Your Questions
Your Questions
Q: Dr. Eppley, just curious if you had testicular enhancement procedures. I am 34 years old and on TRT for the past 3 years and got little nuts now lol.
A: Most testicular enhancement procedures use a side by side by side techniques using custom testicle implants in the 6.0 to 7.0cm size range. While the natural testicles can be removed, the side by side technique keeps them in place and the larger implants displace them from view.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, How can I help my head to be smaller?
A: While certain areas of the head/skull can be reduced to change its shape and make it appear a bit slimmer/smaller. How that applies to you I can not say based on your inquiry, this requires a specific description of your head shape concerns along with pictures that so illustrate.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
How Can I Improve The Prominence Infraorbital Rim Appearance After PEEK Infraorbital-Malar Implants?
Q: Dr. Eppley, In January I had double jaw surgery for sleep apnea along with a saddled PEEK implant to the infraorbital zygomatic region. I was wondering if it is possible to resolve my issues with the implant without removing them. While the shape of the implant seems natural enough, in certain lighting the implant shows through the skin and there is a very deep hollow between the undereye and the orbital rim. Does it look possible to smooth out with fat grafts or will I need it removed or replaced?
A: Whlle I haven”t seen your PEEK infraorbital-zygomatic implants design what I can see is that the infraorbital component is prominent which is a design and material issue. But assuming every other aspect of the implant’s effect you like it would make the most send to try and camouflage the issue rather than directly treat it. (total implant replacement) The options for infraorbital camouflage include injectable fat grafting or ePTFE sheet implant overlay.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I got newer implants with a breast lift that left me with bad keloid scarring about 2 years ago. I’ve tried topicals but I’m not seeing much of a difference. The scars are worse due to the fact I was allergic to the stitches and it caused sores which took longer to heal. I’m including a pic of the lower part of my breast. I don’t know if these can be removed but I wanted to ask because it has really affected the way I feel about my body in a bad way. Please let me know if you can help. I live in TN and I don’t want to travel for surgery unless you think you can drastically reduce these scars. Thank you
A: With wide hypertrophic scarring topical treatments will not be effective. The only effective treatment is to cut out all of the scars and reclose it to bring ubnscarred skin edges back together. (secondary breast lift) It would be helpful to know how the incisions were initially closed which should be in the original operative note. In addition this also raises the question of what does your original surgeon say about improving the scarring since what I am suggesting is not novel…it is the only path to improvement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, How can the scars from may facelift be improved?
A: Thank you for sending your pictures. Your facelift scarring shows multiple issues which includes:
1) hypertrophic anterior scarring
2) trapped right earlobe skin
3) left pixie ear (pulled down scarring
4) bilateral anterior displaced preauricular scars
Like all secondary problems it is helpful to know exactly how the issues occurred so they could be avoided the next time. While you nor I will never know the exact details of your facelift (what was done under the hood so to speak), and I wouldlike to read the operative note from the surgery, I do know the following:
1) To be successful with the anterior (preauricular) scarring the facelift flaps must be re-raised ad the closure line moved back into a retotragal position which is more consistent with a female facelift. This will also hide some of the closure and give the rest of the anterior scarring a chance to heal better.
2) The elongated left earlobe is a form of pixie ear in which the scar pulls down on the earlobe, lengthens it and then shows visible scsarring below the earlobe. This again supports re-raising the facelift flaps.
3) For whatever reason there appears to be trapped earlobe skin/tissue in the closure line, hence the hole.
When you put all this together the only successful strategy is to redo the facelift…this time with deeper tissue support and different scar placement. (retrotragal) Management of facelift scars rarely is as simple as just cutting out the scars and closing. It almost always requires some or all re-elevation of the facelift flaps and a deeper method tio better distribute the forces onj the incisional closure. This becomes paramount because the ‘easy’ tissue laxity has been removed and now the tissues are scarred and less mobile.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello there, so I’m trying to see waistline reduction for a specific measurements, I’ve already removed the 12th, 11th, and the 10th rib previously. Had liposuction and I still have yet to achieve the proper results that I’m looking for. I was wondering what you might suggest.
A: Whether you can ever achieve the waist narrowing results you are striving for is up for debate. But what is clear is that the last anatomic barrier to what is possible is skin. The rolls of skin on your back indicate significant laxity for which a vertical backlift can have a definitive torso narrowing effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, can you please let me know the cost of brow bone implant? I’m trying to figure out whether it’s more cost effective to have done in the States or in Thailand. Thanks
A:In reply to your inquiry I can make the following comments:
 1) You can not just have a brow bone implant alone as your forehead is significantly recessed as that will make it look unusual. You need a combined forehead-brow bone implant to bring the entire upper third of your face foreward. (see attached imaging as well as implant design)
1) You can not just have a brow bone implant alone as your forehead is significantly recessed as that will make it look unusual. You need a combined forehead-brow bone implant to bring the entire upper third of your face foreward. (see attached imaging as well as implant design)
2) The augmentation would have to extend down into the nasal radix area to avoid the nasofrontal angle from becoming too deep.
3) The question is never whether it will cost less in Thailand…as that will always be true. The real question is what will be the result differences.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can’t figure out what’s going on, I think somehow my maxilla is too small or something.
A:You have two fundamentally different paths to go down:
1) Treat the underlying maxillomandibular deficiency with Bimax advancements (upper and lower jaw advancement surgery – see attached imaging)
2) Leave the maxilla and mandible (jaw bones) where they are and do a camouflage approach with either either chin augmentation alone (implant vs sliding genioplasty) or total jaw augmentation with a custom implant. (perhaps even with a rhinoplasty to help de-rotate the tip of the nose) (see attached imaging)
There is no right or wrong here. It is all about what final aesthetic result do you want and how effort do you want to put in to achieve it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’d be interested to know the approximate price of standard infraorbital rim implants and the price of custom ones as well. The lid retraction is genetic I’ve never had any surgery near my eyes. My goal would be to get rid of my sceleral show, improve my negative orbital vector and get rid of the darkness under my eyes.
A: It is important to be aware that standard infraorbital and custom Infraorbital implants do not have the exact dimensional effects. (customs saddle the rims while standard implants do not which will affect how they treat a specific problem particular in congenital scleral show)
While implants have a role to play in the treatment of scleral show and eye corner reshaping they must be combined with lateral canthoplasties and spacer grafts for the lower eyelids to be maximally effective. Natural scleral show is a reflection of underlying tissue deficiencies which includes bone and soft tissues. Unless all are addressed either a failed or inadequate result will occur. As a result you can see why the combination of implants (bone augmentation), spacer grafts (lower eyelid vertical tissue addition) and lateral canthoplasties (coner repositioning) is ideally needed.
Thus you have to look at implants as part of the solution but not the total solution.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, when I had the genioplasty in SK, there is a noticeable dent on the edge of my jaw that creates the look of a ‘jowl’. One side of my face is much more shaved down than the other, making it appear full, the same side with the genioplasty dent, and it makes me very insecure still.
I would also like a little bit of extra jaw angle on the side that is still a greater size, to create a more pointed edge, as well as more chin projection horizontally, and probably nothing vertically. Although, the length of my face may be an illusion due to how narrow it is with the lack of a proper jaw angle. I was also wondering if I could get paranasal implants for my nasolabial folds. I realize this is a lot of different procedures, but I know you are the best when it comes to implants, and after seeing how much difference the cheek implants have made in my face, you would be able to help me. Thank you so much
A: It is easy to see in your postop x-ray the very significant left jawline/chin deficiency which is present to which a custom jawline implant is the only effective method to improve it. That can certainly be combined with a right jaw angle implant to achieve your desired effects. Getting both sides of the jawline augmented and even/symmetric is the exact role that the custom implant design process is suited to do.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to get an aesthetic metopic ridge reduction surgery. 39M.Can I have more details about the procedure, like cost, what to expect, etc? I think I was born with a minor form of trigocephaly (metopic craniosystosis).
A:I believe your supposition is correct in that your midline ridge is a microform of metopic synostosis…as that would be the only explanation for why it is there. Burring reduction would be an appropriate treatment for it provided the bone is thick enough to do so. Usually it is since in synostoses the suture line is thickened not thinner. But it is always a good idea to check a 2D scan to know for sure.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello I had a facelift over a year ago with a neck lift. I have been getting injections on my scars but they still haven’t helped. Is there anyway I can get some information on possibly getting treated?
A:These are significant hypertrophic scars for which injections are not going to be effective. The only effective approach is to cut out the scars, re-elevate the facelift skin flaps, and do an extended SMAS or deep plane lift/support. This is the way you keep all the tension off the closure line and then they will heal without the hypertrophy and pixie ear deformities that you have. There is no ‘little’ way to fix this problem. While the injections have not been harmful they are just buying time to get to what really needs to be done and at one year postop that can now been done at any time.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Would like to have a slimmer non round shaped face? What is your recommendation and costs associated. would like a flatter chest, smaller muscle and shoulder blades that don’t stick out so much.
Head Width Reduction
Temple Reduction/Bone Reduction
Check bone Reduction
V-shaped Jaw Surgery
Chin Implant
Shoulder Blade Reduction
Chest Reduction
Trapezius Reduction
A: This is a long list of desired procedures for which I can summarize my opinions as follows:
1) Unless one is having clavicle shortening (shoulder narrowing) there is little sense to scapular and trapezius reductions. So I would eliminate the body procedures minus the chest reduction which is really chest liposuction/areolar gynecomastia reduction.
2) The lowest hanging fruit on the face, so to speak, is the chin augmentation. This is at least 10 to 12mms of advancement for which a sliding genioplasty is the appropriate procedure. (see attached) This forward movement will also make the jaw more narrow in appearance so this is your V line procedure not the whole jawline. (see attached imaging)
3) You have a wide face which starts at the skull and goes down through the cheeks but, as part of that development, your eyes are also widely spaced. (type 1 hypertelorism) As a result you don’t want to try and narrow your face aggressively as that will just make the eyes look even wider apart. I think the skull/temporal reduction is beneficial but I would leave the cheeks alone. (see attached imaging)
In conclusion, a sliding genioplasty with type 4 temporal reductions and possibly chest liposuction is what I would recommend.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in getting some custom cheek implants. I wondered if you could send through some before and after pictures of males with implants that add Malar projection with the sizes? I believe I’m looking at 5mm of projection.
A:Due to patient confidentiality I don’t pass out patient pictures. (I suspect you would not want your pictures passed around randomly either) But that issue aside other people’s results and implant dimensions have little actual correlation to someone else based on anatomy and aesthetic preferences. What matters is what is the patient’s specific cheek augmentation preference/target is? That can only be determined by computer imaging of the patient’s pictures to determine their range of change tolerance. I don’t how you have picked the 5mm thickness number. Buit unless one has gone through the imaging exercise to develop a feel for the change the patient is seeking there is no way to know the relevance of any specific implant dimension.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,Would a genioplasty/sliding genioplasty have different look affect or roughly the same?
A:If you are referring to how it looks horizontally or in the side view an implant and sliding genioplasty will look the same as long as they are in the under 10mm movement range. It is in the front view where they may look potentially different as a chin implant can make the chin wider or more square if desired while a sliding genioplasty can not.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am writing this email to share my concerns about a craniofacial asymmetry that has been bothering me. I was born as a preterm baby and I was hospitalised for over two months due to low birth weight and complications from hydrocephaly. Since my childhood, I have been extremely conscious about my prominent ears. I also had dental malocclusion, which bothered me as I believed that it contributed to my lopsided smile but otherwise, there were no complications in speech or eating. In 2011, I underwent orthodontic treatment and in 2013, I had otoplasty to correct my prominent ears. While the otoplasty dramatically improved my appearance, I noticed that my left ear was slanted at an angle “\” while my right ear seemed perfect. I underwent two revision otoplasty till 2014 to unsuccessfully resolve this issue. I then decided to let the matter rest.
My first orthodontic treatment concluded in 2014, by my lopsided smile remained and I am still undergoing orthodontic treatment to this date to correct a mild occlusal cant. I have had consultations with oral and maxillofacial surgeons in 2016 and they ruled out jaw asymmetry.
I have spent the past decade trying to understand the factors contributing to my facial asymmetry. The issue that bugs me the most to date is my lopsided left ear.
I used to go to a hairdresser regularly, who pointed out that my head is asymmetrical – my left side is convex, and the back was apparently “flatter”. Frankly speaking, I have never noticed the latter. I started reading up on cranial asymmetry and I eventually realized that the issues I have are most likely linked to plagiocephaly.
It seems like a hopeless cause, and I am not sure if anything can be done to correct my facial asymmetry. I hope something can be done to bring some harmony between the left and right ear and correct my lopsided smile.
A: In answer to your ear and facial asymmetry questions:
1) You have correctly surmised that changing the position of the ears vertically is not possible as your two previous attempts to do so have failed. Thus leaving them alone is the appropriate choice.
2) Conversely the skull and facial asymmetries are very improvable as your 3D CT scan shows the bony asymmetries of the right back of the head and the left cheek and jawline for which custom implant designs treat those very effectively.
3) The lopsided smile (one mouth corner higher than the other) is challenging since there is no good way to lower the higher left mouth corner side.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley For webbed neck correction apart from the aesthetic aspect, I wonder if I would be more flexible in terms of mobility? Also, is such an operation performed under general anesthesia or twilight sleep?How long does it take to fully recover and when would I be allowed to do sports again? What are the risks of the operation?
A:First and foremost the purpose of the imaging is to show that normalization of the neck shape can never be achieved completely…improvement is seen but the webs are never completely eliminated. If one sees the imaging as not enough change then the surgery is not for them. Imaging is, in essence, a patient qualifier for the surgery. Secondly it is not a surgery for functional range of motion improvement. No such improvement will occur nor is there any surgery that can have that effect. Thirdly, this is an operation done in the prone position under general anesthesia. Fourth one may return unrestricted sports activities 4 to 6 weeks after the surgery. Lastly the risks of the surgery are aesthetic…how much improvement is seen and how well does the scar heal on the back of the neck.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,So I have a drawing here of pretty much what I want for my custom testicle implants. I also included a picture of what I look like on a normal day as well as me stretching my sack with a saline infusion to show that I think I can handle a larger size implant. My goal is to have permanent low hangers that hide my real testicles, but I still want everything to look realistic. just a tad larger than most guys. I have been doing saline infusions for a few years now and I think I decently stretched my skin to make extra room in there.
A:Thanks for the information. The question is certainly not whether your scrotum can handle just about any size implant but what the implant’s size and shape should be. The conundrum is having implants that hang long enough but in so doing also hide your natural testicles. This is where the stretchy scrotum works against what you are trying to achieve based on your drawing. If the implants had that size and hung that low your natural testicles would certainly be exposed. The ‘problem’ with a lot of scrotal laxity is that it would take an enormous sized implants to fill it out without exposing your natural testicles but then they wouldn’t hang like you have drawn. So I don’t think you can achieve exactly what you want based on this drawing.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a very important question for you. I have a flat forehead, but slightly sloped, and my brow ridges are underdeveloped, can you augment my brow ridges, and with implants, make my forehead more sloped? Is this possible? On the first photo, the person has a sloping forehead and well-developed brow ridges, while on the second photo, it’s the opposite.
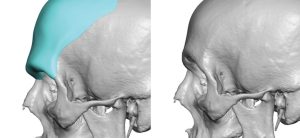 A:You are referring to the use of a custom forehead-brow bone implant surgery for that aesthetic effect, a procedure that I do regularly.
A:You are referring to the use of a custom forehead-brow bone implant surgery for that aesthetic effect, a procedure that I do regularly.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a question regarding your testicular enhancement methods with solid implants to see whether it makes sense to schedule a virtual appointment.
My testicles are not small but rather regular (almost 5cm in length) and I would have normally opted for the wraaparound technique to have them enhanced. From one of your recent articles I understand that the wraparound technique not used anymore so the side by side displacement method is the safe alternative nowadays.
And here’s my question: if the custom implant needs to be at least 75% bigger than the natural testicle and if the largest implants so far have been 8.5cm long is this a good technique to enhance ‘standard-size’ testicles where the implants would need to be longer than 8.5cm?
I know that the scrotum can be stretched easily and mine is relatively wide already but what is the limiting factor for these custom implants: is there any technical or medical reason why they can’t be 9cm or 10cm in length?
A: It is not that I would never do a wrap around testicle implant again, and it is a great concept, just that one has to accept the 50% risk that one of them will eventually become dislodged.
At a near 5 cm size you are correct in that volumetric displacement would likely have to be in the 7 to 7.5cm range. Technically it is implant volume not length that matters most when it comes to a displacement effect. (e.g., a 5cm testicle implant = 45cc, a 6.5cm implant = 70cc and an 8.0cm implant = 130cc) As you can see using the length measurement alone is deceiving about the effects of implant displacement on the natural testicles. Then it comes down to whether implants of that size will fit which can be deceiving as there are two of them. But at 7.0cm (80ccs) and 7.5cm (105ccs) probably they would as long as one as some scrotal skin laxity.
I thin now you can also see why implants of 9 or 10cms in size would never be needed nor would they ever fit.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Here are the attached before, after, and hip implant outline pictures. To reiterate, I feel the hip implants designed help address the goals mentioned but might fall short of making this desired silhouette change. To outline the goals in order of importance to least important:
1) To look as natural as possible if not seamlessly natural with the rest of the body.
2) To feminize the hip and side-butt area.
3) To augment the hip (and body) silhouette to get as close to or emulate that supplied after changes picture.
4) To fill in the congenital dip that is currently present on the side-butt hip area to look more if not seamless with the rest of that area in terms of volume.
I also wanted to know what, to the best of their knowledge, would be the trade-off between the scars produced for the current planned implant vs anything larger.
A:Your hip augmentation goals and objectives are not in question. What is in question and is the fundamental dilemma that you face is the following:
To review the fundamental issue with hip implants and their high and predictable postoperative problems that they cause, it comes down to this general premise:
Accept a smaller implant size/coverage with a reduced risk of problems…or go for a bigger coverage area and accept the assured equalae that comes with it.
The key question of course is what is the adverse sequelae that will happen with larger surface area hip implants…the bottom third will bend and the inferior edge of the implant will show,. That will occur with a 100% predictability based on the coverage area you have outlined. The question thus is not whether it will happen but how significant will that effect be.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello i want to ask i have 25yo and i see on my skull asymetry. one side is more flat than other side soo if its possible to make more symetrie skull thx!:)
A: All skull asymmetries can be improved using a 3D CT scan to accurately identify the flat asymmetric area from which a custom skull implant is designed to treat it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I was wondering if I could get a consultation from you re a recent sliding genioplasty I just had. I did a google search after the surgery and saw your comments about lip droop. I measured my facial dimensions and it appears my chin was shortened by about 10 mm after surgery and my upper lip about 2 mm. I drool most of the time and can’t say certain consonants like B, F and P. It’s only been three weeks, but your comments have me concerned that this won’t be self-correcting. I was curious if there was any chance of correcting the lower lip with a second surgery.
Thanks for your time
A: I normally don’t comment on patient’s concerns/problems when they are in the early recovery period and are under the active care of the surgeon who performed it. But what I would say in your cases you need ask your surgeon about this early outcome as a lower lip that significantly droops down after chin surgery has a high chance to be a persistent problem.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Are the titanium hip implants hard when someone touches you? Can I see some before & after pictures please?
A: They are metal so they are hard to the touch, just like your natural iliac crest bone. We are just starting implantation of these implants here in the U.S. so we don’t have any results yet to show. To see results go to the Korean site where they were developed and have been implanting them for several years.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Would hydroxypatite implants be an option for skull implants?
A: Unless it is a very small area that is located on the bony skull (not the sides) in which a long scalp scar can be used to access it….no. While hydroxyapatite is biologically appealing it is a poor aesthetic augmentation material whether it is the face or the skull. It simply doesn’t have the proper handling and shape characteristics to effectively use.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, hello I have ptosis of the chin. A surgeon put sutures for an elevation of the vestibule, no anchorage, and it did not work.I know that now you make facial implants but how to fix this please? what technique? help me
A: Ptosis of the chin can be very difficult to significantly improve. Vestibular shortening is an adjunctive procedure in the treatment of chin ptosis not a primary one so it alone would not be expected to work. A small implant that allows for tissue ingriowth, anchorage and vestibular shortening is a more comprehensive approach.
An important question is what is the cause of your chin ptosis?
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Could he also do a midface lift from inside the mouth incision to combat any sagging from removal.
A: A midface lift requires a superior point of pull, thus an inferior intraoral approach will not work. But I would doubt that would ever be necessary from nasal base implant removals.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, is there a way to make rib removal results more extreme? like removing more ribs?
A: The reason I present the imaging in the way it is shown is because you make a decision for surgery based on the LEAST amount of change that is known to occur NOT on the most amount of change you hope will happen. The former is known to occur while the latter may never happen. It is all about controlling expectations as that is how you don’t end up disappointed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Does The Orientation of the Dermal-Fat Graft Affect How Well It Works In Buccal Lipectomy Reversals?
Q: Dr. Eppley, In your case study titled “Plastic Surgery Case Study – Buccal Lipectomy Reversal with Dermal-Fat Grafts” you write “With the suture placement through the graft the dermis surface of the graft into the pocket on the opposite side of the incisional closure.” I have 2 questions about the Dermal Fat Grafts (DFG) orientation inside the buccal space, as it is described in the above excerpt:
1. Does the Dermis side of the DFG face the cheek/away from the mouth, or does the Dermis side face the tongue/towards the mouth?
2. Does the orientation effect the viability of the graft?
A: In answer to your dermal-fat graft questions:
1) The dermis side faces the incision or the tongue side.
2) In the deep buccal fat pad space the orientation of the graft does not affect its external visibility.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
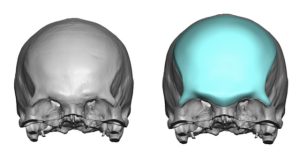
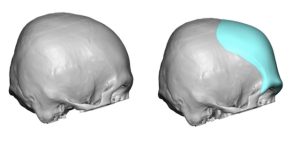
Q: Dr. Eppley, I have a problem with flat back head and have few question about skull reshaping surgery.
How long does recovery take after surgery?
Can I travel by plain after surgery?
Do the implants need to be replaced or do they last for life?
A:In answer to your flat back of head questions:
1) Custom skull implants are made to treat it (see attached) and such implants are permanent and never need to be replaced due to structural failure.
2) Recovery is largely defined as swelling and sometimes bruising of which the most significant of these effects are largely resolved in 10 to 14 days after the surgery.
3) Patients can return home 2 to 3 days after the surgery including by air travel.
Dr. Barry Eppley
World-Renowned Plastic Surgeon