Rhinoplasty
Rhinoplasty / Nose Surgery
At his state-of-the-art plastic surgery facility, Dr. Barry Eppley has assisted numerous rhinoplasty patients achieve their desired profile. To learn more about this procedure, please read the content below and also visit his rhinoplasty before and after pictures section.
Aesthetic vs. Functional Nose Surgery

 As one of the oldest and most common plastic surgical procedures, operations on the nose (‘nose jobs’) remain quite popular. It is important for the potential patient to make the distinction between nasal surgery which is directed towards the inside of the nose to improve breathing versus those operations which change the external shape of the nose to improve one’s appearance. Breathing difficulties of the nose frequently require a straightening of the nasal septum which is composed of cartilage (septoplasty) which may be combined with a reduction of the lower turbinate bones. (inferior turbinectomies) Changing the shape of the outside of the nose (aesthetic rhinoplasty) may involve surgery of the nasal bones (upper portion of the nose), manipulations of the cartilaginous portions of the nose (middle and lower portion of the nose), or both. Commonly, simultaneous correction of both the breathing and appearance of the nose is done in many patients and is known as a septorhinoplasty.
As one of the oldest and most common plastic surgical procedures, operations on the nose (‘nose jobs’) remain quite popular. It is important for the potential patient to make the distinction between nasal surgery which is directed towards the inside of the nose to improve breathing versus those operations which change the external shape of the nose to improve one’s appearance. Breathing difficulties of the nose frequently require a straightening of the nasal septum which is composed of cartilage (septoplasty) which may be combined with a reduction of the lower turbinate bones. (inferior turbinectomies) Changing the shape of the outside of the nose (aesthetic rhinoplasty) may involve surgery of the nasal bones (upper portion of the nose), manipulations of the cartilaginous portions of the nose (middle and lower portion of the nose), or both. Commonly, simultaneous correction of both the breathing and appearance of the nose is done in many patients and is known as a septorhinoplasty.
Anatomy of a Rhinoplasty
 The nose occupies a very small part of one’s face but yet has a very complex and intricate anatomy. Underneath the nasal skin lies bone, cartilage and an internal airway that collectively together makes up the shape and function of the nose. The outer shape of the nose is determined by the paired nasal bones (upper one-third of the nose), the paired upper lateral cartilages (middle one-third of the nose) and the paired lower alar cartilages (lower one-third of the nose). Underneath these structures is the middle support of the cartilaginous septum and the bony inferior turbinates bones which contribute to how well one breathes through their nose. Rhinoplasty surgery requires an intimate knowledge of this anatomy, how to change it and in so doing understanding how it may improve or worsen one’s nasal breathing.
The nose occupies a very small part of one’s face but yet has a very complex and intricate anatomy. Underneath the nasal skin lies bone, cartilage and an internal airway that collectively together makes up the shape and function of the nose. The outer shape of the nose is determined by the paired nasal bones (upper one-third of the nose), the paired upper lateral cartilages (middle one-third of the nose) and the paired lower alar cartilages (lower one-third of the nose). Underneath these structures is the middle support of the cartilaginous septum and the bony inferior turbinates bones which contribute to how well one breathes through their nose. Rhinoplasty surgery requires an intimate knowledge of this anatomy, how to change it and in so doing understanding how it may improve or worsen one’s nasal breathing.
Male vs. Female Rhinoplasty


Like many other parts of the face and body, it is no surprise that the shape of the nose is aesthetically different between men and women. Men like a stronger and higher nasal profile (and occasionally will even tolerate a small hump) and a nasal tip that is not too short or turned up. Conversely, women like a straight and lower nasal profile (and occasionally will even prefer a slightly concave profile) and a smaller and slightly more turned up nasal tip (more open nasolabial angle). While these are general gender nose shape trends, it is important for the rhinoplasty surgeon to have a full understanding of what the male or female patient really wants… and some patients prefer a shape that is not always in agreement with these classic gender nose shapes.
Computer Imaging in Rhinoplasty
 Before rhinoplasty surgery, it is important that one have a good appreciation of what may be changed and how your nose may look after surgery. This is done with computer imaging or simulated predictions. Dr. Eppley feels that this is essential for anyone considering rhinoplasty surgery or any form of facial reshaping surgery. Computer imaging of the nose is really about communicating what you want and having realistic expectations about the potential nose reshaping result. It is not a guarantee or an absolute assurance of what the final result will be but it does provide a general appearance of what the nose reshaping goals are. Computer imaging is also very valuable in that it may discover other helpful facial changes that can be done at the same time as your rhinoplasty of which chin augmentation or chin reduction is one of the most common.
Before rhinoplasty surgery, it is important that one have a good appreciation of what may be changed and how your nose may look after surgery. This is done with computer imaging or simulated predictions. Dr. Eppley feels that this is essential for anyone considering rhinoplasty surgery or any form of facial reshaping surgery. Computer imaging of the nose is really about communicating what you want and having realistic expectations about the potential nose reshaping result. It is not a guarantee or an absolute assurance of what the final result will be but it does provide a general appearance of what the nose reshaping goals are. Computer imaging is also very valuable in that it may discover other helpful facial changes that can be done at the same time as your rhinoplasty of which chin augmentation or chin reduction is one of the most common.
Open Rhinoplasty
 Rhinoplasty may be done either open or closed, depending upon the complexity of your surgery. When done closed, incisions are made inside the nose only and minor changes such as a small hump reduction or tip narrowing may be done. Open rhinoplasty is best done for more significant changes in the nose or if one has had prior rhinoplasty surgery. This involves a small incision across the strip of skin (columella) between your nostrils which is combined with other intranasal incisions. This scar almost always heals in an invisible manner.
Rhinoplasty may be done either open or closed, depending upon the complexity of your surgery. When done closed, incisions are made inside the nose only and minor changes such as a small hump reduction or tip narrowing may be done. Open rhinoplasty is best done for more significant changes in the nose or if one has had prior rhinoplasty surgery. This involves a small incision across the strip of skin (columella) between your nostrils which is combined with other intranasal incisions. This scar almost always heals in an invisible manner.
Hump Reduction



 One of the most common reasons for requesting a rhinoplasty, both historically and today, is to remove a hump or bump on the nose. A straight nasal profile or dorsal line is part of any aesthetically pleasing nose shape. Reducing a nasal hump requires removing both bone and cartilage that make up the hump in the upper part of the nose. In smaller humps, adequate reduction may be obtained by rasping or scraping it down. In larger humps, however, more bone and cartilage needs to be removed and this often leaves an ‘open roof’ deformity during the procedure. To close this down, the nasal bones needs to be cut (osteotomies) to allow them to fall back together for a smooth but lower nasal profile. This is what is commonly referred to as ‘breaking the nose’ and is what is primarily responsible for any bruising that occurs from rhinoplasty surgery.
One of the most common reasons for requesting a rhinoplasty, both historically and today, is to remove a hump or bump on the nose. A straight nasal profile or dorsal line is part of any aesthetically pleasing nose shape. Reducing a nasal hump requires removing both bone and cartilage that make up the hump in the upper part of the nose. In smaller humps, adequate reduction may be obtained by rasping or scraping it down. In larger humps, however, more bone and cartilage needs to be removed and this often leaves an ‘open roof’ deformity during the procedure. To close this down, the nasal bones needs to be cut (osteotomies) to allow them to fall back together for a smooth but lower nasal profile. This is what is commonly referred to as ‘breaking the nose’ and is what is primarily responsible for any bruising that occurs from rhinoplasty surgery.
Injectable Rhinoplasty for Hump Reduction

 The concept of a non-surgical or injectable rhinoplasty is mainly used for the temporary removal of a small or moderate-sized nasal hump. There are indications for other nose reshaping effects by injectable fillers (e.g. nasal tip lifting, asymmetry corrections) but nasal hump camouflage is the most common. By injecting a hyaluronic acid-based filler above the hump to fill in the space between it and the frontonasal junction, the hump ‘disappears’ as the dorsal line becomes straight. It is important to only use hyaluronic-acid based fillers as their long0term effects are assured of dissipating with very low risks of adverse inflammatory reactions.
The concept of a non-surgical or injectable rhinoplasty is mainly used for the temporary removal of a small or moderate-sized nasal hump. There are indications for other nose reshaping effects by injectable fillers (e.g. nasal tip lifting, asymmetry corrections) but nasal hump camouflage is the most common. By injecting a hyaluronic acid-based filler above the hump to fill in the space between it and the frontonasal junction, the hump ‘disappears’ as the dorsal line becomes straight. It is important to only use hyaluronic-acid based fillers as their long0term effects are assured of dissipating with very low risks of adverse inflammatory reactions.
Nose Tip Reshaping


 The shape of the tip of the nose is as variable as one’s fingerprints. The size and shape of the lower alar cartilages, how they join (or don’t join) in the middle, the length of the underlying nasal septum and the thickness of the overlying skin all contribute to how the tip of the nose looks. The most common tip concerns are those that are too wide or round, too long and droopy or twisted and asymmetrically shaped.
The shape of the tip of the nose is as variable as one’s fingerprints. The size and shape of the lower alar cartilages, how they join (or don’t join) in the middle, the length of the underlying nasal septum and the thickness of the overlying skin all contribute to how the tip of the nose looks. The most common tip concerns are those that are too wide or round, too long and droopy or twisted and asymmetrically shaped.

 As a result, tip reshaping in rhinoplasty surgery offers the greatest number of potential nose shape changes . Most commonly the lower alar cartilages are reduced in size and put back together to make the nose tip more narrow and refined. To prevent long-term nose tip changes with healing and scar contracture, a cartilage graft is often used to support the newly shaped tip, like a tentpole, and is known as a columellar strut graft. How the tip is sutured to this central support has a major influence on the final tip shape.
As a result, tip reshaping in rhinoplasty surgery offers the greatest number of potential nose shape changes . Most commonly the lower alar cartilages are reduced in size and put back together to make the nose tip more narrow and refined. To prevent long-term nose tip changes with healing and scar contracture, a cartilage graft is often used to support the newly shaped tip, like a tentpole, and is known as a columellar strut graft. How the tip is sutured to this central support has a major influence on the final tip shape.
Shortening the Long Nose



 The long nose is typically associated with overgrowth of the septum, excessively large tip cartilages, or a combination of both. This results in either the tip being pushed outward beyond the dorsal line (too much tip projection) or the tip is pushed down creating an elongated appearance. (lack of adequate tip rotation) In essence the tip is just too big for the rest of the nasal framework. Often the bridge of the nose is also high, reflective of the underlying large cartilage structure. Shortening the long nose requires reducing the length of the lower alar cartilages and/or the caudal end of the septum as well. The rest of the nose must then be put in balance with the new tip length.
The long nose is typically associated with overgrowth of the septum, excessively large tip cartilages, or a combination of both. This results in either the tip being pushed outward beyond the dorsal line (too much tip projection) or the tip is pushed down creating an elongated appearance. (lack of adequate tip rotation) In essence the tip is just too big for the rest of the nasal framework. Often the bridge of the nose is also high, reflective of the underlying large cartilage structure. Shortening the long nose requires reducing the length of the lower alar cartilages and/or the caudal end of the septum as well. The rest of the nose must then be put in balance with the new tip length.
Lengthening/Building Up the Short Nose


 Unlike the long nose which occurs due to natural development, the short nose deformity is often the result of either a traumatic injury or the result of a prior over aggressive rhinoplasty. It occurs due to the loss or removal of underlying cartilage and/or bone support. Thus, building out the nose always requires the use of cartilage grafts from the septum, ear or rib depending upon how much graft material is needed. This could involve graft placement on just the tip of the nose (columella and tip), the dorsal bridge or a combination of dorso-columellar augmentation.
Unlike the long nose which occurs due to natural development, the short nose deformity is often the result of either a traumatic injury or the result of a prior over aggressive rhinoplasty. It occurs due to the loss or removal of underlying cartilage and/or bone support. Thus, building out the nose always requires the use of cartilage grafts from the septum, ear or rib depending upon how much graft material is needed. This could involve graft placement on just the tip of the nose (columella and tip), the dorsal bridge or a combination of dorso-columellar augmentation.
Broad/Wide Rhinoplasty



 A broad nose is perceived from the front view in which the nose looks wide compared to other facial features. In particular, it refers to a variety of nose shapes in which the lower third of the nose is almost as wide or equal to a vertical line dropped down from the inner corner of the eye. This can occur in isolation due to separate or combined issues of widely separated/enlarged dome cartilages, flared nostrils and/or thick skin. Or it affects the whole nose in combination with a wide upper and middle third of the nose which is primarily influenced by the width of the nasal bones. Making the broad nose more narrow requites a variety of techniques including nasal bone osteotomies, tip narrowing/reshaping, nostril width reduction and, in some underdeveloped noses dorsal and tip augmentation.
A broad nose is perceived from the front view in which the nose looks wide compared to other facial features. In particular, it refers to a variety of nose shapes in which the lower third of the nose is almost as wide or equal to a vertical line dropped down from the inner corner of the eye. This can occur in isolation due to separate or combined issues of widely separated/enlarged dome cartilages, flared nostrils and/or thick skin. Or it affects the whole nose in combination with a wide upper and middle third of the nose which is primarily influenced by the width of the nasal bones. Making the broad nose more narrow requites a variety of techniques including nasal bone osteotomies, tip narrowing/reshaping, nostril width reduction and, in some underdeveloped noses dorsal and tip augmentation.

 One potential feature of wide nose is flaring nostrils. This can be treated by various techniques of nostril reduction, either as an isolated procedure or more commonly as part of an overall nose reshaping surgery.
One potential feature of wide nose is flaring nostrils. This can be treated by various techniques of nostril reduction, either as an isolated procedure or more commonly as part of an overall nose reshaping surgery.
Ethnic Rhinoplasty

 The concept of an ethnic rhinoplasty is a bit misleading as it comes from the perspective of Caucasian nose standards or shapes… and not every non-Caucasian rhinoplasty patient necessarily desires a more western-shaped nose. But many African-American, Hispanic, Asian and Middle Eastern patients who desire nose changes do strive for smoother and higher nasal profiles, removal of humps or bumps, a more narrow and projected nasal tip and nostrils that are not too wide or flared.
The concept of an ethnic rhinoplasty is a bit misleading as it comes from the perspective of Caucasian nose standards or shapes… and not every non-Caucasian rhinoplasty patient necessarily desires a more western-shaped nose. But many African-American, Hispanic, Asian and Middle Eastern patients who desire nose changes do strive for smoother and higher nasal profiles, removal of humps or bumps, a more narrow and projected nasal tip and nostrils that are not too wide or flared.

 In considering rhinoplasty for patients of various ethnicities, it is critically important to use computer imaging and establish a clear understanding of exactly what nasal shape changes the patient desires and not to try and overly ‘westernize’ their nasal appearance. For some patients, cartilage grafts or implants will be needed to provide the amount of nasal augmentation that they desire.
In considering rhinoplasty for patients of various ethnicities, it is critically important to use computer imaging and establish a clear understanding of exactly what nasal shape changes the patient desires and not to try and overly ‘westernize’ their nasal appearance. For some patients, cartilage grafts or implants will be needed to provide the amount of nasal augmentation that they desire.
Congenital and Cleft Rhinoplasty

 There are a large variety of congenital birth defects that affect the nose, but none is more common than that of cleft lip and palate due to its birth defect rate. While the cleft may affect the lip and palate most noticeably, the overlying nose is also highly affected with septal deviations, tip asymmetries, nasal bone deviations and deficiencies of the underlying platform of bone on which the nose rests. (maxilla, paranasal base) Unlike the more common aesthetic rhinoplasty, the cartilage, bone and skin of the cleft nose is not normal and is different in both amounts and shape. This makes the cleft rhinoplasty one of the most challenging forms of nose reshaping surgery in an effort to take what is abnormal and make it look more normal. In addition, there are often significant breathing problems that must be simultaneously addressed due to the internally deranged septum and enlarged turbinates.
There are a large variety of congenital birth defects that affect the nose, but none is more common than that of cleft lip and palate due to its birth defect rate. While the cleft may affect the lip and palate most noticeably, the overlying nose is also highly affected with septal deviations, tip asymmetries, nasal bone deviations and deficiencies of the underlying platform of bone on which the nose rests. (maxilla, paranasal base) Unlike the more common aesthetic rhinoplasty, the cartilage, bone and skin of the cleft nose is not normal and is different in both amounts and shape. This makes the cleft rhinoplasty one of the most challenging forms of nose reshaping surgery in an effort to take what is abnormal and make it look more normal. In addition, there are often significant breathing problems that must be simultaneously addressed due to the internally deranged septum and enlarged turbinates.

 Cleft rhinoplasty is really a continuum of nose reshaping efforts throughout growth and development that often begin at the time of the initial cleft lip and palate repairs. These early efforts are more limited procedures just for tip and nostril reshaping that will culminate in the teen or adult years as a more complete septorhinoplasty effort.
Cleft rhinoplasty is really a continuum of nose reshaping efforts throughout growth and development that often begin at the time of the initial cleft lip and palate repairs. These early efforts are more limited procedures just for tip and nostril reshaping that will culminate in the teen or adult years as a more complete septorhinoplasty effort.
Teenage Rhinoplasty

 One of the most common cosmetic surgeries for teenagers, both past and present, is rhinoplasty. Since the nose is is centered in the middle of the face and plays a major role in its appearance, self-image concerns about the shape of the nose can begin soon after puberty. Due to development or traumatic injury, a teen may also have breathing problems through their nose due to septal deviation or turbinate enlargement. Rhinopasty in teens can offer significant improvement in both the appearance and function of the nose. The most relevant questions in teenage rhinoplasty or septorhinoplasty is what is the earliest age at which it can be done. While there are no absolutes and each patient must be considered individually, the age of 14 for females and 15 for makes are general guidelines.
One of the most common cosmetic surgeries for teenagers, both past and present, is rhinoplasty. Since the nose is is centered in the middle of the face and plays a major role in its appearance, self-image concerns about the shape of the nose can begin soon after puberty. Due to development or traumatic injury, a teen may also have breathing problems through their nose due to septal deviation or turbinate enlargement. Rhinopasty in teens can offer significant improvement in both the appearance and function of the nose. The most relevant questions in teenage rhinoplasty or septorhinoplasty is what is the earliest age at which it can be done. While there are no absolutes and each patient must be considered individually, the age of 14 for females and 15 for makes are general guidelines.
Silver (Older) Rhinoplasty

 While many envision that rhinoplasty is an operation that is done on young people to change the shape of the nose they were born with, older patients (ages 60 and above) are increasing undergoing rhinoplasty. While it may be for a nose that they have never liked, often it is for a nose that has aged or dropped. There is an old saying that the nose gets longer as we get older, and this is true, but it is not due to ongoing growth. Rather it is due to the ligaments that hold the tip cartilages up begin to weaken and the nasal tip drops. This makes the total nasal length longer and leads to an aesthetically unpleasing downward turn of the nasal tip (lessening of the nasolabial angle). Rhinoplasty for the droopy aging tip can have a facial rejuvenative effect and can turn a long downturned tip into a more uplifted one.
While many envision that rhinoplasty is an operation that is done on young people to change the shape of the nose they were born with, older patients (ages 60 and above) are increasing undergoing rhinoplasty. While it may be for a nose that they have never liked, often it is for a nose that has aged or dropped. There is an old saying that the nose gets longer as we get older, and this is true, but it is not due to ongoing growth. Rather it is due to the ligaments that hold the tip cartilages up begin to weaken and the nasal tip drops. This makes the total nasal length longer and leads to an aesthetically unpleasing downward turn of the nasal tip (lessening of the nasolabial angle). Rhinoplasty for the droopy aging tip can have a facial rejuvenative effect and can turn a long downturned tip into a more uplifted one.
Reconstructive Rhinoplasty (Nasal Fracture Repair)



 Injuries to the nose are very common as the protrusion of the nose makes it the most easily injured part of the face. Because the cartilage of the nose (which makes up the lower 2/3s) is very flexible, it is very resilient to injury. But the upper part of the nose is bone and is commonly fractured. Displacement of the nasal bones is what makes up the ‘fractured nose’ most of the time although the underlying supportive septum is often displaced as well. The repair of nose fractures is a more scaled down version of a rhinoplasty in that the broken bones are moved back in place and the septum is repositioned if necessary. This is generally done within several weeks of the injury when much of the swelling and bruising has resolved and the extent of the nasal deformity is evident.
Injuries to the nose are very common as the protrusion of the nose makes it the most easily injured part of the face. Because the cartilage of the nose (which makes up the lower 2/3s) is very flexible, it is very resilient to injury. But the upper part of the nose is bone and is commonly fractured. Displacement of the nasal bones is what makes up the ‘fractured nose’ most of the time although the underlying supportive septum is often displaced as well. The repair of nose fractures is a more scaled down version of a rhinoplasty in that the broken bones are moved back in place and the septum is repositioned if necessary. This is generally done within several weeks of the injury when much of the swelling and bruising has resolved and the extent of the nasal deformity is evident.
Implants vs. Rib Grafts in Rhinoplasty

 One of the classic ‘controversies’ in rhinoplasty is whether to use the patient’s own cartilage (graft) or a synthetic material (implant) when significant nasal augmentation is needed. There are advantages and disadvantages to both grafts and implants and there are surgeons who have strong beliefs with the use of either one. With good patient selection and careful surgical technique both grafts and implants can be used successfully. In general it is always best long-term to use the patient’s own cartilage. Donor sites include the septum, ear and rib but sometimes due to donor site inadequacy/depletion or the patient’s desire to avoid a donor harvest (usually from the rib), implants become necessary. The one major advantage that implants have is in significant augmentations where their preformed shapes allow for a predictable volume effect that is very likely to be straight and smooth. It is never a good idea, however, to use an implant to significantly push upward on the nasal tip skin as skin thinning and eventual erosion may occur. The restriction of implant placement to the bridge of the nose and using preformed ePTFE or hand carved solid ePTFE material ensures good clinical outcomes.
One of the classic ‘controversies’ in rhinoplasty is whether to use the patient’s own cartilage (graft) or a synthetic material (implant) when significant nasal augmentation is needed. There are advantages and disadvantages to both grafts and implants and there are surgeons who have strong beliefs with the use of either one. With good patient selection and careful surgical technique both grafts and implants can be used successfully. In general it is always best long-term to use the patient’s own cartilage. Donor sites include the septum, ear and rib but sometimes due to donor site inadequacy/depletion or the patient’s desire to avoid a donor harvest (usually from the rib), implants become necessary. The one major advantage that implants have is in significant augmentations where their preformed shapes allow for a predictable volume effect that is very likely to be straight and smooth. It is never a good idea, however, to use an implant to significantly push upward on the nasal tip skin as skin thinning and eventual erosion may occur. The restriction of implant placement to the bridge of the nose and using preformed ePTFE or hand carved solid ePTFE material ensures good clinical outcomes.
Transgender (Male to Female) Rhinoplasty
![]()
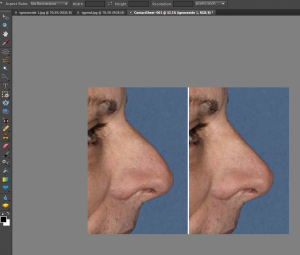
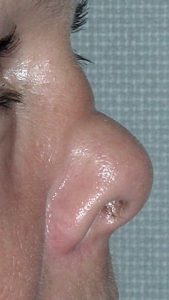
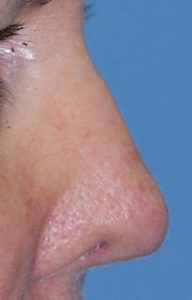
![]() Creating a more feminine nose shape focuses on several specific changes of the dorsum (bridge) and the tip. A straight or slightly concave dorsal profile with a narrow tip that has adequate rotation for a more open nasolabial angle (greater than 90 degrees) is preferred. Lowering the central dorsum to create a slight saddle appearance and having a significant tip rotation, and tip shortening, if necessary, has a very feminizing effect. Good tip rotation is important but should not be done so much that excessive nostril show occurs. An open rhinoplasty is usually needed to reliably achieve this form of nose shape change. Because in most male to female rhinoplasties it is a reductive operation extensive cartilage grafting is not needed. But support for the tip and possibly the middle vault as well are commonly used.
Creating a more feminine nose shape focuses on several specific changes of the dorsum (bridge) and the tip. A straight or slightly concave dorsal profile with a narrow tip that has adequate rotation for a more open nasolabial angle (greater than 90 degrees) is preferred. Lowering the central dorsum to create a slight saddle appearance and having a significant tip rotation, and tip shortening, if necessary, has a very feminizing effect. Good tip rotation is important but should not be done so much that excessive nostril show occurs. An open rhinoplasty is usually needed to reliably achieve this form of nose shape change. Because in most male to female rhinoplasties it is a reductive operation extensive cartilage grafting is not needed. But support for the tip and possibly the middle vault as well are commonly used.
‘Extraordinary’ Rhinoplasty


 There are instances where patients may request an uncommon or an extraordinary rhinoplasty outcome. This is where the patient desires a nose shape that falls outside the traditional concepts of nose shape and proportionate relationships. One such example is that of the ‘Barbie Nose’ in which the middle third of the nose has more of a saddled appearance and where the upturn of the nasal tip (nasolabial angle) exceeds the upper end of the normative value. (110 degrees) From a conventional rhinoplasty perspective this represents an overdone or over reduced nose in which risks do exist for nasa airway compromise and excessive nostril show. But with good cartilage support (spreader grafts and columellar strut and alar rim grafts, such a result can be obtained without adversely affecting nasal airway function.
There are instances where patients may request an uncommon or an extraordinary rhinoplasty outcome. This is where the patient desires a nose shape that falls outside the traditional concepts of nose shape and proportionate relationships. One such example is that of the ‘Barbie Nose’ in which the middle third of the nose has more of a saddled appearance and where the upturn of the nasal tip (nasolabial angle) exceeds the upper end of the normative value. (110 degrees) From a conventional rhinoplasty perspective this represents an overdone or over reduced nose in which risks do exist for nasa airway compromise and excessive nostril show. But with good cartilage support (spreader grafts and columellar strut and alar rim grafts, such a result can be obtained without adversely affecting nasal airway function.
Revision Rhinoplasty

 Despite a plastic surgeon’s best efforts, not every rhinoplasty surgery turns out to meet a patient’s expectations. This can occur from a variety of reasons but most commonly is due to some aspect of the shape be less than desired. The skin of the nose does not always shrink and adapt well to the underlying bone and cartilage framework and may develop thick scarring or scar distortions. There may also be residual asymmetries of the bone or cartilage edges.
Despite a plastic surgeon’s best efforts, not every rhinoplasty surgery turns out to meet a patient’s expectations. This can occur from a variety of reasons but most commonly is due to some aspect of the shape be less than desired. The skin of the nose does not always shrink and adapt well to the underlying bone and cartilage framework and may develop thick scarring or scar distortions. There may also be residual asymmetries of the bone or cartilage edges.
The risk of revisional rhinoplasty is estimated to be around 10% to 15% but that is an average number which does not take into account the original nasal problem. Suffice it to say every rhinoplasty patient needs to know that such a risk exists. Nose surgery takes a while to see the final result and scar tissue needs to soften before any effort at revisional surgery is attempted. For this reason, revisional rhinoplasty is not usually done for six months to one year after the original surgery.
Rhinoplasty with Chin Augmentation
The nose does not exist in isolation from the rest of the face. Changing its shape should be done with the consideration of how it influences other facial features and/or how changing other facial features with a rhinoplasty makes for a more proportioned and balanced face. The classic dual facial reshaping operation is rhinoplasty with chin augmentation. Many larger noses have small chins so making the nose smaller and the chin bigger can dramatically change one’s facial profile. Rhinoplasty can be done with almost any other facial plastic survey procedure, however, from cheek augmentation, facelifts and blepharoplasties to create optimal facial shape improvement.
Before Rhinoplasty Surgery
Patients that are considered for rhinoplasty must be of sufficient age. Usually, patients must be at least 12 to 13 years of age so that the nose may be near full development so that surgery will not interfere with its growth. In addition, the maturity that comes with an older age helps ensure that the desired nasal changes are based on the patient’s own feelings rather than that of others or from trendy looks.
Conversely, there is no older age at which rhinoplasty cannot be performed. In the older patient, it is not uncommon to perform rhinoplasty with other procedures such as a facelift or eyelid lift / brow surgery. For the older patient who often has a drooping nasal tip, a rhinoplasty that creates tip rotation and elevation can create a more youthful look.
Patients that have the following nasal problems may be candidates for surgery:
- bump on the bridge of the nose
- wide bridge of the nose
- wide nostrils
- thick or full nasal tip
- drooping nasal tip
- crooked nose
- nose that is too big for the rest of your face
- difficulty in nasal breathing that is not associated with allergies
In consultation, a thorough medical history will be taken with emphasis on any history of bleeding problems or difficulty breathing through the nose. Medications that may interfere with the ability of the blood to clot (e.g., aspirin) or the use of nasal sprays or decongestants will also be noted. It is extremely important to very specifically identify what about your nose you do not like or exactly which parts you want to be changed. This is usually done in front of a mirror at the time of your consultation. The nose will then be examined by feeling its outer structures and breathing through the nostrils tested. Photographs will then be taken to more fully evaluate your nose and its relationship to your face and to determine if other procedures (e.g., chin surgery) may also be helpful to provide better facial balance and proportions.
It is important to understand that not every patient can achieve the same result from rhinoplasty surgery. Good results are usually obtained, however, when the surgeon and patient have a mutual and realistic understanding of the goals and expectations from the procedure. Also, one cannot get a nose that looks like someone else’s such a celebrity or model, you can only make your own unique nose more aesthetically pleasing and proportionate.
The Rhinoplasty Operation
Nasal surgery is always performed under general anesthesia, never requires hospitalization and is usually done in an outpatient surgery center setting.
Many aspects of the nose can be altered (e.g., lowering the nasal bridge, narrowing the nostrils or the tip of the nose) and the specific technique will be determined by Dr. Eppley. Most structures of the nose are best approached through an external approach known as an open rhinoplasty. Through the use of a small incision across the vertical strip of skin between the nostrils, known as the columella, the skin can be gently lifted off the nose. This open approach permits a direct view of the complex cartilage and bone structures that comprise the majority of the nose and for this reason is more commonly used today. This very small incision usually heals without a noticeable scar. In some cases of minor nasal changes or revisions, incisions may only be done on the inside of the nose (endonasal approach).
The only other external scars from rhinoplasty occur when the width of the nostrils is narrowed at the attachment of the nostrils to the upper lip (nostril narrowing). These scars are quite small and most of them lie just inside of the nostril.
After Rhinoplasty Surgery
After the surgery is completed, dressings are placed on the nose, which consist of tapes and a splint. This splint helps hold the tissues in place while healing is occurring as well as protects the nose during sleep and against accidental bumps. Packing of the inside of the nose is almost never done anymore.
After adequately recovering from the anesthesia, the patient is discharged to home with instructions to sleep with the head up on several pillows and limit one’s activities. Antibiotics and decongestant prescriptions will be given to take as directed.
Bruising and swelling around the nose and eyes is quite variable but can be expected to be completely gone anywhere from ten to twenty-one days after surgery. Minor residual nasal swelling, however, may persist for several months and the final subtler aspects of the nasal shape may not completely be settled for three to six months after surgery. The nasal tapes and splint is removed at one week after surgery during the first postoperative visit. No sutures need to be removed as they are dissolvable.
Significant complications from rhinoplasty are rare. Bleeding and infection are quite uncommon. The most common complications are subsequent asymmetries in nasal shape and form. Revisional surgery may be needed in up to 10% of rhinoplasty surgery to optimize the result. Such revisional rhinoplasties are not done for at least six months after the initial procedure to allow all tissues to heal and all swelling to be completely gone.



A detailed description and pictures of your concerns allow for the most informed response.
Disclaimer: By submitting a question, you agree that it may be used for educational purposes. Any identifying details or photos will be removed. Responses are general and not a substitute for medical advice.
North Meridian Medical Building
Address:
12188-A North Meridian St.
Suite 310
Carmel, IN 46032
Contact Us:
Phone: (317) 706-4444
WhatsApp: (317) 941-8237