Lip Surgery
Lip Surgery
Lip enhancement patients have visited Dr. Barry Eppley for many years for help in achieving fuller and more beautiful lips. Please visit the lip injection before and after results page to view before and after pictures.
LIP AESTHETICS
 In the past decade, full pouty lips have become the epitome of feminine beauty. In most Caucasians, the size of the upper lip is about two-thirds that of the lower lip. The trend today is to have the upper lip match the lower lip in size. Certain people are born with small thin lips, aging effects can make the lips lose volume and lengthen, and facial expression and smoking contribute to the development of vertical lines around the lips. All of these influences have seen the number of cosmetic lip procedures performed increase dramatically.
In the past decade, full pouty lips have become the epitome of feminine beauty. In most Caucasians, the size of the upper lip is about two-thirds that of the lower lip. The trend today is to have the upper lip match the lower lip in size. Certain people are born with small thin lips, aging effects can make the lips lose volume and lengthen, and facial expression and smoking contribute to the development of vertical lines around the lips. All of these influences have seen the number of cosmetic lip procedures performed increase dramatically.
LIP AUGMENTATION – It’s All About The Vermilion
In simplicity, lip enhancement is about improving the amount of vermilion (pink part) show and its shape across the lip from one mouth corner to the other. This creates a fuller lip appearance. It is the vermilion that is responsible for our perception of lip size. Therefore, a variety of approaches exist for improving the amount of vermilion show throughout the lip. This includes injectable fillers, implants, and surgical lip advancements and lip lifts. Which procedure is right for a specific patient is a matter of how much vermilion show (how thin are your lips?) you have and the appeal of the advantages and disadvantages of each lip approach.
Injectable Fillers
 Injectable fillers are the most common method of lip enhancement. For the lips, the injectable filler should be composed of hyaluronic-acid, a naturally resorbing sugar-like molecule (e.g., Juvederm, Restylane), that has very few problems and always goes away. While losing the injected filler volume is not desired by patients, the lips are very sensitive and potentially reactive to particulated longer-lasting fillers and these should be avoided for lip augmentation. While injectable filler lip enhancement is quick to-do and produces an instant result with virtually no recovery, treatments must be repeated and the cost over time can be significant. As a result many patients will eventually develop ‘filler fatigue) and seek a more permanent solution to their aesthetic lip concerns.
Injectable fillers are the most common method of lip enhancement. For the lips, the injectable filler should be composed of hyaluronic-acid, a naturally resorbing sugar-like molecule (e.g., Juvederm, Restylane), that has very few problems and always goes away. While losing the injected filler volume is not desired by patients, the lips are very sensitive and potentially reactive to particulated longer-lasting fillers and these should be avoided for lip augmentation. While injectable filler lip enhancement is quick to-do and produces an instant result with virtually no recovery, treatments must be repeated and the cost over time can be significant. As a result many patients will eventually develop ‘filler fatigue) and seek a more permanent solution to their aesthetic lip concerns.
Injectable Fat Grafting
 The one potentially permanent method for permanent lip injections is the use of fat. Fat is a natural material that is taken from the patient by liposuction, processed into a concentrate and then injected into the lip(s) using a layered microaliquot technique. While fat is very appealing how well it will survive and its degree of permanency, unfortunately, is not assured. Persistent fat volume retention is usually low and best results come from multiple injection treatments.
The one potentially permanent method for permanent lip injections is the use of fat. Fat is a natural material that is taken from the patient by liposuction, processed into a concentrate and then injected into the lip(s) using a layered microaliquot technique. While fat is very appealing how well it will survive and its degree of permanency, unfortunately, is not assured. Persistent fat volume retention is usually low and best results come from multiple injection treatments.
Lip Implants

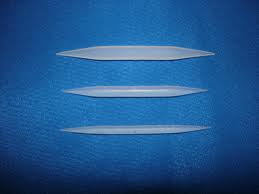 Lip implants are available that offer a permanent solution to increasing the size of the lip vermilion. (Permalip implants). This is an utrasoft solid silicone implant that has a smooth surface. It is available in 3mm, 4mm and 5mm sizes with different lengths. They are shaped as tapered cylinders that extend across the lip from one corner of the mouth to the other. While lip implants have a very checkered history, Permalip implants offers a well tolerated material that is both easy to insert as well as to remove. The lips are a sensitive area for any solid implant. But for those patients who like the results of injectable lip fillers but want a permanent ‘filler’, lip implants provide such an option.
Lip implants are available that offer a permanent solution to increasing the size of the lip vermilion. (Permalip implants). This is an utrasoft solid silicone implant that has a smooth surface. It is available in 3mm, 4mm and 5mm sizes with different lengths. They are shaped as tapered cylinders that extend across the lip from one corner of the mouth to the other. While lip implants have a very checkered history, Permalip implants offers a well tolerated material that is both easy to insert as well as to remove. The lips are a sensitive area for any solid implant. But for those patients who like the results of injectable lip fillers but want a permanent ‘filler’, lip implants provide such an option.
Surgical Lip Lifts and Vermilion (Lip)Advancements
Surgical options exist to change the size and shape of the lip vermilion, procedures known as lifts and advancements. These are excisional procedues that remove skin from either under the nose or along the lip skin lines to affect a change in the size and shape of the lip vermilion. They provide permanent lip enhancement results but do so with the aesthetic trade-off of fine line scars.
 A subnasal upper lip lift, also known as a bullhorn lip lift because of the shape of the skin excision, is done at the base of the nose and lifts the central lip area known as the cupid’s bow primarily. It does not enhance the vertical height of the vermilion across the whole upper lip contrary to the statements of some surgeons. Thus one should not expect the very sides of the lip or the mouth corners to be changed from any lifting done from around the base of the nose.
A subnasal upper lip lift, also known as a bullhorn lip lift because of the shape of the skin excision, is done at the base of the nose and lifts the central lip area known as the cupid’s bow primarily. It does not enhance the vertical height of the vermilion across the whole upper lip contrary to the statements of some surgeons. Thus one should not expect the very sides of the lip or the mouth corners to be changed from any lifting done from around the base of the nose.

 As a general rule the amount of skin removed in a subnasal lip lift should not exceed 33% of the total vertical philtral length. When keeping within this guideline good results that don’t look overdone can be achieved. It is important to remember that once skin is removed it can not be put back so it is an irreversible procedure.
As a general rule the amount of skin removed in a subnasal lip lift should not exceed 33% of the total vertical philtral length. When keeping within this guideline good results that don’t look overdone can be achieved. It is important to remember that once skin is removed it can not be put back so it is an irreversible procedure.
There are different incisional variations of the subnasal lip lift of which the most well known is the ‘Italian Lip Lift‘. This avoids the incision across the base of the columella and creates the lip lift by moving the lip skin up onto the columella of the nose. In the properly selected patient this can be an effective lip lift but it is not for most patients who seek a lip lift procedure.
 Conversely a lip advancement, known as a gull wing lift because of the shape of the skin excision, removes a strip of skin from one mouth corner to the other at the vermilion-cutaneous line. This directly changes the exposed lip vermilion. This is the single most powerful lip enhancement procedure that is permanent because of its direct effect on the position of the vermilion-skin edge. It also has the ability to change the shape of the Cupid’s bow, changing a flat non-descript shape into one with more obvious peaks or enhanced double convexity to the central upper lip. But it does so at the trade-off of a fine line scar along the more visible vermilion-cutaneous border. This fine line scar usually heals well but must always be taken into consideration.
Conversely a lip advancement, known as a gull wing lift because of the shape of the skin excision, removes a strip of skin from one mouth corner to the other at the vermilion-cutaneous line. This directly changes the exposed lip vermilion. This is the single most powerful lip enhancement procedure that is permanent because of its direct effect on the position of the vermilion-skin edge. It also has the ability to change the shape of the Cupid’s bow, changing a flat non-descript shape into one with more obvious peaks or enhanced double convexity to the central upper lip. But it does so at the trade-off of a fine line scar along the more visible vermilion-cutaneous border. This fine line scar usually heals well but must always be taken into consideration.

 Vermilion advancements can be performed on the upper lip, lower lip or both. Because of its powerful effect 3 or 4mm vermilion advancements can make a big difference particularly when performed on both upper and lower lips.
Vermilion advancements can be performed on the upper lip, lower lip or both. Because of its powerful effect 3 or 4mm vermilion advancements can make a big difference particularly when performed on both upper and lower lips.
Combination Subnasal Lip Lifts and Vermilion Advancements
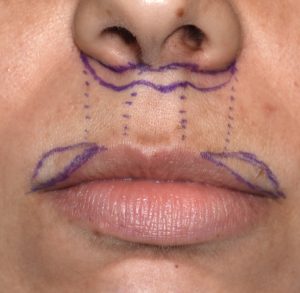 There is a role for combining surgical lip lifts and vermilion advancements. This is specifically for the patient who desires a subnasal lip lift but has thin sides or outer portions of the upper lip. Because a subnasal lip lift does not affect the entire lip from one mouth corner to the other, when performed in such a patient an unusual ‘rabbit-like’ lip appearance can result. This is better known as upper lip vermilion disproportion where the amount of vermilion show across the upper lip is out of balance. The central third of the upper lip has too much vermilion show compared to the sides. When such a patient is properly identified before surgery the combination of a subnasal lip lift and lateral vermilion advancements can be done for a more balanced amount of vermilion show across the whole upper lip. But the such a problem develops after a subnasal lip lift, the salvage position is to perform isolated lateral vermilion advancements.
There is a role for combining surgical lip lifts and vermilion advancements. This is specifically for the patient who desires a subnasal lip lift but has thin sides or outer portions of the upper lip. Because a subnasal lip lift does not affect the entire lip from one mouth corner to the other, when performed in such a patient an unusual ‘rabbit-like’ lip appearance can result. This is better known as upper lip vermilion disproportion where the amount of vermilion show across the upper lip is out of balance. The central third of the upper lip has too much vermilion show compared to the sides. When such a patient is properly identified before surgery the combination of a subnasal lip lift and lateral vermilion advancements can be done for a more balanced amount of vermilion show across the whole upper lip. But the such a problem develops after a subnasal lip lift, the salvage position is to perform isolated lateral vermilion advancements.
Male Lip Advancement and Lip Lifts
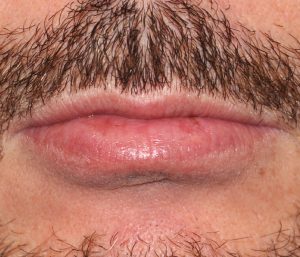
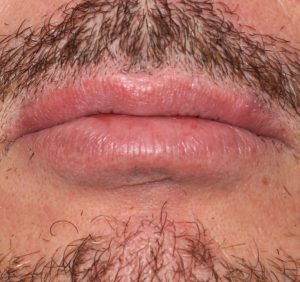 While many think that lip enhancement procedures are done exclusively for women, there are some men that have them as well. Men generally have less interest in procedures that require repeated treatments to maintain them (e.g., injectable fillers). Lip advancement and subnasal lip lifts can be done very successfully in men. While scars are always a concern with an permanent skin excisional lip procedure, the beard skin of men make most of these scars superior (even less visible) than what are seen in women.
While many think that lip enhancement procedures are done exclusively for women, there are some men that have them as well. Men generally have less interest in procedures that require repeated treatments to maintain them (e.g., injectable fillers). Lip advancement and subnasal lip lifts can be done very successfully in men. While scars are always a concern with an permanent skin excisional lip procedure, the beard skin of men make most of these scars superior (even less visible) than what are seen in women.
Cupid’s Bow Upper Lip Changes

 Most of the upper and lower lip is a line in an arc shape with the exception of the central region of the upper lip. This lip area has a double curve which resembles a bow laying on its side. The peaks of the bow are the location of the junction with the vertical philtral columns. Creating a more prominent cupid’s bow by injectable techniques is not usually successful and requires a more direct approach through a limited vermilion advancement technique. This can be combined with any other lip enhancement technique, surgical or non-surgical.
Most of the upper and lower lip is a line in an arc shape with the exception of the central region of the upper lip. This lip area has a double curve which resembles a bow laying on its side. The peaks of the bow are the location of the junction with the vertical philtral columns. Creating a more prominent cupid’s bow by injectable techniques is not usually successful and requires a more direct approach through a limited vermilion advancement technique. This can be combined with any other lip enhancement technique, surgical or non-surgical.

 Conversely some people prefer a smoother upper lip line without the double peaks of the cupid’s bow. This can be done by a very limited vermilion advancement between the two peaks.
Conversely some people prefer a smoother upper lip line without the double peaks of the cupid’s bow. This can be done by a very limited vermilion advancement between the two peaks.
Lip Asymmetries

 Lip asymmetries are often the result of a discrepancy in the location or level of the vermilion-skin border between the sides of the lip or the mouth corners. Almost always one side or lip area is lower or less full than the other side. This is particularly true in facial asymmetries where the mouth corner and lips on the affected side are less full or more inferiorly positioned. While injectable fillers can be useful treatments for some lip asymmetries, a permanent and often more effective improvement comes from changing the location of the asymmetric vermilion-skin junction location through limited vermilion advancement procedures.
Lip asymmetries are often the result of a discrepancy in the location or level of the vermilion-skin border between the sides of the lip or the mouth corners. Almost always one side or lip area is lower or less full than the other side. This is particularly true in facial asymmetries where the mouth corner and lips on the affected side are less full or more inferiorly positioned. While injectable fillers can be useful treatments for some lip asymmetries, a permanent and often more effective improvement comes from changing the location of the asymmetric vermilion-skin junction location through limited vermilion advancement procedures.
V-Y Mucosal Lip Augmentation
 Another uncommonly performed type of surgical lip augmentation that is both permanent and scarless is create vermilion show by rolling out the inner aspect of the lips. This internal roll technique is done by a technique known as a V-Y mucosal advancement. Internal v cuts are made in the wet mucosa inside the lip which permits the vermilion to roll out when the v cuts are closed into a y shape.
Another uncommonly performed type of surgical lip augmentation that is both permanent and scarless is create vermilion show by rolling out the inner aspect of the lips. This internal roll technique is done by a technique known as a V-Y mucosal advancement. Internal v cuts are made in the wet mucosa inside the lip which permits the vermilion to roll out when the v cuts are closed into a y shape.

 This is a technique that works best in lip that have adequate vermilion fullness, not very thin lips with little vermilion show. It is also a procedure that causes a fair amount of swelling after surgery unlike allayer surgical lip enhancement procedures.
This is a technique that works best in lip that have adequate vermilion fullness, not very thin lips with little vermilion show. It is also a procedure that causes a fair amount of swelling after surgery unlike allayer surgical lip enhancement procedures.
Corner of Mouth Lifts

 Downturning of the corner of the mouth typically occurs from aging but can also be a natural mouth feature in some people. Injectable methods of correcting the downturned mouth corners can be done by Botox injections to weaken the depressor angle muscle and injectable fillers to provide an upward push on the mouth corners. When these injectable procedures either are not ideally effective or one develops ‘injection fatigue’ surgical corner of mouth lifts can be considered.
Downturning of the corner of the mouth typically occurs from aging but can also be a natural mouth feature in some people. Injectable methods of correcting the downturned mouth corners can be done by Botox injections to weaken the depressor angle muscle and injectable fillers to provide an upward push on the mouth corners. When these injectable procedures either are not ideally effective or one develops ‘injection fatigue’ surgical corner of mouth lifts can be considered.
 Such corner mouth lifts have a long history and are typically described as the excision of a heart-shaped segment of skin and relocation of the mouth corner. While this procedure can be effective int leaves a line of scar in the skin outside the mouth corner which I have never liked. Thus my technique is the pennant corner of mouth lift which incorporates two unique features, keeping the scar line at the vermilion-skin junction and performing an orbicularis tightening/lift. In essence it creates a vermilion corner relocation higher up on the skin at the mouth corner.
Such corner mouth lifts have a long history and are typically described as the excision of a heart-shaped segment of skin and relocation of the mouth corner. While this procedure can be effective int leaves a line of scar in the skin outside the mouth corner which I have never liked. Thus my technique is the pennant corner of mouth lift which incorporates two unique features, keeping the scar line at the vermilion-skin junction and performing an orbicularis tightening/lift. In essence it creates a vermilion corner relocation higher up on the skin at the mouth corner.
Mouth Widening
 One determination of the size of the mouth is how wide it is, the linear measure from one mouth corner to the other. The ideal width of the mouth is defined by whether the mouth corners are as far out as a vertical line dropped down from the pupils. Regardless of what it is considered ideal, for the the person who feels their mouth is too small a mouth widening procedure is available. Mouth widening is a form of vermilion advancement, like a corner of mouth lift, but done in a horizontal direction. The excisional pattern is shaped like an arrow and involves removal of a wedge of orbicularis muscle to accommodate the corner widening. Like any vermilion advancement procedure there is always the tradeoff of a fine line scar around the mouth corner.
One determination of the size of the mouth is how wide it is, the linear measure from one mouth corner to the other. The ideal width of the mouth is defined by whether the mouth corners are as far out as a vertical line dropped down from the pupils. Regardless of what it is considered ideal, for the the person who feels their mouth is too small a mouth widening procedure is available. Mouth widening is a form of vermilion advancement, like a corner of mouth lift, but done in a horizontal direction. The excisional pattern is shaped like an arrow and involves removal of a wedge of orbicularis muscle to accommodate the corner widening. Like any vermilion advancement procedure there is always the tradeoff of a fine line scar around the mouth corner.
Lip Lines and Wrinkles

 The most challenging and pesky problem affected the lips is age-related vertical lip lines and wrinkles. Like all facial wrinkles the cause is the near continuous action of the orbicularis muscle which encircles the lips, creating wrinkles perpendicular to the movement of the muscle. While Botox injections can help reduce some of the muscle action and help with the wrinkle reduction, it will only soften some of the wrinkles. As a result other wrinkle reduction methods are needed of which a variety of skin resurfacing methods are available. The most common topical method used is laser resurfacing. If the lip lines are very deep, the historic use of dermabrasion can also be very effective. While laser resurfacing and dermanradsion are effective they are not permanent as the orbicularis muscle will continue to work. Maintenance treatments are needed to main long-term results.
The most challenging and pesky problem affected the lips is age-related vertical lip lines and wrinkles. Like all facial wrinkles the cause is the near continuous action of the orbicularis muscle which encircles the lips, creating wrinkles perpendicular to the movement of the muscle. While Botox injections can help reduce some of the muscle action and help with the wrinkle reduction, it will only soften some of the wrinkles. As a result other wrinkle reduction methods are needed of which a variety of skin resurfacing methods are available. The most common topical method used is laser resurfacing. If the lip lines are very deep, the historic use of dermabrasion can also be very effective. While laser resurfacing and dermanradsion are effective they are not permanent as the orbicularis muscle will continue to work. Maintenance treatments are needed to main long-term results.
LIP REDUCTION

 While some people feel their lips are too small, others may feel that their lips are too big. The amount of exposed vermilion is seen as excessive and the perception is that the size of the lips is an overwhelming feature on their face. Lip reduction surgery reduces the size of the lip by removing tissue from the internal part of the lip at the wet-dry junction. (where the vermilion (dry) meets the mucosa (wet) The key in lip reduction is that this removal must be from the dry vermilion and not the wet mucosa. This then rolls back the outer vermilion inward, reducing the size of the lips and putting the scar in a near invisible location. As a general rule lip reduction can produce a 1/4 to 1/3 reduction in lip size in a single surgery.
While some people feel their lips are too small, others may feel that their lips are too big. The amount of exposed vermilion is seen as excessive and the perception is that the size of the lips is an overwhelming feature on their face. Lip reduction surgery reduces the size of the lip by removing tissue from the internal part of the lip at the wet-dry junction. (where the vermilion (dry) meets the mucosa (wet) The key in lip reduction is that this removal must be from the dry vermilion and not the wet mucosa. This then rolls back the outer vermilion inward, reducing the size of the lips and putting the scar in a near invisible location. As a general rule lip reduction can produce a 1/4 to 1/3 reduction in lip size in a single surgery.
 One unique use of lip reduction surgery is in the treatment of chronically dry or chapped lips in which portions of the dry vermilion are refractory to topical treatments. These areas may be amenable to being treated by surgical removal of part or all of the affected dry vermilion depending upon the proximity of the dry areas to the wet-dry line. Usually not all of the chapped dry vermilion can be removed to prevent excessive lip reduction but some portions of it which helps reduce the magnitude of the problem.
One unique use of lip reduction surgery is in the treatment of chronically dry or chapped lips in which portions of the dry vermilion are refractory to topical treatments. These areas may be amenable to being treated by surgical removal of part or all of the affected dry vermilion depending upon the proximity of the dry areas to the wet-dry line. Usually not all of the chapped dry vermilion can be removed to prevent excessive lip reduction but some portions of it which helps reduce the magnitude of the problem.
CLEFT LIP REVISION

 A unique lip shape problem is that of the cleft lip. As a congenital facial defect that affects roughly 1 in every 1,000 births in the U.S., its disruption of the natural merging of the lip tissues creates many well known lip shape issues. While most cleft lip repairs are done in infancy, and this closes the wide gap between the two separated lip halves, it rarely produces a perfect realignment of the natural vermilion-cutaneous border or even adequate lip fullness. Thus many cleft patients need lip revisions later on in life in childhood or their teenage years. Adult cleft lip revision can often also be helpful as older patients often think that their lip can not be further improved… which often is not true.
A unique lip shape problem is that of the cleft lip. As a congenital facial defect that affects roughly 1 in every 1,000 births in the U.S., its disruption of the natural merging of the lip tissues creates many well known lip shape issues. While most cleft lip repairs are done in infancy, and this closes the wide gap between the two separated lip halves, it rarely produces a perfect realignment of the natural vermilion-cutaneous border or even adequate lip fullness. Thus many cleft patients need lip revisions later on in life in childhood or their teenage years. Adult cleft lip revision can often also be helpful as older patients often think that their lip can not be further improved… which often is not true.
Unlike aesthetic enhancement of a normal lip, the cleft lip requires a working knowledge of every form of lip reconstruction methods. A wide variety of lip reshaping techniques are needed including narrowing of philtral scars, creation of orbicularis muscle integrity, vermilion cutaneous realignment, enhanced lip fullness and internal vestibular lengthening/scar release.
Lip Enhancement – Before Surgery
Determining the correct procedure for the patient amongst the lip options available is the most important issue preoperatively. The patient must have a clear understanding of the advantage and disadvantages with each type of procedure. For such a small but prominent area of the face, the lips have a diverse number of non-surgical and surgical options from which to choose. The safest and most conservative approach is to try temporary injectable fillers first and only ‘graduate’ to more permanent options if dissatisfied.
Lip Enhancement – Operation
All of the lip procedures can be performed under either local or sedation anesthesia as an outpatient. Often they are combined with other aesthetic facial or body procedures and are done under general anesthesia. The procedures are relatively short to perform. For lip implants, the incisions are placed in the red portion either in the corner of the mouth or in the central aspect of the lip which aids in passing the implant into the correct position. For lip advancements, the skin is removed at the junction of the red and white portions of the lips with the final suture line at this junction. For lip lifts, the skin is removed at the base of the nose with the final suture line at the skin crease at the junction of the upper lip and nose. The corner of the lift is the smallest surgery of the lips, removing a triangle of skin overhanging the mouth corners. In peeling or laser resurfacing, the outer layer of skin surrounding the vermilion is removed, allowing smoother skin to result after healing. Skin resurfacing may be combined with other lip enhancement procedures at the same time.
Lip Enhancement – After Surgery
Only antibiotic ointment is used on the lip and suture lies with no other dressings needed. There is very minimal postoperative discomfort with any of the procedures. More swelling is associated with lip implants than those with skin excision or resurfacing. Bruising is rarely seen. By three weeks after surgery, however, most of the swelling is gone and the result evident. Lip sutures are removed after one week. Lipstick may be worn again after the first week. In resurfacing, the treated areas of the lip must be kept moist with antibiotic ointment. Once healed, it will take several months for the redness of the treated skin to fade.
Complications with lip implants (synthetic) are more frequent than with lip advancement/lifts due to the indwelling material. These include the potential for unnatural palpability, lip stiffness, and infection. When these occur, removal of the implant may be needed or the implant may need to be replaced. In fat injections, most of the fat eventually atrophies and retained lip volume may be unpredictable. For lip advancements/lifts, the only issue is the potential for adverse scarring which seems to be very uncommon. Slight asymmetries may need to have a touch-up procedure for optimal results. In laser resurfacing, pre- and postoperative anti-viral medication needs to be taken to prevent outbreak of herpetic lip infections, even if the patient has never had a prior eruption.



A detailed description and pictures of your concerns allow for the most informed response.
Disclaimer: By submitting a question, you agree that it may be used for educational purposes. Any identifying details or photos will be removed. Responses are general and not a substitute for medical advice.
North Meridian Medical Building
Address:
12188-A North Meridian St.
Suite 310
Carmel, IN 46032
Contact Us:
Phone: (317) 706-4444
WhatsApp: (317) 941-8237