Your Questions
Your Questions
Q: Dr. Eppley, I am scheduled this summer for a procedure for the removal of an occipital knob on the back side of my skull. Before fully committing to the procedure, I wanted to ask a few questions pertaining to concerns that I have about the operation.
From our consultation and the case studies that you published online, I understand that this is a fairly low-risk procedure. Are there any potential serious implications that could arise from this surgery? I am also concerned about the size of the scar for this operation. I plan on fully shaving my head after the surgery; in your estimation, will the scar be detectable from a few feet away? I understand that the scar size can be variable, but will it appear to be a hairline incision and will it be any wider than two inches? I attached photos of the occipital knob to this message if they may be helpful in gauging the potential size of the scar.
Any information would be greatly appreciated, thank you.
A: In answer to your occipital knob skull reduction questions:
1) The occipital knob is a very thick protrusion of bone which means reducing it entirely still leaves a lot of bone for protection. While I could not imagine it not being very thick bone, the way to absolutely determine if it is indeed as thick as I think it is is to get a 2D CT scan and make measurements.
2) The scalp scar is in the range of 5 cms length and it does heal very well. It is placed in a horizontal skin crease if one exists which in your case would be at the bottom of the knob. I can not say whether it will heal so well that it would be undetectable from a few feet away. But I have yet to have a male patient comment on that they found the scar unacceptable.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, I have been looking to have chin surgery for a while now. My chin is my biggest insecurity. I never smile due to the way my chin pulls down when I smile. I also dislike the dimple in my chin and how wide my chin looks when I smile.
A: Thank you for your inquiry, sending your pictures and detailing your concerns. You have two specific soft tissue chin concerns, 1) hyperdynamic chin ptosis and 2) a vertical chin cleft. They may be anatomically related as a vertical chin cleft occurs due to a midline soft tissue deficiency. For improvement/correction a submental approaches needed as the size of the chin pad must b reduced and the chin cleft managed by a muscle repair in your case. Such soft tissue chin repairs, while not technically challenging to perform, are difficult to predict the outcomes since surgery is done in a static setting while your chin issues mainly appear with dynamic motion. (smiling)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a big complex with my head shape because my head is too wide. When I go a Korean plastic surgery hospital the doctor said most part of side head is bone, there is very slim muscle over the ear. Is that true that there is 7mm to 9mms tmuscle hickness above the ear??
A: In my extensive experience with temporal reduction surgery, most men particularly Asian males, have very thick temporalis muscle in the location above the ears. It is usually in the 7 to 9mm thickness range and sometimes even thicker. However the best way to determine the muscle:bone composition ratio of the side of the head is a CT scan. By looking at how much the thickness of the muscle makes up the sides of the head this will help you to determine if temporal reduction surgery is worth it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Would this mess on the side of my mouth be correctable without a facelift? Just an incision beside mouth? I had filler placed there over a year ago and ever since it looks terrible. I have also had the area melted with devices and I am left like this. I’d take a scar any day over this mess. Thank you.
A: Thank you for your inquiry and sending your picture. With the development of perioral folds I would expect any treatment that involved adding volume (fillers) or skin tightening/fat reduction efforts to merely exaggerate the problem. This is a surgical issue that requires either direct or indirect tissue excision/rearrangement. Even though it is an indirect approach, there is no doubt that a lower facelift is the superior approach to trying to smooth out this area by distant tissue excision and skin pull and is also scar free by the mouth area. However there is a direct approach which is an elliptical tissue excision placed above the perioral folds along the line of the nasolabial fold. (see attached image) It typically is reserved for much older patients who have a very deep nasolabial fold anyway which is the equivalent of a pre-existing scar. Bit it can be done on anyone if they are motivated enough to want to avoid a facelift and can accept the scars.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Greetings, do you by any chance offer cranioynostosis treatment in adults, 19 years old to be specific. I have lived with sagittal craniosynostosis my whole life and I want to get it treated.Please refer me to someone that can perform this procedure if it is not in your field.
A: Almost 100% of the time cranial vault surgery is not done in adults due to the increased thickness of the bone and the magnitude of the surgery. Young children have thin pliable bone and a growing brain to help shape it. In adults we greet the effects of sagittal synostosis used on the aesthetics of it not through craniotomies.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I need this procedure. Can a custom skull implant be made that creates a square shape without increasing the height of the head?
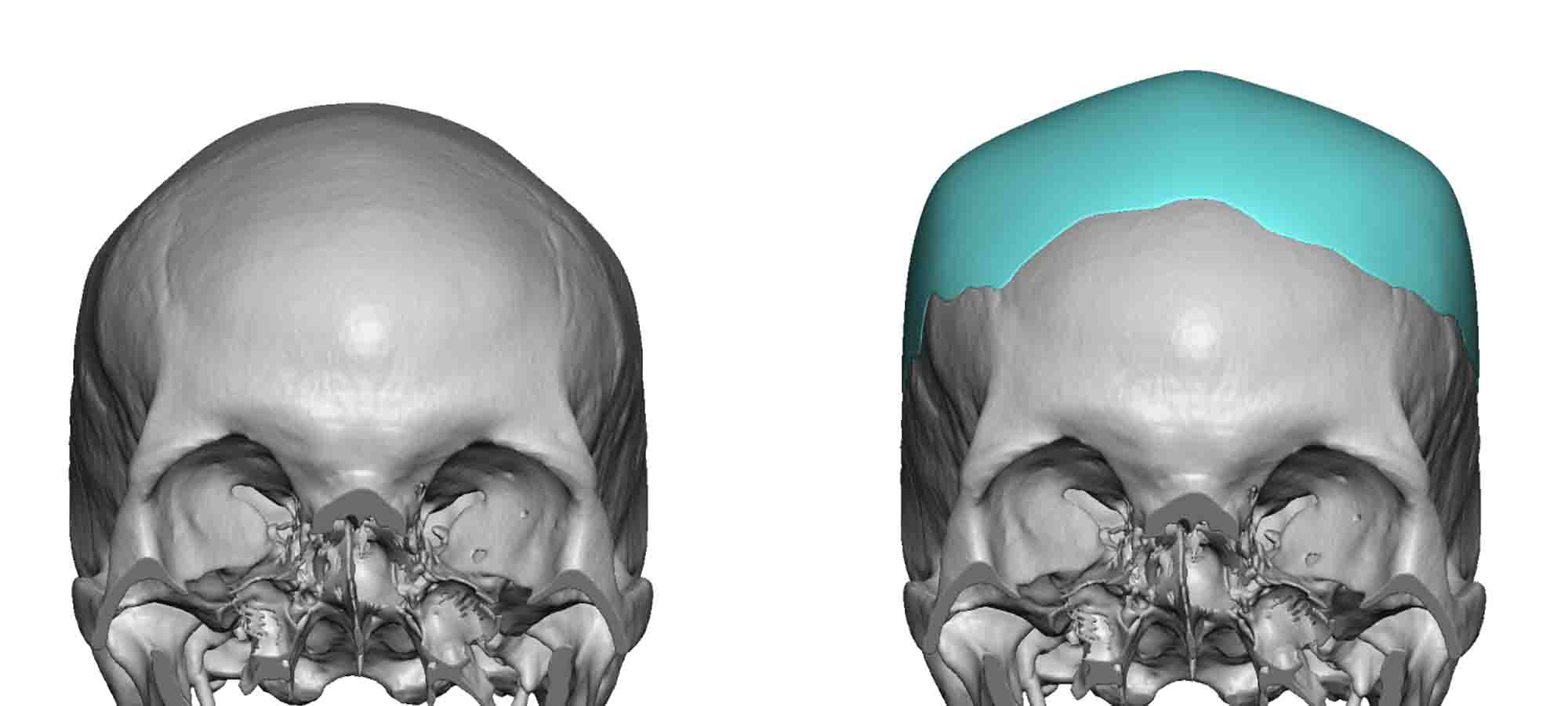 A: Creating a more square-shaped head requires a custom skull implant that elevated the lateral bony temporal line. While such an implant will cross the sagittal midline of the head it would do so by only adding about 2 to 3mms of height in the middle…which I would call not really substantially increasing the height of the head.
A: Creating a more square-shaped head requires a custom skull implant that elevated the lateral bony temporal line. While such an implant will cross the sagittal midline of the head it would do so by only adding about 2 to 3mms of height in the middle…which I would call not really substantially increasing the height of the head.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Please find attached photos of my face at anterior, oblique and profile angles.
I’m interested in custom paranasal silicone implants to address retrusion in the Lefort 2 area and general lack of definition in my midface. I’m hoping to achieve 5-6mm with paranasal implants.
I’ll be looking into dental veneers down the road to project the teeth out as much as possible as well.
I’m aware that down the road I’ll need implants to address retrusion in the tear trough area too, and other work, but would like to start with the paranasals for now.
I’ve also attached photos of my “ideal” female faces where the mid and lower face areas are very well projected (even though I am aware my lower face is structured very differently to theirs.)
Could you please advise on what the cost of custom paranasal implants, including all surgical costs, would be?
Many thanks.
A: Thank you for your inquiry and sending all of your pictures. The best way to think about your implant design is to look at a typical Asian midface implant that addresses the whole midface retrusion issue and then decide how to reduce it if so desired. I have outlined with the purple lines what would be considered the footprint off the premaxillary-paranasal component of it. Assuming that is the basic design of what you need/desire, my assistant Camille will pass along the cost of the surgery to you later today.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in Vertical Orbital Dystopia surgery obj my right eye. However, there is concern involved, as I have to put in eye drops. Here are the names of the drops:
Vital Tears Eye Drops
AzaSite Eye Drops
Xiidra Eye Drops
Retaine Eye Drops.
These are all for dry eye purposes.
A:Those eye drops are all used to treat dry eye syndrome (keratoconjunctivitis sicca) which I assume this is present in both eyes and not just the vertical orbital dystopia side. But even so that does present some concerns about aggravating that condition with any type of procedure on the eyelids in which their position up against the eyeball is surgically manipulated. I would have to have some input from your ophthalmologist who put you on these medications to better determine the risk of symptomatic aggravation with any orbital surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, One thing that bothers me is the fact that I don’t have hollow cheeks like a lot of models do. Why is this, and how could I get that as well as just get a more angular facial structure overall? I have heard that thick skin tissue plays a part, not sure if that is the case for me?
Best regards.
A: Thank you for sending your pictures. While thicker skin does play a major role in how well the facial bones are seen, you still have some room for improvement in changing some of your facial structure. The two areas that strike me as the most important for you are buccal lipectomies (for hollow cheeks) and jaw angle augmentation. (for more angular facial structure) n This would enhance the already largely good facial bone structure you already have.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I asked you the other day if the chin can, in a safe and natural manner, be vertically lengthened up to 15-20mm and you answered as follows:
“Getting the chin vertically increased to 15 to 20mms is best done by a staged vertical lengthening bony genioplasty. In the first stage the bone is lengthen by 10mms and then six months later add the additional vertical length required. No form of an implant does this very well became the soft tissue chin pad will not redrape up over the implant properly once it is detached for implant placement. It works in a genioplasty because the soft tissue chin pad at the bottom is never detached thus always follows the bone vertically down in a natural fashion.”
With regards to this I just had a follow-up question:
Is it possible to split the two stages into a genioplasty and then a custom chin implant? So for example in the first stage the chin will be vertically lengthened via a genioplasty, say, 10mm. And then in the second stage (4-6 months later) the chin will be further vertically lengthened via a custom chin implant, say, 5-6mm. Might that work?
A:Your supposition is correct. That would be an effective technique as long as the bulk of the ertucaly lengthenign effect is done by the bony genioplasty. (10 to 12mm bine first stage, 5mm implant second stage)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question regarding custom forehead implants. I’m a saturation diver which basically means we live in hyperbaric chambers for a month at a time at depths at up to -300metres. We breath helium so we saturate our bodies in helium/oxygen. Would these implants be ok absorbing helium and decompressing as such. Would there be any complications? Obviously if the implants holds any gas on the way up to the surface there’s going to be huge complications. Have you ever had experience with saturation divers and implants in the past. Just want to make sure it is indeed safe.
A: Good question… that is a new one although not the first diver who has had a skull/forehead implant in my practice. Solid silicone is a highly-cross linked polymer which would not absorb any gases that are circulating in your blood stream. That is not possible from a material and soluble gases standpoint.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question regarding paranasal implants. Could they be used in a way to bring the alar base upwards? The reason I’m asking is because this would enable a long nose to appear shorten, since if there was a way to bring the alar base forward and up (through means of a well placed implant), one could then shave the collumela and present with a shortened nose (the entire base of the nose would move up, including the alar base).
Thank you in advance!
A:Thank you for your inquiry. No form of midface augmentation is going to rotate the alar base upwards in any significant way. The effects of paranasal implants are primarily in the horizontal or forward direction…at least by conventional design. I could envision shaping the patronal implant design a certain way to try and create that upward movement but I could not tell you whether that would be effective for that type of nasal base change.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in learning more about a surgical knee lift. I have very bad rolls of wrinkles from suntanning in my youth. I may need a calf lift too. I have sagging there also. I would love to see some pictures of any knee lift procedures. Thank you
A: Thank you for our inquiry and sending your pictures. A knee lift is similar to a few other body contouring procedures (e.g. armlift) in that a visible scar results that is not hidden. (unlike breast lift or tummy tuck for example) Thus the decision for such surgeries is more aesthetically difficult because one doesn’t have the luxury of a surgical result that does not have its own aesthetic downside. Thus, It is always a question of which is better from the patient’s perspective…the scar from a knee lift or the wrinkles above the knee. each patient is going to interpret that differently. The only thing that matters is to avoid trading off one problem for another problem that one dislikes just as much. With this premise in mind the patient who feels the knee lift scar better than their wrinkles is a good candidate for the procedure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m interested in undereye-cheek implants. I prefer custom implants to be able to individualize the shape of the implants to suit my face, but on the other hand I’m worried that the costs will be much higher. Please inform me on the cost difference between custom and conventional implants and maybe on some other (dis-)advantages of either procedure.
A: Your assumption is correct in that custom undereye cheek implants is always going to cost more than the use of standard implants. But beyond cost the reason a patient would choose a custom implant approach in almost all cases is because they offer implant designs and augmentation results that are not available with the use of standard facial implant designs. Such is the case with infraorbital-malar implants (aka custom undereye cheek implants0 as no such standard implant design exists to replicate what this custom approach to the undereye area does. One could try and combine standard infraorbital and cheek implants but they would be a relatively poor substitute as they are not only not connected but don’t create the same effect.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a few questions concerning the eyelids. When I met with you concerning my hooded lids he asked how I felt regarding my brows. At the time, I said that I was good with my brows. I have since given it some more thought and wonder if a brow lift in conjunction with an eyelid lift might be the best option to address my concerns regarding my heavy lids.
– Is it possible to do a brow lift in conjunction with the eyelid lift?
– What types of brow lifts do you recommend? Essentially, where are the incisions?
A: In answer to your browlift questions:
1) A browlift and upper blepharoplasties are commonly done together and is a more complete form of eye rejuvenation if there is ay brow sagging present.
2) For determining the type of browlift, for which there are five (5) different types, the key determinant is the length of the forehead. (how long is the distance between the eyebrows and the hairline. If the forehead is not long, an endoscopic browlift technique is done. If the patient has a long forehead of which there is concern about it getting any longer, a pretrichial or hairline type of browlift is done.
Dr. Barry Eppley
Indianapolis, Indiana
Q:Dr. Eppley, I had saline breast implants placed five years ago through armpit incisions. The left breast implant has always been too high but I let it go at that time. I now want to change my implants to silicone, increase my breast size and get the two breasts looking more similar. (attached are my current pictures) Do you think I would need to come in in person to discuss the breast operation and be examined? I know there are different types and shapes of silicone implants and so I want to ensure that we choose the correct implant. I prefer them to sit a little lower because I think it looks more natural. Basically I’d be happy if both my implants looked like my “good” implant, the one that was placed correctly. Also, I don’t think adding 75 CCs is a huge jump but if this greatly increases my chances of rippling or other issues, I’d like to weigh that in my decision. I’m really happy with the look and feel of my breasts, they feel natural and there is no rippling double bubble etc. So I am trying to avoid any of those issues in round two and honestly that’s kind of been my hesitation in getting them fixed, but the asymmetry does really bother me.
A: In answer to your breast implant replacement questions:
1) I do not consider a before consultation (coming in way ahead of surgery) to be essential. There will be one the day before surgery anyway. Your pictures show a left breast with a highly positioned implant with the associated higher inframammary fold level as well. This is not rare in the transaxillary approach for breast implants, particularly on the non-dominant side of the surgeon. (right handed surgeon often does not do an adequate inferior dissection on the left side of the patient) This is best treated by a small inframammary incision where the lower end of the pocket can be adequately released with the implant exchange. The implant size increase is already known (+75ccs) and there are only available smooth silicone implants today of which high profile projection is probably what you are seeking. (all textured/shaped implants have been removed from clinical use or should not be used due to the risk/concerns of ALCL) Your goal, besides volumetric breast size increase, is to have the left implant position look like the right…that is a given.
2) A 75cc implant increase is really minimal so don’t let the number fool you. As a general rule one needs at least a 30% implant volume increase to even see any change on the outside. For example, if one has 350cc one really need at least 450ccs (+100ccs) to tell any difference at all.
3) The size of a breast implant has no correlation with the occurrence of ripping. That is caused by different issues.
4) When in doubt about the increasing the size of the breast implants, you can always just adjust the left implant down as that addresses the most important concern to you
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is it possible to do a combination of sliding genioplasty for vertical and horizontal chin increases while also doing jaw implants to maintain the optimal jawline proportions and angles? Can both procedures be done in the same surgery?
Is a wrap around vertically lengthening implant the better alternative or is this a case by case assessment?
 A: Thank you for your inquiry. It is very common in my practice to combine a sliding genioplasty for the chin and a custom jawline implants for the rest of the jawline.
A: Thank you for your inquiry. It is very common in my practice to combine a sliding genioplasty for the chin and a custom jawline implants for the rest of the jawline.
Whether a total custom jawline implant would be better or even a good alternative depends on the horizontal and vertical dimensional changes needed for the chin augmentation part of the jaw. If the additive numbers of the horizontal and vertical chin movement is 12 or less a custom jawline implant can be done. But if those combined numbers are greater than 12, a sliding genioplasty is needed for the chin augmentation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question regarding the forehead implant and size…How large do these implants go? Can they be made quite substantial or is there there a limit to the depth and size etc…My forehead is quite sloping you see and small….So I’d like to go substantially larger if possible. Nothing ridiculous but as long as it looks adequate. Not happy with it right now at all.
 A: Technically a custom forehead implant can be made to any size in the design process.The ‘limitation’ is in how much the forehead skin can stretch to accommodate what is placed behind it. While that is a practical consideration, the reality is that I have not yet seen someone whose tissues could not stretch to accommodate any implant that has been designed.
A: Technically a custom forehead implant can be made to any size in the design process.The ‘limitation’ is in how much the forehead skin can stretch to accommodate what is placed behind it. While that is a practical consideration, the reality is that I have not yet seen someone whose tissues could not stretch to accommodate any implant that has been designed.
One of the keys in custom forehead implant designing is the balance between how much the slope should be corrected in the side profile vs how much width to provide in the front view to keep it looking natural and that it look like it belongs there. The latter is trickier to figure out then how much to change the slope.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am 24 years old and I had regrettable cheekbone reduction surgery in Korea sic months ago and I am devastated by the results. I am hoping to reverse the changes made and was wondering if you could help with some questions.
I think the doctor fractured the zygomatic bone then pushed and rotated it inwards. If no bone was removed, is it possible to push and rotate it back outwards? Is a bone graft still necessary in this case?
Many thanks for your help.
A: I am very sorry to hear of your unsatisfactory aesthetic results. Cheekbone reduction osteotomies can be reversed and, in most cases, a bone graft is required. That determination however requires a 3D CT scan to look at the osteotomy pattern and the current healing of the zygomatic osteotomy site. That is a scan you can get where you live and we can order it for you to have it done.
Dr. Barry Eppley
Indianapolis, Indiana
Dr. Eppley, I have a question about the shoulder reduction treatment, I am wondering what the costs of this treatment would be?
I am emailing as I wish to reduce my shoulder width length. My shoulder width length is very problematic to me as I am a woman but my shoulders are so wide it gives me a very manly figure (see image). I have discovered about this surgery from an online forum from a patient who underwent treatment with Dr Eppley. I am curious as to how much the total procedure would cost, the recovery time and bone healing time.
Kind regards,
A: Thank you for our inquiry and sending your pictures. Your bideltoid width appears to be greater than 50cms which would more masculine than feminine. Thus you would be a good candidate for shoulder reduction surgery. I will have my assistant Camille pass along the cost of the surgery to you later today. The total recovery time is six weeks which mainly relates to how long full range of motion of both shoulders is normalized. It is a progressive range of motion of the shoulders which begins at two weeks after surgery.
Dr Barry Eppley
Indianapolis, Indiana
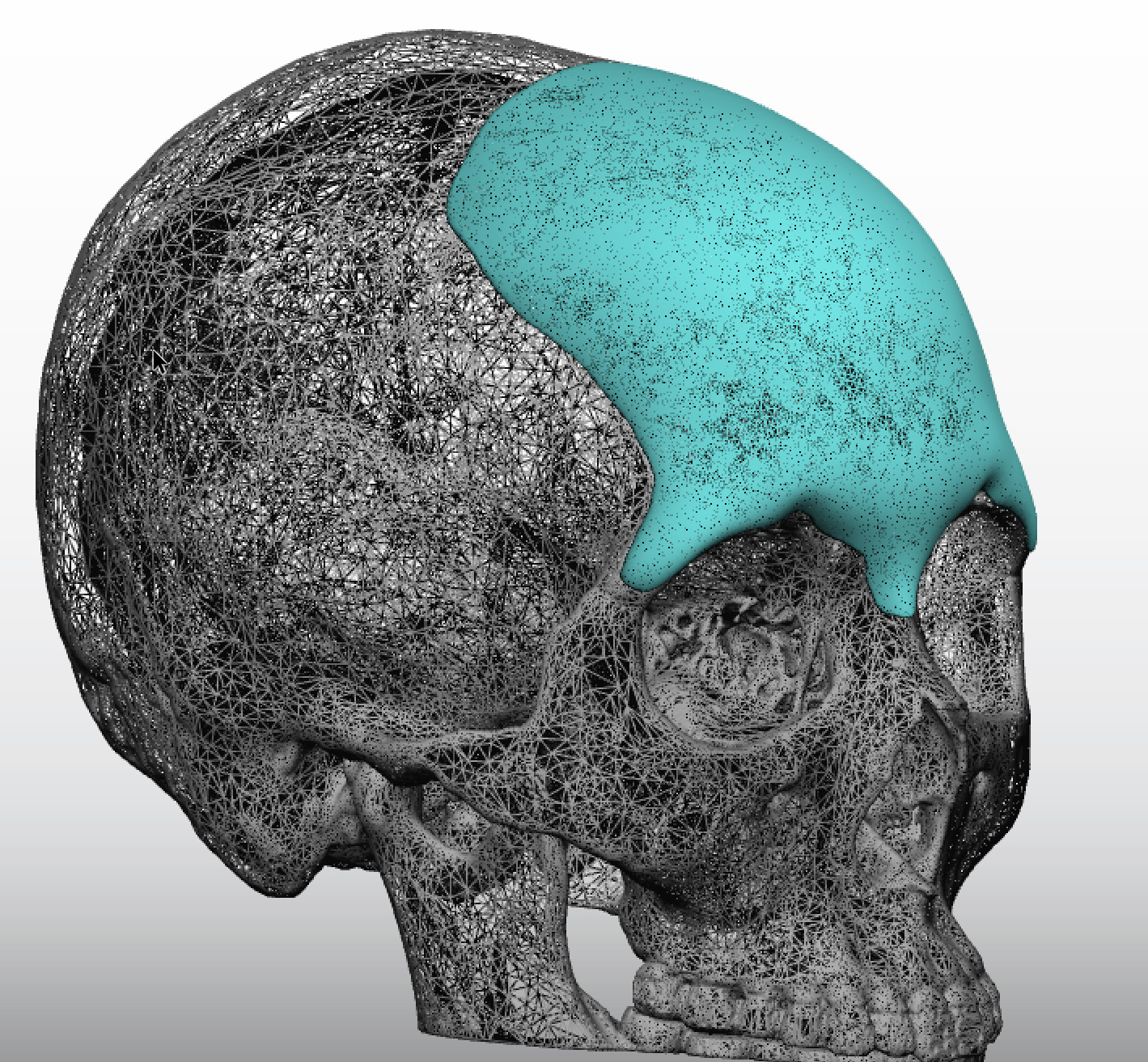
Q: Dr. Eppley, I need a custom skull implant procedure. Can such an implant be made that creates a square shape without increasing the height of the head?
A: Creating a more square-shaped head requires a custom skull implant that elevates the lateral bony temporal line. While such an implant will cross the sagittal midline of the head it would do so by only adding about 2 to 3mms of height in the middle…which I would call not really substantially increasing the height of the head.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am female to male trans man. I have an extremely small head and very self conscious. I saw a doctor about jaw and chin implants to give the illusion of a larger head but he said it would unbalance my face because my head is so small. Do you think you could help me with this with a custom skull implant?
A:Given that males on average have a 10% bigger head size as measured by a circumferential measurement than females (although shape is also important) an overall head size increase can be obtained by a custom skull implant. What the exact dimensional increases should be is up for discussion but I did some imaging on one of your pictures to see what that might look like which is attached. This probably represents a 10% head enlargement effect.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have been researching a lot about chin reduction but it seems like my case is not common at all. I used to got filler injected to my chin but two years later I found out the substance I got injected may not hyaluronic acid-based which is dissolvable. It made my chin longer, more protrusive horizontally, and kinda pointy. I really wanted to come back where i was before, at least reduct the length and make it less protrude. My case is that my bone is totally fine, it is all about the soft tissue. I know its difficult to handle the soft tissue thats why Im reaching out to you whom I believe is very experienced in this area. Please let me know if I am too ambitious.
A:Thank you for your inquiry and sending your pictures. The question in your case is whether a submental chin pad excision would produce the desired chin change and whether the fine line scar to do so is worth it. Your chin pad excess is caused by injections which likely means the cause of the problem is undoubtably spread throughout the tissues which has created an overall fullness. The injection material is not located in just one spot. But yet the only excisional approach is to remove a wedge of chin pad tissue from below in an effort to make the chin smaller. (submental tuck) This can be effective as long as one can accept a fine line scar under the chin to do so.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a problem and the back of the head is flat and I want it to be adjusted and from the back should be circularly acceptable
Is it possible to get good results?
Is the process safe and does not need hair remove?
Is the material that will be placed against the back of the head fixed and does not move with the years.
A: In answer to your occipital augmentation questions;
1) Most cases of occipital augmentation get good results based on how much the scalp can stretch to accommodate the implant.
2) No hair removal is needed to do the surgery.
3) The implant is fixed to the bone and will never move.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, is asking if Rib Removal and Breast Augmentation may be done in the same surgery?
A: Rib removal and breast augmentation can be done at the same time and their diametric effects are synergestic for body contouring changes. It is not too much surgery to go through at one time and is commonly done. Neither procedure causes an undue amount of pain nor does one recovery prolong the recovery of the other procedure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, There’s an issue that I’ve been wondering as to whether a surgical intervention exists. I have extremely deep-set eyes with a lot of spacing between my eye and the brow bone above. This creates a sort of gaunt look (and only gets more exaggerated with age, as I’ve been able to see in both of my parents) with no hooding whatsoever and I don’t care for it. A picture is attached that gives an idea of what I’m referencing. I’ve always preferred the more hooded, bedroom eye-type look (which I guess has come to be referred to as “hunter eyes”) and I’m wondering if there is any way to create that look. (Lateral brow bone implant?) I tried some filler in that area to try and create that look, but it looked sort of clumpy and didn’t provide much change.
I’ve attached a picture of me that shows the issue, as well as an example of the target I have in mind.
I’d love your input, and hope you’re well. Thanks very much!
A: The anatomic differences between you and your ideal upper eye look is the lack of adequate brow bone projection and upper eyelid soft tissue fullness. You have a long distance between your brow and lashline and a deep supratarsal sulcus. While I don’t think you can ever get exactly that look, it would require a combination of brow bone augmentation and fat grafting to the upper eyelids to come close. That would have to be a staged procedure with the brow bone augmentation done first followed by fat grafting later.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have had multiple bony genioplasties and I have another one planned later this year. Now I’m having a functional issue where it’s a bit hard to talk, it takes more effort then usual. I think this is because I still have skin that is not fully supported by the chin bone. I’m wondering, do you know if there’s any simple procedure that can be done now to reduce the severity of this functional issue until I can move forward with having the genioplasty advancement? Or do you think a temporary implant would resolve this issue? I really want to minimize creating any scar tissue but if you have any thoughts please let me know. It almost seems like if there was a screw that can be inserted underneath to hold the skin in place that, that would resolve the issue. Let me know your thoughts.
A: What you are referring to is mentalis or soft tissue chin pad suspension in which the soft tissues are sutured up to a higher position through an intraoral approach. The superior portions of your existing titanium hardware may be sufficient to do so. Whether that will really provide an improvement to your symptoms I can not say but that is how it would be technically done. I have done such soft tissue suspensions from underneath the chin so I can not say how effective that might be.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Could you please give me advice on enhancing my hip dips? Please see attached for photos. I am 5” 1” tall and weigh 126 lbs. M prior surgery has been a BBL procedure with liposuction.
Please let me know if there are any questions or concerns.
A: Thank you for your inquiry and sending your picture. With a thin body frame and have had prior BBL surgery, I am going to assume that you have had a prior effort at fat grating into the hip dips. While fat grafting for hip augmentation is not associated with as high a fat take as that of the buttocks, it is always the first approach that should be done. If one can get some fat to take into the hips, even if it takes more than one grafting session, this is always the preferred approach because it is of an autologous nature.
When fat grafting has failed or there are inadequate fat reservoirs for harvest, the remaining approach is that of an implant. Custom designed hip implants can be used for placement on top of the TFL fascia over the trochanteric area. (hip dips)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a pro bodybuilder but have always had a hard time building a great chest due to my height and width delisted attaining that status. While I have put on some mass, it is just not as impressive as my other areas of muscle density. I am thinking about pectoral implants. Can you install them to look just as natural as someone without but with just a great dense chest that won’t be visible when I compete? I plan to compete for several more years. Your thoughts?
A: Thank you for your inquiry and detailing your objective and concerns. Since pectoral implants are placed in a submuscular position and are placed so that the implant does NOT extend past or violate the lateral pectoral muscle border (which is a key distinction from that of breast implants in women), there is no risk of animation deformity which is common in breast implants. I would imagine that what you mean by a ‘dense chest’ look is a thicker muscle mass in the medial 2/3s of the muscle belly with good definition air the sternal and upper pole (under the clavicle) areas. The key to such a pectoral implant design is to keep the base diameter or footprint of the implant all within the muscle border but have good/high projection in the desired areas. This would be a unique look/goal from the non-body builder male and would most likely require its own unique design.
Dr. Barry Eppley
Indianapolis, Indiana
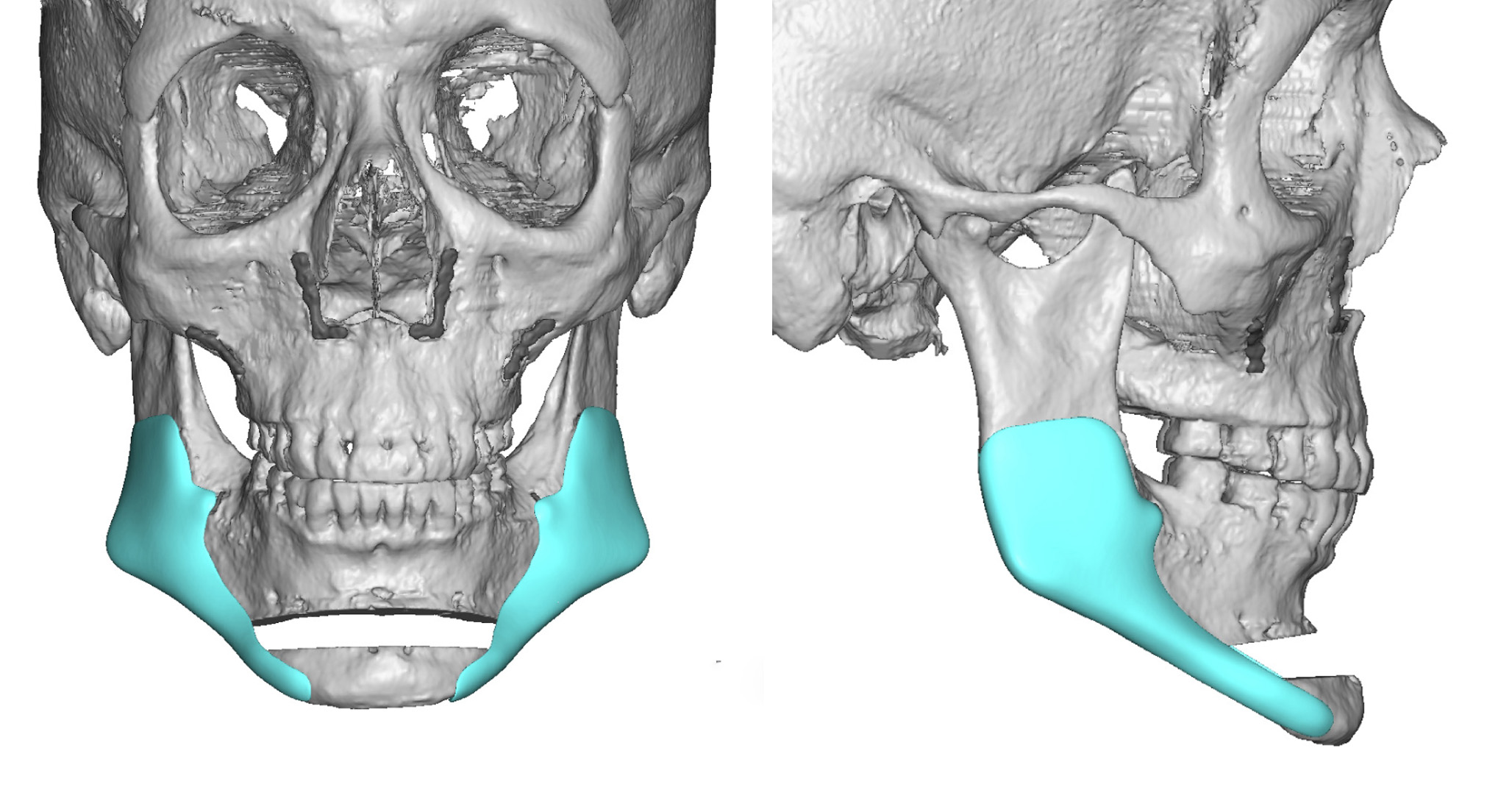
Q: Dr. Eppley, My photos are attached and the #1’s are with my jaw relaxed as normal. The #2’s are with my jaw pushed forward and is the look that I am after. I’m seeking a vertically longer, wider and more pronounced lower face in all aspects especially the area between my lower lip and the tip of my chin bone. My profile’s features are naturally pointy and I want them square. Thanks for your help.
A: Thank you for sending your pictures and doing your own imaging for your desired jawline augmentation goals. What you are demonstrating is a vertical lengthening jawline augmentation with a squaring effect at the three corners. (chin and jaw angles) This can be done one of two ways depending on how much vertical chin lengthening is desired. If the vertical chin lengthening needed is less than 10mms than the entire jawline can be lengthened by a custom implant design. If the vertical chin lengthening is 10mms or greater then a combined vertical lengthening bony genioplasty combined with a custom implant that brings down the rest of the jawline as well as squares out the chin.
The reason there is a dual approach is the the soft tissue chin pad will only stretch vertically so far if separated from its attachment to the bone. (total vertical lengthening jawline implant) You have to be careful that you don’t put in such an implant and then ‘discover’ that the chin pad will not lengthen enough to pull over the end of the implant properly. A lengthening bony genioplasty gets around that problem as the soft tissue chin pad will go wherever the bone goes because it remains attached to it.
Dr. Barry Eppley
Indianapolis, Indiana