbone outward. By making a vertical bone cut through the zygomatic body from an intraoral approach, the bone is pushed outward using the zygomatic arch as a hinge. It is held in this outward position by a small plate and screws. This leaves a bone gap between the two cut bones ends into which a tissue bank graft is placed. Hence the name of the procedure, the zygomatic sandwich osteotomy. While appealing to some patients because it does not involve an implant, it only creates a dimensionally limited cheek augmentation effect that only widens the cheekbones. (can not add forward projection) But in the properly selected patient this can be a good cheek augmentation procedure.
One very unique form of non-implant or autologous cheek augmentation is by moving the main body of the cheekbone outward. By making a vertical bone cut through the zygomatic body from an intraoral approach, the bone is pushed outward using the zygomatic arch as a hinge. It is held in this outward position by a small plate and screws. This leaves a bone gap between the two cut bones ends into which a tissue bank graft is placed. Hence the name of the procedure, the zygomatic sandwich osteotomy. While appealing to some patients because it does not involve an implant, it only creates a dimensionally limited cheek augmentation effect that only widens the cheekbones. (can not add forward projection) But in the properly selected patient this can be a good cheek augmentation procedure.
CHEEK (Midface) Lifts
Midface/Cheek Sagging Due to Aging
Aging affects all regions of the face from the forehead down to the neck. While facelifts improve the neck and jawline and browlifts improve the forehead, the central third of the face has fewer surgical options for aging improvement besides eyelid surgery. It is often neglected or overlooked in facial rejuvenation approaches. The cheek tissue is well known to descend downward with time and gravity, creating a roll of tissue below the cheek bones (malar descent) and making a significant contribution to the deepening of the nasolabial folds.
Weak Cheekbones Contribute to Facial Aging
Some patients are highly susceptible to developing sagging cheeks because they have a weak or underdeveloped bone structure. Their cheekbones are flatter and more recessed and do not provide much of a ‘ledge’ for which the cheek tissues can be supported. Thus, when the ligaments holding the skin and soft tissues to the bone weakens they are especially prone to drifting ‘south
Cheeklift Types
The concept of a cheeklift is to reposition the fallen soft tissues back up onto the cheek bone. This can be done one of two ways, soft tissue resuspension or bone implant augmentation. In some cases, both cheeklift approaches may be used.
Cheeklift (Soft Tissue Suspension)
A soft tissue cheeklift is done through a lower eyelid (blepharoplasty) incision where the fallen cheek tissues are lifted back up onto the bone. At the same time, a lower blepharoplasty is also performed which most facial aging patients need as well. A soft tissue resuspension midface lift may also be done through a temporal incision (temporal suspenion), a scalp incision (cranial suspension) or combined with the Endotine device to help hold up the cheek tissues. Almost every approach, however, uses a lower eyelid incision as part of the procedure.
Cheeklift (Implant Augmentation)
 A bony cheeklift is done by placing a specially designed cheek implant (submalar or combined submalar/malar shell) onto the bone through an incision inside the mouth. By adding bone support, the fallen cheek tissues are lifted up. The size of the submalar or shell implant will determine how effective this type of cheeklift is. For some patients this is all the midface lifting effect they may need. Such implants can also be placed. through a lower eyelid incision if a lower blepharoplasty or combined direct cheek lift is done concurrently.
A bony cheeklift is done by placing a specially designed cheek implant (submalar or combined submalar/malar shell) onto the bone through an incision inside the mouth. By adding bone support, the fallen cheek tissues are lifted up. The size of the submalar or shell implant will determine how effective this type of cheeklift is. For some patients this is all the midface lifting effect they may need. Such implants can also be placed. through a lower eyelid incision if a lower blepharoplasty or combined direct cheek lift is done concurrently.
Cheeklift Operation
All cheek lifts are done under general anesthesia. A soft tissue re-suspension is done through a lower eyelid incision, often combined with an intraoral incision as well. This allows the cheek tissues to be completely freed up and lifted. The key to this type of cheeklift is in how to lift and maintain support to the bone as it heals. (where and how to the tissues) While many different methods have been described, my preferred approach is a cranial suspension technique where the sutures lifting the cheek tissues are passed under the temporal and forehead skin and sewn high up onto the skull bone directly above the outer corner of the eye. Malar shell or submalar cheek implants are introduced from inside the mouth and placed on top of the cheek bone. The implants are secured into position by a small titanium screw to the bone to prevent the risk of displacement.
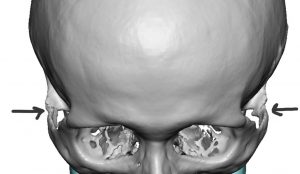
CHEEKBONE REDUCTION/NARROWING
Due to a broad or wide face, some people desire a facial narrowing surgery. The widest part of most people’s faces is in the cheek areawith the greatest convexity at the midportion of the zygomatic arch. This thin sliver of bone is a bowed structure that connects the larger cheek or zygomatic bone with the temporal bone above the ear. Underneath the zygomatic arch passes the large temporalis muscle which attaches to the upper portion of the lower jaw.

 The cheekbones can be reduced by moving the zygoma and the zygomatic arch inward, as a combined unit, through osteotomies or bone cuts. From inside the mouth an oblique straight line or L-shaped osteotomy is done through the main body of the zygoma and from a small temporal incision the attachment of the tail of the zygomatic arch is cut. This allows a cheekbone reduction to be done by moving these bone segments inward and fixing them in a more narrowed position with small plates and screws. These types of osteotomies are the primary method of cheekbone reduction surgery and produce the greatest amount of facial narrowing.
The cheekbones can be reduced by moving the zygoma and the zygomatic arch inward, as a combined unit, through osteotomies or bone cuts. From inside the mouth an oblique straight line or L-shaped osteotomy is done through the main body of the zygoma and from a small temporal incision the attachment of the tail of the zygomatic arch is cut. This allows a cheekbone reduction to be done by moving these bone segments inward and fixing them in a more narrowed position with small plates and screws. These types of osteotomies are the primary method of cheekbone reduction surgery and produce the greatest amount of facial narrowing.

 Cheekbone reduction osteotomies narrow the side of the face by moving the entire zygomatic arch inward. This operation is about changing the projection (peak of the convexity) of the zygomatic arch by moving its two ‘ends’ inward. How effective this would be for any patient with a wider face or large ‘cheekbones’ requires a preoperative x-ray to look at the natural convexity of their arches to determine how much contribution of the width comes from the zygomatic arches.
Cheekbone reduction osteotomies narrow the side of the face by moving the entire zygomatic arch inward. This operation is about changing the projection (peak of the convexity) of the zygomatic arch by moving its two ‘ends’ inward. How effective this would be for any patient with a wider face or large ‘cheekbones’ requires a preoperative x-ray to look at the natural convexity of their arches to determine how much contribution of the width comes from the zygomatic arches.
 A limited cheekbone reduction technique, using only the posterior zygomatic arch osteotomy, can be done in select cases. Some patients have an excessive cheek width that is located more posteriorly towards the ear or they have had a cheekbone reduction surgery that did not treat the posterior part of the cheek. The posterior zygomatic arch osteotomy done through a sideburn incision can be done to narrow this often overlooked wide cheek area.
A limited cheekbone reduction technique, using only the posterior zygomatic arch osteotomy, can be done in select cases. Some patients have an excessive cheek width that is located more posteriorly towards the ear or they have had a cheekbone reduction surgery that did not treat the posterior part of the cheek. The posterior zygomatic arch osteotomy done through a sideburn incision can be done to narrow this often overlooked wide cheek area.

 In far less common indications cases, burring or shaving of the main body of the cheekbone can be done from an intraoral approach. Because of the limited area of treatment only subtle am0unts of a cheekbone reduction effect is usually obtained. Understanding the location of where the cheekbone can be reduced will determine if this suits a patient’s needs.
In far less common indications cases, burring or shaving of the main body of the cheekbone can be done from an intraoral approach. Because of the limited area of treatment only subtle am0unts of a cheekbone reduction effect is usually obtained. Understanding the location of where the cheekbone can be reduced will determine if this suits a patient’s needs.
CHEEK SLIMMING (BUCCAL LIPECTOMY)
 Midfacial defatting can be a useful facial reshaping technique for those with chubby or naturally rounder faces. The most well known facial slimming technique is that of the buccal lipectomy. While this procedure is well known it is frequently misunderstood both anatomically as well as what part of the cheek it actually affects.
Midfacial defatting can be a useful facial reshaping technique for those with chubby or naturally rounder faces. The most well known facial slimming technique is that of the buccal lipectomy. While this procedure is well known it is frequently misunderstood both anatomically as well as what part of the cheek it actually affects.
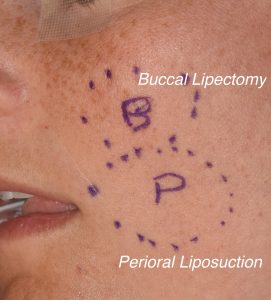 The buccal fat pad is a relatively large collection of concentrated fat that sits right below the cheekbone that is easily accessed from a small intraoral incision opposite the maxillary second molar. Its removal, either partially or totally, helps reduce upper cheek fullness. But it is important to know that its effects do not extend all the way down to the level of the mouth or the jawline. This is a common misconception that it does. For this reason perioral liposuction is a good complement to buccal lipectomies. This reduction in the thickness of the subcutaneous fat layer by the side of the mouth and down to the jawline creates a more complete cheek slimming effect. Done with a very small cannula from an incision just inside the corner of the mouth, this lower cheek area can be treated from the buccal fat area down to the jawline. This is a perfectly safe area to treat by liposuction due to the lack of any motor nerves that run in this area.
The buccal fat pad is a relatively large collection of concentrated fat that sits right below the cheekbone that is easily accessed from a small intraoral incision opposite the maxillary second molar. Its removal, either partially or totally, helps reduce upper cheek fullness. But it is important to know that its effects do not extend all the way down to the level of the mouth or the jawline. This is a common misconception that it does. For this reason perioral liposuction is a good complement to buccal lipectomies. This reduction in the thickness of the subcutaneous fat layer by the side of the mouth and down to the jawline creates a more complete cheek slimming effect. Done with a very small cannula from an incision just inside the corner of the mouth, this lower cheek area can be treated from the buccal fat area down to the jawline. This is a perfectly safe area to treat by liposuction due to the lack of any motor nerves that run in this area.
The dual effects of buccal lipectomies and perioral liposuction can create a noticeable slimming effect even in patients that don’t really have a round or fuller facial shape. In the right face these defatting procedures can make the cheekbones look more prominent. In combination with even smaller cheek implants, a substantially enhanced cheekbone definition can be achieved.
Cheek Dimpleplasty
Cheek dimples exist naturally because of a tissue defect or split through the zyygomaticus major muscle in most people. They may only be present when smiling or exist in a lesser form at rest and get deeper with smiling. Cheek dimples can be surgically created and are most reliably done to appear when smiling with little presence at rest.
 Cheek dimpleplasty is done under local anesthesia with an intraoral technique. A small amount of mucosal lining and muscle directly opposite the desired dimple location is removed. A percutaneous suture is used to pull the skin inward towards the cheek mucosa which then heals with an outward indentation.
Cheek dimpleplasty is done under local anesthesia with an intraoral technique. A small amount of mucosal lining and muscle directly opposite the desired dimple location is removed. A percutaneous suture is used to pull the skin inward towards the cheek mucosa which then heals with an outward indentation.
Dr. Eppley not only performs cheek augmentation to help his facial aesthetic patients. He also performs facelift, Botox, in addition to helping rhinoplasty patients achieve their desired facial profile. He also offers custom implants patients facial implant procedures that are specifically tailored to their aesthetic or reconstructive needs
Cheek Reshaping – Before Surgery
Evaluation of the face and how cheek augmentation and/or lifting may fit in the overall shape of the face is important for the patient to visually see. Often times, cheek augmentation is part of other facial procedures (e.g., nasal or eyelid surgery) to improve facial proportions and overall facial balance. This may be helped by computer predictions, although this is one of the harder areas to demonstrate by digital imaging. Choosing from amongst the different cheek implant styles is important as different areas of the cheek may be highlighted in different patients. Cheek or midface lifting is often part of other anti-aging facial plastic surgery such as a facelift or browlift and eyelid surgery.
Cheek Reshaping – Operation
Cheek implants are done as an outpatient procedure under general anesthesia in most cases. They are most commonly placed through the mouth through a small incision high above the molar (upper back) teeth. They may be secured to the bone by a small screw to prevent them from moving after surgery. In some cases, they may be placed through a lower eyelid incision if a lower eyelid procedure is also being performed at the same time. Cheek (midface) lifting is done through a lower eyelid incision and is often part of eyelid and browlifting surgery. The cheek tissues are elevated and sutured back up onto the bone, restoring fullness to the cheek area and eliminating bags below the cheekbone.
Cheekbone Reshaping Recovery
No specific dressing or bandages are needed. Mild swelling of the cheek and middle part of the face will be seen but usually there is no bruising. Pain is very minimal. The final result is usually seen in about three weeks when most of the swelling has subsided.
Complications are very infrequent with facial implants due to the good tolerance of the face to synthetic materials, particularly at the bone level. Infection is very rare. Implant location and size (too much or too little) is the most common complication that may require revisional surgery. The only significant complication from cheek lifting is alteration of the lower eyelid position (pulled down) due to scar contracture. While rare, it may require a touch-up procedure to readjust the lower eyelid.



A detailed description and pictures of your concerns allow for the most informed response.
Disclaimer: By submitting a question, you agree that it may be used for educational purposes. Any identifying details or photos will be removed. Responses are general and not a substitute for medical advice.
North Meridian Medical Building
Address:
12188-A North Meridian St.
Suite 310
Carmel, IN 46032
Contact Us:
Phone: (317) 706-4444
WhatsApp: (317) 941-8237