Waist and Torso Narrowing/Rib Removal Surgery
Waist Narrowing/ Rib Removal

 Waist Narrowing – commonly called Rib Removal Surgery – is a body contouring procedure for reduction of internal anatomic restrictions for horizontal waistline narrowing. When non-surgical (diet, exercise and waist training) and surgical efforts (liposuction, tummy tucks) have not achieved as much waistline reduction as desired, one can consider rib removal surgery.
Waist Narrowing – commonly called Rib Removal Surgery – is a body contouring procedure for reduction of internal anatomic restrictions for horizontal waistline narrowing. When non-surgical (diet, exercise and waist training) and surgical efforts (liposuction, tummy tucks) have not achieved as much waistline reduction as desired, one can consider rib removal surgery.
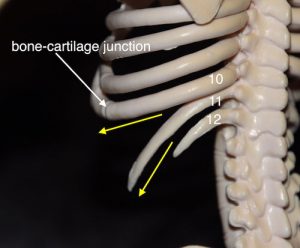
The concept of rib removal can be appreciated by pushing in on your own waistline in which ribs #11 and #12 can be felt. These free-floating ribs angle sharply downward, unlike all ribs above them, where their ends are attached to muscle and fascia. These ribs provide outward support to the shape of the waistline. As a result, reduction of the outer ends of these ribs can help the waistline to collapse inward and create a more inward shape and a smaller circumferential measurement.
 wasit narrowing rib removal surgery Dr Barry Eppley IndianapolisWhile the procedure is called Rib Removal, it involves more tissue reduction than the name alone implies. Flank liposuction and latissimus dorsi muscle reductions are also concurrently done to further improve the amount of waistline reduction achieved. In all patients, the outer sections of ribs #11 and #12 are removed. In certain patients, a section of rib #10, which wraps around the waistline to attach to the subcostal ribcage, is also removed. This is indicated for those patients who have a shorter torso and/or want to do maximum waistline reduction. The entire surgery is usually performed through twin 4.5cm incisions placed over rib #11 on the back.
wasit narrowing rib removal surgery Dr Barry Eppley IndianapolisWhile the procedure is called Rib Removal, it involves more tissue reduction than the name alone implies. Flank liposuction and latissimus dorsi muscle reductions are also concurrently done to further improve the amount of waistline reduction achieved. In all patients, the outer sections of ribs #11 and #12 are removed. In certain patients, a section of rib #10, which wraps around the waistline to attach to the subcostal ribcage, is also removed. This is indicated for those patients who have a shorter torso and/or want to do maximum waistline reduction. The entire surgery is usually performed through twin 4.5cm incisions placed over rib #11 on the back.
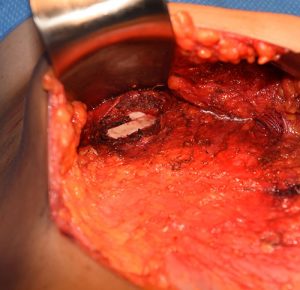
 One of the very important maneuvers in rib removal surgery is the preservation of the intercostal neurovascular bundle, specifically the intercostal nerve. You want to be able to remove the rib portion but keep the intercostal nerve, which runs along a groove on the underside of the rib, intact. By not injuring the nerve at each rib removal site the risk of chronic pain from nerve injury after surgery is eliminated.
One of the very important maneuvers in rib removal surgery is the preservation of the intercostal neurovascular bundle, specifically the intercostal nerve. You want to be able to remove the rib portion but keep the intercostal nerve, which runs along a groove on the underside of the rib, intact. By not injuring the nerve at each rib removal site the risk of chronic pain from nerve injury after surgery is eliminated.
 The amount of waistline reduction, as reported by patients, averages between one and three inches depending on individual body shape, weight, and thickness of tissues. There are some patients who get a more significant result than others as a result of these anatomic differences.
The amount of waistline reduction, as reported by patients, averages between one and three inches depending on individual body shape, weight, and thickness of tissues. There are some patients who get a more significant result than others as a result of these anatomic differences.

 Everyone sees a more inward movement or concavity to the outer waistline which is aesthetically more valuable than a circumferential waistline measurement for most patients. There are some patients who get more significant results than others
Everyone sees a more inward movement or concavity to the outer waistline which is aesthetically more valuable than a circumferential waistline measurement for most patients. There are some patients who get more significant results than others
Dr. Eppley’s clinical experience in aesthetic rib removal surgery for waist narrowing is that it is extremely safe and presents no long-term issues with partial loss of the outer portions of the lower ribs or the muscle that has been removed. In the properly selected patient, it offers an amount a waist narrowing effect that cannot otherwise be achieved by more commonly used procedures. (liposuction, tummy tuck) Rib removal surgery is often combined with other procedures such as buttock and hip augmentation, taking advantage of the prone patient position in surgery used for rib removal surgery.





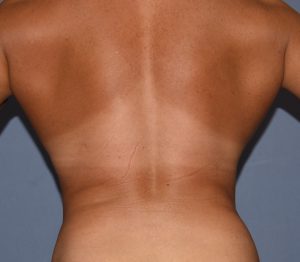
Perhaps surprising to some, a common female patient seeking waist reduction is already very thin. Their issue is that their body shape is very straight without any curves. They seek some more inward waist shape for a more feminine body appearance as opposed to the more ‘boyish’ shape they currently have. Such patients often have some of the most successful results because they are so thin.



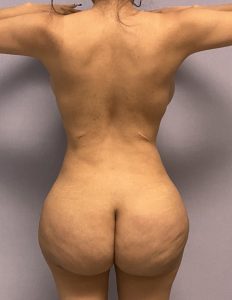


Some waistline narrowing patients have already had prior surgery to reduce their waist, most commonly BBL (Braziian Butt Lift) surgery. Even in these prior surgery patients additional waistline narrowing can be achieved by manipulation of deeper layer tissues. (muscle and ribs)

 It is not uncommon to combine other body contouring procedures with rib removal for their synergestic effect. Buttock implants is a not infrequent combination although the recovery with this combination surgery is not insignificant.
It is not uncommon to combine other body contouring procedures with rib removal for their synergestic effect. Buttock implants is a not infrequent combination although the recovery with this combination surgery is not insignificant.
A common misconception is that there is damage to internal organs during or following surgery. With ribs #12 overlying the fascia of the kidney and rib #10 close to the pleura of the lung, staying in the circumferential subperiosteal plane of the rib keeps the dissection away from these areas and makes the procedure safe. Patients report no long-term pain or any functional limitations once fully healed. Very active patients, such as gymnasts and bodybuilders, have had the procedure with full return to their strenuous activities.
A modified version of conventional rib removal surgery for waist narrowing is ‘rib breaking’ or, more accurately, surgically-assisted corseting. In this approach the ribs are not removed but undergo osteotomies (full-thickness cuts) and left in place. The patient then wears a corset afterwards to mold the ribs and soft tissues. The success of this approach is very heavily patient dependent with postoperative corset use. Whether this approach to waist narrowing is as successful as rib removals is unknown. It is also not currently known whether the recovery from this approach is any faster or has less discomfort. But given the quick recovery and surprising low level of postoperative discomfort that most patients have from rib removal surgery there is probably not much difference between the two approaches. Rib osteotomies is really for the patient who has a personal belief that keeping the rib segments in place is a more appealing waist narrowing approach for them.

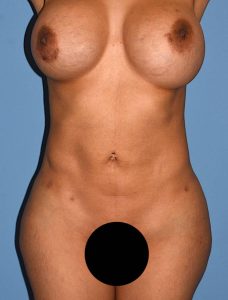
 Another type of aesthetic rib removal, Subcostal Rib Shaving, is done for anterior protrusions of the subcostal ribcage. These appear in the upper abdominal area below the breasts and create bulging prominences. They can appear on both sides or only on one side, causing a visible asymmetry. Subcostal rib reduction can be done through either a direct overlying small incision or through a tummy tuck approach at the time of a tummy tuck if that is also needed. When done as part of a tummy tuck, the prominent bulges are removed and a vertical waistline or torso lengthening is created as well.
Another type of aesthetic rib removal, Subcostal Rib Shaving, is done for anterior protrusions of the subcostal ribcage. These appear in the upper abdominal area below the breasts and create bulging prominences. They can appear on both sides or only on one side, causing a visible asymmetry. Subcostal rib reduction can be done through either a direct overlying small incision or through a tummy tuck approach at the time of a tummy tuck if that is also needed. When done as part of a tummy tuck, the prominent bulges are removed and a vertical waistline or torso lengthening is created as well.


 Subcostal rib prominence reduction can also be done by a direct incisional approach. Using a small incision like a mobile window the cartilaginous rib prominence is reduced, often using a high speed burr, leaving a thin layer of rib behind to avoid the potential for creating a contour defect that could occur from a full-thickness rib removal technique. Given the prominent location of the subcostal region patients have to consider whether a small scar is a worthy aesthetic tradeoff for the contour improvement.
Subcostal rib prominence reduction can also be done by a direct incisional approach. Using a small incision like a mobile window the cartilaginous rib prominence is reduced, often using a high speed burr, leaving a thin layer of rib behind to avoid the potential for creating a contour defect that could occur from a full-thickness rib removal technique. Given the prominent location of the subcostal region patients have to consider whether a small scar is a worthy aesthetic tradeoff for the contour improvement.
 There are also medical reasons for rib removal due to chronic pain. Non-fracture rib pain conditions are generally of two types, the costo-iliac impingement syndrome and the slipped rib syndrome. Both share two main symptoms: site-specific pain and a palpable clicking sound.
There are also medical reasons for rib removal due to chronic pain. Non-fracture rib pain conditions are generally of two types, the costo-iliac impingement syndrome and the slipped rib syndrome. Both share two main symptoms: site-specific pain and a palpable clicking sound.
 The costo-iliac impingement syndrome, also known as the rib tip syndrome, results in back and hip pain caused by the touching of the 12th rib (and occasionally the 11th rib) against the top of the hip bone. (iliac crest) It most commonly occurs in patients who have had osteoporosis of the spine and loss of vertebral height. This allows the spine to curve and bend towards one side. It can also occur in patients with congenital scoliosis as well as younger patients who have naturally longer free floating ribs or an accentuated angulation to them. The slipped rib syndrome is when the cartilage on the lower rib slips or moves leading to pain. In this rib condition a mobility of the rib usually refers to ribs #8, 9 or 10 and their cartilaginous junction with the bone. The bony rib becomes disarticulated from its more anterior cartilaginous portion. (costochondral junction separation) Mobility at the bone-cartilage junction either impinges on the intercostal nerve or causes inflammation due to periosteal/perichondrial irritation. The clicking is the two ends moving against each other. Both conditions response well to removal of the offending part of the rib.
The costo-iliac impingement syndrome, also known as the rib tip syndrome, results in back and hip pain caused by the touching of the 12th rib (and occasionally the 11th rib) against the top of the hip bone. (iliac crest) It most commonly occurs in patients who have had osteoporosis of the spine and loss of vertebral height. This allows the spine to curve and bend towards one side. It can also occur in patients with congenital scoliosis as well as younger patients who have naturally longer free floating ribs or an accentuated angulation to them. The slipped rib syndrome is when the cartilage on the lower rib slips or moves leading to pain. In this rib condition a mobility of the rib usually refers to ribs #8, 9 or 10 and their cartilaginous junction with the bone. The bony rib becomes disarticulated from its more anterior cartilaginous portion. (costochondral junction separation) Mobility at the bone-cartilage junction either impinges on the intercostal nerve or causes inflammation due to periosteal/perichondrial irritation. The clicking is the two ends moving against each other. Both conditions response well to removal of the offending part of the rib.
TORSO NARROWING by RIB REMOVAL (Type 2)
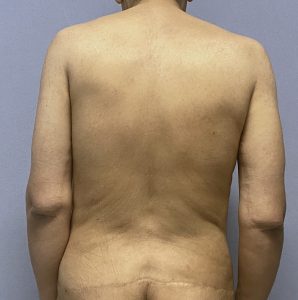
 There are two types of patients that present for waistline narrowing, cis-females and transfemales. Most cis-females that present for the surgery are often thin but lack any curves to their torso. They have usually exhausted the traditional methods for waist reshaping (liposuction, tummy tucks) or were not candidates for them. The transfemale seeks to have an improved waistline but their primary goal is really to improve their boxy torso shape due to their genetically wider ribcage. Traditional rib removal surgery offers the only anatomic change that can help but it often is less than ideal since its effects are restricted to the waistline at the horizontal umbilical level.
There are two types of patients that present for waistline narrowing, cis-females and transfemales. Most cis-females that present for the surgery are often thin but lack any curves to their torso. They have usually exhausted the traditional methods for waist reshaping (liposuction, tummy tucks) or were not candidates for them. The transfemale seeks to have an improved waistline but their primary goal is really to improve their boxy torso shape due to their genetically wider ribcage. Traditional rib removal surgery offers the only anatomic change that can help but it often is less than ideal since its effects are restricted to the waistline at the horizontal umbilical level.
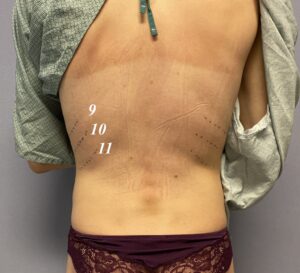 The boxy torso is due to a wider ribcage but it is not restricted to just the floating ribs. It is due to the attached ribs above the floating ribs. Ribs #9 and #10 in particular make a significant contribution and an argument can even be made for rib #8 as well. In the transfemale in particular who is seeking a more generalized torso narrowing this modified rib removal approach offers an improved approach.
The boxy torso is due to a wider ribcage but it is not restricted to just the floating ribs. It is due to the attached ribs above the floating ribs. Ribs #9 and #10 in particular make a significant contribution and an argument can even be made for rib #8 as well. In the transfemale in particular who is seeking a more generalized torso narrowing this modified rib removal approach offers an improved approach.

 The mid-lateral incision offers improved access to more rib modifications as well as more latissimus dorsi muscle removal as well. In this approach rib #12 is not treated because it is short and does not play much of a role in torso narrowing. But it could also be removed if the patient so desires as well.
The mid-lateral incision offers improved access to more rib modifications as well as more latissimus dorsi muscle removal as well. In this approach rib #12 is not treated because it is short and does not play much of a role in torso narrowing. But it could also be removed if the patient so desires as well.

 By going further top along the ribcage and removing ribs #10 and #11, shaving rib #9 and removing a long strip of latissimus dorsi muscle a torso narrowing effect is obtained.
By going further top along the ribcage and removing ribs #10 and #11, shaving rib #9 and removing a long strip of latissimus dorsi muscle a torso narrowing effect is obtained.
VERTICAL BACKLIFT RIB REMOVAL (Type 3)
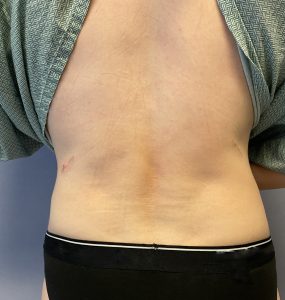
In patients who desire waistline narrowing but have loose overlying skin (such as from multiple BBL procedures or significant weight loss) the effects of any amount of rib removal are not going to be seen very well externally. Loose skin does not have the ability to shrink down around reduced structural support. Rib removal depends on taut overlying tissues to contract down around the waistline when underlying tissues are removed.
 If one has enough loose skin that it can easily be pinched or bunched up in the back the vertical backlift approach is going to produce the best waistline narrowing effect. Through a large vertical ellipse of skin removed from the back the closure of it produces a corset-like effect to pull the waistline inward. This is the definitive waistline narrowing procedure provided one can accept a long vertical scar line down the middle of the spine.
If one has enough loose skin that it can easily be pinched or bunched up in the back the vertical backlift approach is going to produce the best waistline narrowing effect. Through a large vertical ellipse of skin removed from the back the closure of it produces a corset-like effect to pull the waistline inward. This is the definitive waistline narrowing procedure provided one can accept a long vertical scar line down the middle of the spine.

 Through the vertical backlift approach ribs #11 and #12 and long wide strips of the outer latissimus dorsi muscle can be removed. Thus a total tissue removal approach can be achieved for maximal waistline narrowing.
Through the vertical backlift approach ribs #11 and #12 and long wide strips of the outer latissimus dorsi muscle can be removed. Thus a total tissue removal approach can be achieved for maximal waistline narrowing.


 While the use of a vertical excision and the long midline back scar can seem radical, for the properly selected patient it offers an unparalleled waistline body contouring change. The key, of course, is that one is willing to accept the scar as a favorable tradeoff for the most waistline change.
While the use of a vertical excision and the long midline back scar can seem radical, for the properly selected patient it offers an unparalleled waistline body contouring change. The key, of course, is that one is willing to accept the scar as a favorable tradeoff for the most waistline change.


 A vertical backlift can also be done after rib removal surgery for an even better result or it can be done as as isolated procedure without rib removal IF significant excessive skin exists.
A vertical backlift can also be done after rib removal surgery for an even better result or it can be done as as isolated procedure without rib removal IF significant excessive skin exists.



A detailed description and pictures of your concerns allow for the most informed response.
Disclaimer: By submitting a question, you agree that it may be used for educational purposes. Any identifying details or photos will be removed. Responses are general and not a substitute for medical advice.
North Meridian Medical Building
Address:
12188-A North Meridian St.
Suite 310
Carmel, IN 46032
Contact Us:
Phone: (317) 706-4444
WhatsApp: (317) 941-8237