Your Questions
Your Questions
Q: Dr. Eppley, I have two inquiries, the first wanting to know which option testicle implants of side by side and wrap around allows for the largest sizes? I was also wondering if surgical steel or something could be included to make them weight more?
A: Both testicle enhancement techniques allow for the same increases in size but the wrap around technique has a much higher complication rate with not infrequent implant separation.
Metal can be incorporated into a central hollow chamber in the implant but it is important to recognize that this is an off-label implant technique.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My question is relate to a 5mm genioplasty reduction i had done 25 years ago. As a result I’ve lost some contour as far as the muscle below the lip fold. I’ve read that tissue can be tied up to create the natural curve. In a second procedure A small chin implant was placed to restore the fold but I’m still a bit flat. The area looks great when I add filler to that muscle but I’d love to not have to continue to do that. Is it possible to ‘tie up the tissue’ so that I’m not quite so flat from front and side and as a result the chin would be a bit shorter? Thank you!
A: I would not confuse the aesthetic effects of filler with soft tissue resuspension. That is not the effect tissue suspension would create and, even of it could, it would not be a sustained effect. Such tissue resuspensions frequently fail after a few months.(fall back down) The potentially more effective approach is submental chin tuck to make the chin shorter and fat injections to the labiomental fold.
The other option, since fillers works so well, is fat injections with the hope that some of the injected fat survives.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hey just wondering at what age would you perform skull reshaping surgery? Would it be 18 or fully grown or what age would you consider performing this surgery? Thank you
A: Adults age 18 and older is the minimum age for skull reshaping surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a question about the general behavior of implants when removed. Perhaps you can answer this: Does removing implants after 6 months cause any permanent tissue damage and face changes? Does it create saggy skin or slightly change your appearance, etc? Or will the face and muscles go back to normal with some very minor tissue damage (only where the cuts were done during surgery, etc)?
A: The best way to think about any implant removal in the face is that the face will never return to 100% normal after implants are removed. It is just a question of how close it returns to normal which will be dependent on what type material composition) of facial implants have been removed, their size and shape and their facial location.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have recently had a canthoplasty to fix my eye asymmetry and tilt 6 months ago. I’m at the point now where I believe I need more volume with infraorbital implants. Is this possible after me having a canthoplasty?
A: Having a prior lateral canthoplasty does not preclude getting infraorbital implants secondarily.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can i still get infraorbital malar implants if i got a cheekbone reduction before?
A: That is not an implant limitation. Custom infraorbital malar implants can be placed over any bony anatomy regardless of its prior surgical changes.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am writing to inquire about potential surgical options to address my lifelong condition which I believe to be Brachycephaly. Please find attached photos and a video for reference. The key concerns I have are as follows:
1) Bulb-like appearance due to protrusion above my ears on both sides of my head.
2) Asymmetry caused by one side protruding more than the other.
3) Different protrusion of my ears, causing an imbalance.
4) Brachycephaly causing a noticeably large head with a circumference of 59cm/23.22 inches, often inviting unwanted attention and comments.
5) Flat shape at the back of my head, deviating from what is considered typical.
6) Abnormally high, top part of my head.
A change in my head shape would significantly impact my life in various ways. After discovering your work while researching similar cases, I am optimistic about finding a solution. Your expertise in this field is truly life-changing for individuals like me who have faced social challenges.
As a resilient and positive person with a strong support network, I am eager to explore options to address this condition. I appreciate your time and dedication to your profession.
A: You are referring to these procedures:
1) Bilateral Temporal Reductions
2) Left Setback Otoplasty
3) Custom Back of Head Skull Implant
4) Sagittal Ridge Skull Reduction
Any combination or all of them can be performed during the same surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, . I was born with a left-side form of facial asymmetry due to underdevelopment of various facial structures. My left eye sets lower than the right and my left cheek bone is flatter than the right. I also have some chin asymmetry. I am not looking for my face to be perfect just hoping for more facial asymmetry. I look forward to hearing from you.
A: Based on your comments your primary areas of facial asymmetry concern are: 1) left eye, 2) left cheek and 3) chin. The correctuve procedures would be: 1) Left cheek implant, 2) chin asymmetry osteotomy and 3) left orbital floor implant with eye corner adjustments. You have correctly surmised that improvement is the realistic goal not perfect symmetry.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a webbed neck. I have dealing with it for 50 years. I always wanted to improve the appearance of my neck. I’m unsure if I can gain more natural movement but I’m interested in finally achieving a goal of having a smaller neckline.
A: You have what appears to be a mosaic type of webbed neck which typically has less wide neck webs. But the skin and deeper soft tissues are tight and, as a result, does not respond well to webbed neck surgery.
FYI. Webbed neck surgery does not improve the range of motion of the neck.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I read your post regarding filling the step-off that occurs with sliding genioplasty.
Does this bone fill eventually become solid bone that is fused to the chin structure? Or does it remain bone chips? I’m fascinated by this technique as I worry that the step off of a sliding genioplasty will be visible and noticeable, especially in the jawline. How does this technique address these concerns?
A: I assume you are referring to the central stepoff of a sliding genioplasty as opposed to the lateral stepoffs that occur along the inferior border. The blog post to which you cite refers to the central stepoff as opposed to your description which refers to the potential lateral jawline stepoff.
As a general answer to your question about the fate of the use of cadaveric bone chips, if placed during the primary procedure, some of it turns into bone and some of it becomes fibrous scar tissue. But in either case it serves as a volumetric fill which its primary objective.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
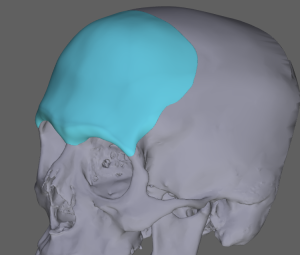
Q: Dr. Eppley, I am interested in potentially getting skull reshaping as I feel my head (temple area) is very narrow at the top instead of round. I have a heavy bottom/jaw that’s wider than my forehead. Would like it to be more balanced. Can I get information and range of potencial cost?
Thank you
 A:Thank you for your inquiry and sending your pictures. What you are referring to are extended temporal or head widening implants that wrap around the side of the head to create increased width. Attached is an example of the concept as well as potential changes in you. (which can also be more or less)
A:Thank you for your inquiry and sending your pictures. What you are referring to are extended temporal or head widening implants that wrap around the side of the head to create increased width. Attached is an example of the concept as well as potential changes in you. (which can also be more or less)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a question about chin reduction through the submental approach. From a lateral view, the protruded chin should be brought to the level of the lower lip. However, from the frontal view, what changes can we expect? Will the shape change considerably? If the patient wants it, could the shape of the chin be preserved? For example, keep a square chin square after the bone reduction.
Please advise
A:In a horizontal chin reduction the bone is reduced back and its shape can either be maintained or changed based on the patient’s aesthetic desires. Keeping a square bony chin shape is a predictable outcome.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve done a bit of research on clavicle shortening surgery. I’m a 23 year old female, however my shoulders are really borad compared to the rest of my body. I do have some questions before booking a vitual meeting for the surgery.
As I’m coming from Denmark, and travelling alone. What is the minimum required of days to stay? I can’t stay for too long. And do you offer a place to stay after surgery, when travelling alone (of course paid)
Will the surgery cause my shoulders to roll inwards, making it look like I have a bad posture?
And is there any long term risks of the surgery, which you’ve seen with your patients? Such as nerve pain/damage, pain in shoulders/arms, or lower mobility? , or any impact on the back muscles during time?
Can I expect any complications during pregnancy or birth?
Will the metal inside the shoulders cause any trouble when visiting airports?
A:You have correctly surmised that the biggest issue in clavicle shortening surgery, particularly for overseas patients who are traveling alone, is the immediate postop recovery logistics. We advise all of such patients to stay at the Hyatt Place right next to my office and very close to my surgery center which makes everything easier. I would anticipate you returning home 5 to 7 days after the surgery.
The surgery does not cause the shoulders to roll in to any significant degree nor does it affect your posture once fully recovered.
I have seen no adverse musculoskeletal effects from the surgery.
The surgery will cause no issues with subsequent pregnancies.
The metal hardware used is titanium which is both MRI compatible and not a problem with airport scanners.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley ,Hello, can you provide a price range for what forehead augmentation with pmma might cost for a man at your clinic? I understand you can’t give specifics but I’m just exploring the idea at this point and am wondering what I should be planning for. Thanks
A:PMMA is a very limited forehead augmentation technique that has many liabilities which as a result I no longer use it. I only use custom made forehead implants now due to their far superior controlled aesthetic results and lower risk of complications…not to mention a smaller scalp incision to place it as well.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, One part of my discussion with the doctor is the possible lowering of eyebrows, which may be done by upper eyelid incision. This is not included in the agreement. I am assuming that this would be a part of my forehead implant augmentation procedure.
A: As stated earlier an upper eyelid incision is typically used for custom forehead-brow bone implants to make sure the implant is seated low enough over the brow bones. In so doing optimal release of the brow bone tissues is done. Whether this will make the eyebrows become lower is not predictable, as these tissues are very tight and have little stretch, but between that maneuver and the implant whatever lowering of the eyebrows that is possible will be achieved.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
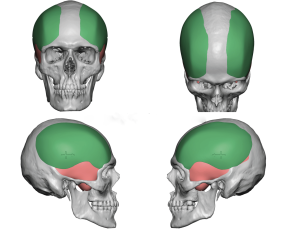
Q: Dr. Eppley,Idk If I had brachycephaly but my head is wide from the sides and kind of flat in the back could I remove temporal muscle and combine with a prosthesis in the back, as my face is round with my head wide looks 0 aesthetic, dr, do you think that tia could work? I leave a pic of my head
A: You have correctly surmised that the combination of temporal reduction (see attached imaging) to narrow the sides and a custom skull implant for the back of the head would be the combination of skull reshaping procedures that would provide the head shape changes you desire) That is a good bidimensional change for the wider but short (front to back) skull shape.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to know if i would be a good candidate for any facial implant that could make my undereye/ midface volume loss disappear. I’m going to send some pictures as attachments.
Thank you for your time and help!
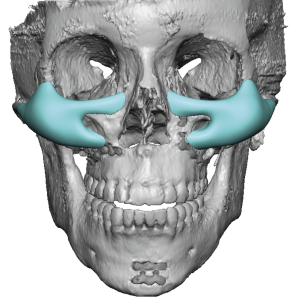
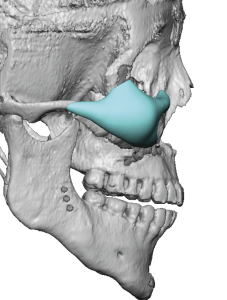 A:You have small facial bones with underdeveloped/weak bone structure around the eyes and cheeks. This not only appears as midfacial volume loss but makes the normal infraorbital fat look herniated, the lower eyelids sag with scleral show and the eyes appear overly prominent. The only effective treatment is a custom infraorbital-cheek-maxillary implant. (see attached images)
A:You have small facial bones with underdeveloped/weak bone structure around the eyes and cheeks. This not only appears as midfacial volume loss but makes the normal infraorbital fat look herniated, the lower eyelids sag with scleral show and the eyes appear overly prominent. The only effective treatment is a custom infraorbital-cheek-maxillary implant. (see attached images)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Good afternoon! I was your patient last year for infraorbital malar implants and the results are amazing! This time in interested in lateral comissuroplasty for making bigger and wider lips. I would like to know if it can be performed under local anesthesia? What is the possible widening? Thank you very much and have a wonderful day!
A:Good to hear from you again and I am very glad your IOM implants worked out well. When it comes to mouth widening surgery, which can be done under local anesthesia, the key concepts to grasp about it are:
1) The mouth corners will be lengthened (widened) but that does make the corners wider. (increased vermilion show – see attached imaging)
2) The need for scar revision on mouth widening is not low.
3) The alternative approach to your concerns are lateral vermilions advancements which will make the outer portions of the upper lip wider/fuller, may increase the mouth width a few millimeters and has a low scar revision rate. (see attached imaging)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Would you ever consider doing cosmetic work on the femoral heads/acetabulum?
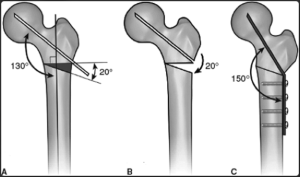 I’m a male with unfortunately wide hips. I think this is due to either a genetic condition or a lack of high testosterone during puberty. Anyway, being 23 now, options to amend this cosmetic issue are very limited. I know from some of the other questions you answered, you may or may not offer “iliac crest reduction” which you say could help. My issue is that the size of my hips aren’t really a matter of the iliac crest. They’re instead because of the femurs. In general, I think most surgeons steer clear of touching the femurs since they’re obviously super critical to locomotion and daily activity. However, in researching this subject, I’ve noticed several medical procedures I think may reduce the distance between the femoral heads (and thus the hip width). I’m talking about things like total hip replacement, femoral angle of inclination surgery, and possibly even acetabulum deepening.
I’m a male with unfortunately wide hips. I think this is due to either a genetic condition or a lack of high testosterone during puberty. Anyway, being 23 now, options to amend this cosmetic issue are very limited. I know from some of the other questions you answered, you may or may not offer “iliac crest reduction” which you say could help. My issue is that the size of my hips aren’t really a matter of the iliac crest. They’re instead because of the femurs. In general, I think most surgeons steer clear of touching the femurs since they’re obviously super critical to locomotion and daily activity. However, in researching this subject, I’ve noticed several medical procedures I think may reduce the distance between the femoral heads (and thus the hip width). I’m talking about things like total hip replacement, femoral angle of inclination surgery, and possibly even acetabulum deepening.
Yes, those procedures are all medical. But as cosmetic surgeon with willing patients who accept the possibility of risk, why not appropriate them to cosmetics? I think myself and thousands of other unfortunate men would flock to it.
A:My two comments would be:
1) Those type of greater trochanter/femur manipulations are within the province of an orthopedic surgeon not a plastic surgeon.
2) In the diagram attached I would doubt that the narrowing effect on the ‘hips’ would be externally noticeable…and it would have to be to justify that effort and risk.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had brain surgery 30 plus years ago that has left me with 2 small divots which I am trying to have filled.
A:With a prior history of a craniotomy, or at least burr holes for decompression, those divots would represent the through and through skull defects from that procedure. Such burr holes defects can be covered over with a variety of materials from bone cements to implants. I suspect a bone cement material would be fine but it would be worthwhile to check an x-ray before doing any surgery so there is a full understanding of what lies underneath these indentations.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,Hello, I am based in London and have nearly exhausted my list of potential oculoplastic surgeons following a few consulation.
I’ve had recommendations for the following combinations : bilateral ptosis repair , lower lid retraction with hard palate graft, lateral tarsal strip.
Orbital decompression , lower lid retraction, bilateral ptosis, canthoplasty
Infraorbital implant , bilateral ptosis , lower lid retraction.
The surgeons seem to disagree and I am considering travelling to the states for treatment . Would you be able to tell me if you think you could help?
I don’t like the bulging/prominent eyes or the droopy eyelids.
Thank you for your time
A:These various recommendations are not as different as they may seem. It is more about the variations in how to treat the 2 obvious eyelid situations you have, mild upper eyelid ptosis and more significant lower eyelid retraction….with the underlying skeletal issue of an infraorbital rim deficiency. (which is one reason you have lower eyelid retraction)
The eyelid ptosis correction recommendation is a uniform one across the board. The ‘debate’ is in how to treat the lower lid retraction, specifically the ‘eyeball protrusion’ part of it, and the only controversy is whether it is better to drop the eyeball deeper into the orbital box (orbital decompression) or build it out the deficient infraorbital bone. (implant) Both are different ways to try and help the lower eyelid retraction repair work better. Most oculoplastic surgeons are going to recommend orbital decompression because that is a procedure in which they are more comfortable performing and it is an historic one in their toolbox so to speak. (doesn’ t necessarily mean it is the better procedure, just one in which they are most familiar) Building out the infraorbital bone is the opposite approach of which a custom infraorbital implant design is the superior implant method to do so. You choose this approach if you prefer the lower eyelid change as seen in the attached image.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had surgery done on the back of my head in 2011 I believe. The back of my left side head was so flat and the flat part was gone after the surgery. Even though the flat part was gone overall my head is still flat. Over the years as I got older I lost my hairs a lot so I don’t have enough hairs to cover my ugly head shape. Can you make my head round and presentable?
A:Back in 2011 the only skull onlay augmentation method that was available was different types of bone cements which have their limitations. Today I no longer use bone cements for aesthetic augmentations and this has been replaced by a custom made skull implants which offer far superior results in terms of both shape shape and volume…often 3 to 5X more than what bone cements could achieve.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi there I was interested in revision rhinoplasty I got my rhinoplasty 8 months ago but not happy with the shape and scarsAs one side I feel is slimmer then the other side and I can feel it with my finger and it tilts more to one side slightly.But was wanting my tip pretty narrow and slim as it looks almost identical to how my tip was before the surgery just wanting to know if possible.
A:Since I don’t know what your nose looked like before and what was done exactly in your rhinoplasty surgery it would be impossible to say whether further improvement is possible. I would need before and after pictures as well as a description of what type of rhinoplasty was done. (e.g.., rib graft, implants etc) The scars along your nostril bases indicated that you and nostril narrowing/nasal bases reduction. Usually those scars can be secondarily improved.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in paranasal-maxillary implant because of the lack of support and projection I have in my midface, specifically around my nose and in my upper lip/philtrum. I was looking into Lefort 1 orthognatic surgery, as I do have a very slight Class 3 malocclusion, but both surgeons and orthodontists discouraged me because it’s very mild. The issue is I still struggle with this lack of support, my midface kind of sinks in when I smile, my nose drops (even after two rhinoplasties) and my upper lip flips in a horizontal line over my philtrum. I also dislike the proportion of my nose in relation to my face, and the prominent nasolabial folds, at only 24 yrs old. The question i’m asking is can a paranasal maxillary implant create similar results in soft tissues as a Lefort 1 advancement ? I understand the osteotomy is probably way more dramatic in inducing a change, but could the results be similar?
A: The fundamental differences between a LeFort I advancement osteotomy and nasal base implants (paranasal-premaxillary-maxillary) is at the dental level. A LeFort I osteotomy can push out the upper lip as the lips rests on the upper teeth. So any forward dental movement (the LeFort I bone contains the teeth)mwill push out the vermilion of the upper lip as the bone moves forward. The effects of implants is relegated to all of the bone above the dental level. That being said in the description of your symptoms most if not all of them could be improved by nasal base augmentation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, does you perform cosmetic testicular implants/enlargement?
Is the nerve to the cremasteric muscles transected or is botox used during the procedure
is the feel or hardness of the implant similar to the native testes?
A:No nerves are cut during the testicle implant placement procedure. If cremaster muscle relaxation is needed Botox injections should be done a few weeks to a month before the procedure.
Testicle Implants are made of a solid but ultrasoft silicone material that is designed to approximate the feel of the normal testicle.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, hi I’m looking to achieve a more heart shaped face shape but I don’t want to look older. is that possible? I’m 21 years old.
A:Based on a review of your pictures your biggest limitation from a more heart-shaped face is the lack of vertical chin length. The benefits of vertical lengthening towards that type of facial change can be seen in the attached imaging. Whether that makes you look older is a judgment you will have to make for yourself.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I hope this message finds you well. I was wondering if I would be a good candidate for buccal fat lipectomy and/or perioral liposuction as I want a slimmer face between my cheeks and jawline with the goal of a more angular-looking masculine facial shape. And if so, I would like to know what the price would be for these procedures.
For reference, I’m a 21-year-old male who’s 6’2 and has fluctuated between 180-190 over the last 1 1/2 years. Despite the rest of my body being pretty skinny, my face appears very bloated to me and very round. I do think my cheekbones are big and rounder than most people due my dad’s side having big and round cheekbones. However, I still think my face carries too much fat and it just doesn’t fit the rest of my body being pretty skinny. I drink plenty of water as well every day and do about 30 minutes of cardio exercise everyday.
The last time I felt that my face didn’t feel very bloated was when I was hovering around 170 lbs around 2 1/2 years ago but I don’t want to be at that weight because it just seems too skinny for the rest of my body. I would ideally like to be around my current weight or even around 200 if I decide to get into weightlifting in the future.
I also noticed that the right side of my face is wider than the left side of my face and so I wasn’t sure if correcting that asymmetry would also help my face in looking more slimmer. My dental arch on the right side of my face also isn’t as wide as my left side as you can see in the photo where I’m smiling, so I wasn’t sure if invisalign would help with this asymmetry by narrowing the right side of my face as I’ve read about people’s faces narrowing after invisalign expansion of the dental arch. I’m not sure if this claim is true or would be applicable in my case.
I was also wondering if you know if there are any risks invisalign could have on my face if I decide to get that in the future to correct my smile if I do end up getting a potential buccal fat lipectomy and perioral liposuction in terms of the risk of my face look too gaunt or narrow.
Thank you for the help!
A: In answer to your questions:
1) You would be a good candidate for facial defatting via buccal lipectomies and perioral liposuction. However be aware that one can never defat their face into a more angular shape…that degree of change is not completely realistic from a soft tissue reduction alone.
2) Facial asymmetry correction will not make the face any slimmer, just more symmetrical.
3) I see no adverse risks of undergoing Invisalign on your external facial shape.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I am interested in deltoid implants to have a bigger looking shoulder. Is this something you do?
A:Thank you for your inquiry and sending your video. While the clever sleeves you put over your deltoids (which is what you may wear under your clothes to create an enhanced deltoid appearance) are not the exact shape of deltoid implants or how they are placed under the muscle, they do convey a sense of deltoid augmentation size. How thick are these sleeves at their widest part which would help choose the size of deltoid implant for you?
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hey, I just had a random question for Dr. Eppley. I was just watching this debate and noticed the face of this one journalist. To me it looks like she had plastic surgery and it’s too obvious. I was wondering, am I right about that, and if so how can we avoid the same look on my face.
A: I can not say whether this person has had facial plastic surgery or not. It is just as likely that is her natural face and makeup highlights her prominent bone structure. But she has a lean long face and your facial structure and skin is different. It would be fair to say you couldn’t make your face look like that even if you wanted it to.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Good morning, sir. I’m inquiring about the upper orbital period, and I want my forehead and eyebrow bones to pop out. The forehead near the forehead hairline is lying back, so I want this part to be raised at a right angle and make an eyebrow bone, but I wonder if it’s possible as a surgery. And I wonder how much it costs. I’d like to know the operation time, recovery period, and operation method.
 A:You are specifically referring to a custom forehead-brow bone implant (see attached), the most effective way to achieve this upper facial shape change. Placed through a limited scalp incision behind the hairline it takes about 90 minutes to surgically placed. Recovery is all about swelling of which it will take about 10 to 14 days to look non-surgical.
A:You are specifically referring to a custom forehead-brow bone implant (see attached), the most effective way to achieve this upper facial shape change. Placed through a limited scalp incision behind the hairline it takes about 90 minutes to surgically placed. Recovery is all about swelling of which it will take about 10 to 14 days to look non-surgical.
Dr. Barry Eppley
World-Renowned Plastic Surgeon