Your Questions
Your Questions
Q: Dr. Eppley, I had a sliding genioplasty four weeks ago. It involved a +3mm lengthening, +3mm projection, and +4mm widening. As my swelling has gone down, I realize that from a side profile view I like the lengthening and projection achieved, BUT, from the front view I see that my chin is asymmetric. I like how the left side of the chin looks, but on the right side the chin looks ‘sunken in’ – as if the bone segment were angled more inwards (and maybe upwards) in comparison to the left. The right looks ‘slimmer’ and left looks ‘fuller’ in comparison. It’s subtle, yet obvious. I can also feel this difference when gently running my fingers down/along the chin. Could you please advise regarding the appropriate solution, and the associated timeline? I would like to take this forward with you at the soonest.
A:Thank you for your inquiry and sending your pictures. I believe the answer is clearly seen on your x-ray which shows the more prominent inferior border stepoff on the right side due to exactly what you have described. (see attached) Your visible and palpable symptoms match what your x-ray shows. This is a contour deformity along the right inferolateral border of the chin. There are two approaches to resolve it; 1) immediate intraoral bony adjustment to rotate the segment out and down or 2) delayed implant coverage of the bony defect, probably using ePTFE from a submental approach. Each approach has their advantages and disadvantages.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,I’m hoping you could help me here. I had a reduction genioplasty 8mm bone shave. The outcome looks awful but I’m now suffering with tightness in the chin. I feel like I’m unable to move my chin. It feels tight where the muscle has been stitched. My intraoral incision has scarred to high up on my tooth line. My mouth movements look funny and I also can’t retract my lower lip downwards. Not being able to show any of my bottom teeth this also has an effect on my speech and movements. I’m so scared to have another procedure because of the amount of scarring I have. I have attached some pictures for you to see. My chin also looks lumpy.
A:I believe we have had this discussion previously but to review it again. A large shave down intraoral bony reduction genioplasty is never a good idea and is prone to a lot of potential problems…many of which you have. Once such a large amount of bony support is removed where does all the enveloping soft tissues go? Unfortunately it does not just shrink down and adapt around the reduced bony chin. Rather it turns into a ball of contracted muscle and scar tissue which is both stiff and immobile. The contour also become irregular due to the soft tissue contracture. I see no other effective option for improvement but to release the scarred soft tissue chin pad and put back some of the bony support lost. (aka sliding genioplasty) Whether the movement should be a partial or complete restoration of the lost bony projection can be debated.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am looking into deltoid augmentation through fat grafting. Is this something you have done in males? Is the result permanent?
A:I have done fat grafting to the deltoids numerous times in men. Like all fat injections the survival is not always 100% predictable but what does survive should be permanent long term.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have an average jaw and chin. I was wondering if the off the shelf implants would suffice, or if the custom chin wrap would be more fruitful. I would love to consult with you and compare options. I have included pictures for computer imaging.
Thank you,
A:I have done some initial jawline imaging which should be interpreted as follows:
‘The purpose of computer imaging is frequently misunderstood by patients. Computer imaging is done to help determine what the patient’s aesthetic goals are. It is a method of interactive visual communication between the patient and surgeon to help establish what your specific goals are. Your task is to evaluate this initial imaging and determine what you like and don’t like about it. Then I adjust the imaging to make it the way the patient wants it. This then establishes the aesthetic target from which I design the operation to try and achieve.’
There are significant aesthetic outcomes, risk considerations and cost differences between the use of 3 standard implants and a one piece custom implant approach to jawline augmentation. But when you break it down to the most simplistic level there is one and one reason only that a patient may choose standard implants over a custom designed one….cost. The use of standard implants has inferior aesthetic results and a higher risk of implant placement asymmetries.
Dr. Barry Eppley
Indianapolis, Indian
Q: Dr. Eppley, I am a naturally broad shouldered female with narrow hips. I am interested in a hip augmentation procedure to widen the width of my hips in proportion to my shoulders. I likely do not have enough donor fat to have a fat transfer to the hips, so I am primarily interested in hip implants.
A few questions:
Does you always use custom implants shaped for the hip region?
Do synthetic hip implants need to be replaced after some years?
Can hip implants be felt when touching the hips?
Is there a danger of hip implants migrating, given that the area is above a joint?
A:In answer to your hip implant questions:
1) Since there are no standard hip implants available, all must be made custom.
2) Like all body implants, other than breast implants, they are solid, do not degrade or breakdown, and thus never need replacing due to device failure.
3) How palpable they are depends on how much soft tissue cover you have.
4) Hip implants do not migrate once well healed. There are no joint issues as these implants are placed on of of the TFL fascia which is well away from the hip joint.
5) When considering hip implants I would read the following statement based on my extensive hip implant surgery experience:
‘Hip implants have a fairly high rate of complications so patients have to be selected very carefully to try and lower those risks. There are two major risk factors, 1) thin patients with little subcutaneous fat (inadequate
soft tissue cover) and 2) implants that are too big. (too thick for the tissues to adequately support them) Both of these hip implant considerations are judgment issues with no absolutes. Before a patient should
consider hip implants they should exhaust every other method of hip augmentation and to be aware that it is a procedure that is in a state of evolution and is far from a perfected surgery’
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am potentially interested in a skull reshaping procedure, specifically crown augmentation. I was wondering if you could answer a few questions for me.? How long is the recovery in general? Is hair loss at the incision site common?
Thank you very much,
A: In answer to your skull augmentation questions:
1) Recovery from any skull augmentation procedure is fairly quick but depends on how you define recovery. Other than swelling, which may or may not drifty down into your face, there are no real physical limitations after surgery other than what feels comfortable.
2) Hair loss around the incision site is very limited to just that of a fine scar line in most cases.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I also had a few practical and technical questions about soft tissue jaw angle implants to treat masseteric muscle dehiscence:
1 – Once I commit to the surgery, how long does the planning process take leading up to the operation date? (I.e. will I need new 3d CT scans)
2 – After the surgery, how acute is the swelling compared to the jaw angle surgery, and how long until the soft implant is stable? (wondering how much social downtime would be need\ed, and when I could resume contact sports afterwards)
3 – Is there significant risk with the external incisions of the soft tissue implant becoming infected (i.e. compared to the jaw angle implants), and is there additional risk that the already placed jaw angle implants could become infected as a result of the new soft tissue implants?
A: In answer to your questions:
1) Soft tissue jaw angle implants are done based on external measurements of the soft tissue defect (draw on yourself the triangular shaped contour defect and then measure the three sides of the triangle on each side) and are then converted into a computer design from which the implants are made. A CT scan is not required as it does not see soft tissue in 3D.
2) Unlike the original surgery this is very minor with a quick social recovery. (a week or less)
3) External incisions and implant placements are not associated with the same infectivity risks of placing large implants intraorally.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m having a bilateral orchiectomy next month. Right side is potential stage 0. I opted to have both removed at once so that I can do implants later on. I don’t like the size or the idea of doing fluid filled ones. I want some big ones if I’m going all in. I assume you custom make the implants?
A: Any solid ultrasoft silicone testicle implants bigger than 5.0cms are custom made…typical sizes range from 5.5 to 7.5cms.
Dr Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, my main concern is my nose. I would like a more feminine nose. I think the bridge is to wide I have a hump and my nostrils are much to wide and large. I have had trouble finding a surgeon that will reduce the size of my nostrils. I’ve been told they may look pinched and one surgeon said they might look sorta mashed.
A: Thank you for your inquiry and sending your pictures. Thick skinned noses pose challenges in performing as well as limitations in the results compared to noses with thinner skin. That being said i do think positive changes can be obtained. (see attached) When it comes to nostril narrowing previous opinions are undoubtably based on the most commonly used approach for nostril narrowing which is that of an internal wedge removal. It is true if that method was used the nostrils would indeed have an unusual shape. But that not be the appropriate method of nostril narrowing for your type nose. You need the full thickness nostril wedge reductions which shorten both their length and width.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, i had buccal fat removal twice. Most recent one was 2 years ago so im over the swelling phase. The doctor claimed he took out all the fat but my face still looks fat in the area where ive drawn the red arrow.
What on earth is going on and please tell me theres something i can do.
A: Where you are indicating in the red arrows in your picture is NOT where the buccal fat pads are located. They are located much higher closer and their removal will have no effect on your indicated areas. There are the perioral mound areas which have to be treated by small cannula liposuction through a small incision inside the corner of the mouth.
Dr. Barry Eppley
Indianapolis, Indianapolis
Q: Dr. Eppley, I really hate my wide, feminine hips and dream of having really narrow masculine hips. Can this be achieved by shaving down the tronchater or something similar? If so, I’d be quite concerned about chronic pain or other complications post surgery.
What would the actual procedure be? Cost? Scarring? Complications? Chance of resultant chronic pain?
A: Shaving of the greater trochanter of the femur is NOT a surgical option. There are too many soft tissue attachments to this bony head that would need to be stripped off to justify any aesthetic reduction of it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Due to a car accident two years ago I have deltoid paralysis in my right shoulder due to axillary nerve impingement. I was wondering if you could help me find my way back to have even looking shoulders.
A: Thank you for your inquiry. The first place to start is to send some pictures of the affected shoulder for my assessment. But as a general statement deltoid muscle atrophies are typically treated successfully with custom implant designs.
Dr Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, i want to improve the appearance of the lateral hooding of skin at the corners of my eye lids, my brows are straight and i feel a little low. I am confused as to whether i need a brow lift or eye lid surgery, I am getting mixed opinions.
I would value your expert opinion.
A: Based on your picture the most effective resolution of your temporal hooding is excisional. (upper blepharoplasty) You can not ‘browlift’ the temporal hooding away. If you feel the brows are low and may desire a browlift for that purpose that can be done at the same time. That may affect how much skin is removed when done at the same time as the lateral upper blepharoplasty. The browlift is an adjunctive technique to the blepharoplasty but not a replacement for it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, In regards to the saddle infraorbital implant, I am just wondering, is there any risks associated with the saddle? Like the edge of the orbital bone eroding, or just general safety issues associated with silicone entering the eye socket?
Also, is this implant commonly requested for? So few surgeons do this implant world wide and it surprises me considering how great of an aesthetic boost it gives. It’s seems even better than procedures like canthoplasties which tend to give uncanny results in comparison. I’m puzzled why this isn’t more popular.
Thank you for your time.
A: In regards to your questions in regards to custom infraorbital or infraorbital-malar implants:
1) I have never seen any evidence of implant bone settling (what is often erroneously called bone erosion) clinically or on 3D CT scans. Nor would I expect it in an implantation site that does not a have a tight muscularized soft tissue cover.
2) These custom implants are for aesthetic conditions that are associated with various degrees of orbito-zygomatic skeletal underdevelopments or retrusions. These are externally seen in various clinical conditions such as lower eyelid sag with scleral show, undereye hollows, negative orbital vectors, flat cheeks and overall midface retrusions.
3) The development of any surgical technique first begins with awareness followed by acceptance which then leads to common use.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have had 800 CC gummy bear implants for 5 years. I would like to increase my size to 1000 or 1100 CC silicone memory gel implants, small base high projection.
A: Thank you for your inquiry. In the U.S. the maximally allowable silicone breast implant size by any manufacturer, including Mentor, is 800ccs. There are no 1100cc silicone breast implants. Any breast implant volume over 800ccs must be done by saline implants that are overfilled. In XL breast implants 800ccs high profile saline lmplants filled to 1100ccs is how that would be accomplished.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a chin implant last October by a plastic surgeon in my country… after a few months i notice food particles entering the incision i tell my doc about it he keeps assuring me it’s normal, after removing the stitches the wound/ incision widen and more food enters. Now I’m left with
Something that looks like open wounds in my gums. Last time i saw my surgeon he advice me to “wait for it to heal i cant stitch it yet because there’s no enough skin ” how can i help it heal properly? Is it due to the size of the implant? Should i ask my doc to re-open and stitch the wound ? Idk what to do it’s uncomfortable when i talk i feel a weird pulling sensation even after 6 months.
A: That is a completely healed intraoral vestibular incision. It is a lot of white scar but a healed wound nonetheless. The tightness you feel is a result of the implant placement which is always higher than ideal because of the intraoral approach and the lack of screw fixation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a problem with face retrusion as a complete front area of face. I have discussed my concern with one of my friend who has contacted you on the past. Acording to him you are very skilled on face augmentation by cranium bone grafts. So I’m interested in using bone grafts.I have 2 questions and I would be very grateful for your kind answers.
So:
1. When you harvest the bone from the head, how much thicken graft can be taken. For example 3 or 4 millimeters thicken graft. So on your experience how much is the maximum thicken graft that you can harvest from the head for face augmentation without any problem on the head on the future. This will help me having an idea if it will meet my wishes.
2. Does the bone graft may include complete front of face up to around the nose. So this way it is necessary using too much grafts. So only front of face starting from zygoma, orbital rim and all front face up to around the nasal bone and maxilla . For me it is important that bone grafts being up to nasal bones
To explain better you may see attached the foto with facial mask custom implant. So my wish is including complete front of face augmentation as implants in foto.
Can be achieved the same area augmentation by bone grafts. Is that any problem to augment full front of face up to around the nose and around the eyes by bone grafts. So not only cheeks or malars.
Many thanks for any answers.
A: Thank you for your inquiry and sending your illustration to which I can say the following:
1) While bone grafts may be appealing compared to implants for midface augmentation, they are comparable in terms of effect. They are not completely interchangeable concepts.
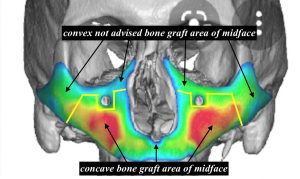 2) Because of the hard inflexible (unbendable) nature of block cranial bone grafts, they can only be placed on concave midface surfaces. Trying to place them on convex midface surfaces will result in a lot of palpable/visible irregularities. To illustrate those different midface zones I have attached an illustrated diagram. (see attached) These convex areas may be treated by allogeneic (tissue bank) bone chips as they can be applied with less irregularities. How well such bone chips survive is variable.
2) Because of the hard inflexible (unbendable) nature of block cranial bone grafts, they can only be placed on concave midface surfaces. Trying to place them on convex midface surfaces will result in a lot of palpable/visible irregularities. To illustrate those different midface zones I have attached an illustrated diagram. (see attached) These convex areas may be treated by allogeneic (tissue bank) bone chips as they can be applied with less irregularities. How well such bone chips survive is variable.
3) The average thickness of most harvested outer table cranial bone graft is in the 4 to 5mm range.
4) Given the volume of bone grafts needed an argument could be made for use of rib grafts which are more easily harvested and are more flexible/bendable.
5) Only a custom midface implant can reliably cover all indicated areas in a smooth fashion. Thicknesses of such implants are what one designs them to be.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a sliding genioplasty four weeks ago. It involved a +3mm lengthening, +3mm projection, and +4mm widening. As my swelling has gone down, I realize that from a side profile view I like the lengthening and projection achieved, BUT, from the front view I see that my chin is asymmetric. I like how the left side of the chin looks, but on the right side the chin looks ‘sunken in’ – as if the bone segment were angled more inwards (and maybe upwards) in comparison to the left. The right looks ‘slimmer’ and left looks ‘fuller’ in comparison – this is something that my girlfriend and another close friend confirmed as well. It’s subtle, yet obvious. I can also feel this difference when gently running my fingers down/along the chin. Could you please advise regarding the appropriate solution, and the associated timeline? I would like to take this forward with you at the soonest.
A:Thank you for your inquiry and sending your pictures. I believe the answer is clearly seen on your x-ray which shows the more prominent inferior border stepoff on the right side due to exactly what you have described. (see attached) Your visible and palpable symptoms match what your x-ray shows. This is a contour deformity along the right inferolateral border of the chin. There are two approaches to resolve it; 1) immediate intraoral bony adjustment to rotate the segment out and down or 2) delayed implant coverage of the bony defect, probably using ePTFE from a submental approach. Each approach has their advantages and disadvantages.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I just wondering on having a high forehead with no loss of hair or receding. Would I get a forehead reduction or hair transplant. My dad and mom have huge foreheads. I’m 21 and want to make it smaller but I’m nervous about the scar and stuff
 A:Because the often inadequate hair densities obtained with hair transplants for forehead reduction I would strongly suggest a frontal hairline advancement. Understandably one would be concerned about the scar but having done a lot of male hairlines, particularly in patients with darker pigmentations, it actually does very well and I have not seen it to be a significant aesthetic issue.
A:Because the often inadequate hair densities obtained with hair transplants for forehead reduction I would strongly suggest a frontal hairline advancement. Understandably one would be concerned about the scar but having done a lot of male hairlines, particularly in patients with darker pigmentations, it actually does very well and I have not seen it to be a significant aesthetic issue.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m 28 years old and transgender (MtF) and have previously had two rounds of facial feminization surgery elsewhere. The specific procedures were brow bone reduction and trachea shave initially and chin/jaw reduction later. This has made a significant improvement to my face, but there are some points that still bother me:
1. My forehead has what I feel is a kind of masculine backwards slope, and I’m interested in the possibility of improving this with a custom implant. I’m also somewhat bothered by my flatter back of the head (around the indent that’s visible on the CT pictures). Would it be possible to address both of these issues in a single procedure, or would that put too much tension on the scalp? Also, how would the position of the hairline be affected by a forehead implant?
2. I’m also bothered by my undereye area, which I feel lacks projection and gives my face a gaunt and tired look. My eyes also have some scleral show and the upper eyelid sits lower on my right side. The right upper eyelid crease has also been asymmetric since my previous forehead surgery. I understand that infraorbital rim augmentation can improve scleral show, but would that be sufficient on its own? And would it be possible to improve the eye asymmetry issues?
3. Unfortunately my chin was reduced more than I expected, and I’m struggling to adjust to the new appearance which just feels too small and pointed. Comparing the pre- and post-op CT scans I think I also lost a few millimetres of height, which I specifically didn’t want; and there’s a bit of ptosis as well. The jaw reduction also wasn’t quite symmetric, so my jawline is now higher on the right, and on the left it’s uneven. I guess a custom implant would be my best option to address these issues?
4. I was initially scheduled to have a rhinoplasty during my original surgery, but the surgeon talked me out of it because I wanted to feminize my nose while retaining a bit of the convexity, which he said would be difficult to achieve. I’m just wondering if you have the same or a different assessment of that.
I have attached some photos, along with some views from my most recent CT scan in case those might be useful.
Any advice would be much appreciated.
Kind regards,
A:Thank you for your inquiry and sending your pictures to which I can say the following:
1) The combination of forehead and back of head augmentations can be done concurrently. The volumetric needs of both do not seem excessive. (see attached)
2) While infraorbital rim augmentation will provide needed volume the eyelid issues need their own concurrent attention for optimal improvement. The right upper eyelid has ptosis which needs a direct ptosis repair. The lower eyelids need a combination of lateral canthoplasties and spacer grafts to eliminate the scleral show.
3) As for the jawline it depends on how far you want to go with it.The chin by itself can be addressed with a standard small vertical lengthening chin implant (and leave the rest of the jawline alone) or make a custom jawline implant and address all of its issues.
4) i see no reason why our rhinoplasty couldn’t be done without leaving some slight convexity to the dorsal profile. That is simply a matter of doing what you see as best as opposed to some ideal standard. (see attached)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’ve been dealing with this issue for years. Ever since my last year of high school I’ve found out about this problem. It was quite embarrassing in high school years when I cut my hair off my last year even though I’ve grown my hair out since junior high school. Since I’ve cut my hair off it’s been harder to sleep. I trained myself to sleep on my face. Some days I wake up with bad headaches and sometimes it itches. I learned how to live with it but I think it might be time for a change somewhere.
A:It is not rare that a prominent bone bulge on the back of the head is associated with headaches and difficulty sleeping when laying on it. There is a surgical procedure to make a major change in that problem as illustrated in my prior email. (occipital knob skull reduction) This would not only provide an aesthetic improvement but is very likely going to improve the ability to lay on it and may even solve the headache issue.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, can a cleft chin (butt chin) go away after genioplasty? I really want to get rid of cleft chin I read somewhere that cleft chins are because of mentalis muscles and they can be managed during genioplasty. Also, can a very deep mental crease be made less prominent with vertical lengthening genioplasty?
A: A chin cleft may be softened by a bony genioplasty but it will not go completely away. There is nothing that can be done intraorally that can help reduce a chin cleft. The best approach is fat injections at the time of the genioplasty.
The depth of the labiomental sulcus will become less with a vertical lengthening bony genioplasty.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, is it possible to improve the ogee curve without adding width to the face? I mean, from the frontal view.
A: The ogee curve is largely an oblique facial profile view so by definition there has to be a little width added to the anterior cheek area….which will add to the facial width a little bit.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am seeking skull augmentation on one side of my forehead to achieve symmetry. The right side of my forehead lacks volume and is sloped inward, while the left side of my forehead is not. I would like to add volume to the right side of my forehead on the frontal side directly above my eyebrow and on the side of my head where the forehead is as well. Since the right side of my forehead is sloped, I would like to make sure there is volume on the top part. My ultimate goal is for my forehead to be symmetrical. I am seeking slight volume on one side of the forehead to achieve symmetry. Attached are photos of my forehead. The side that I want to augment is where I have a diamond nose piercing stud on my nose, not the side where I have the black hoop.
Let me know if a skull imaging scan will help you better understand specifically what I am seeking.
Thanks so much!
A: Thank you for your inquiry and sending your pictures. I understand quite clearly your concerns and objectives. While a 3D skull scan is needed to make the implant designed to achieve them, the concept of a forehead-temporal implant for asymmetry correction is based on what is seen externally. (see attached) The implant designed needed to effect this changes is nor particularly thick in any area but it must have a surface area coverage that is much larger than many would think. (extending fairly far back onto the temporal muscle on the side)
Dr. Barry Eppley
Indianapolis, Indiana
Dr. Eppley, I am considering whether to undergo plastic surgery for this coronal suture indentation. There are a few things I would like to ask you about this surgery.
– Can the plastic that you use if I have this surgery deteriorate over time and affect the outcome of the surgery?
– Is there any side effect caused by this operation that adversely affects my health condition after the operation?
– I understand that there are many patients who have undergone surgery similar to mine at this hospital. Are there any patients who have had serious health problems due to the surgery after the surgery?
– I am thinking of joining the American military in the future.
It’s probably two to three years from now. At that time, there is physical screening as one of the enlistment tests. If I have had surgery between the time I was born and the time I joined the military, it may be necessary to record the surgery and explain the results of the surgery by a doctor. So is it possible to prove that this surgery does not adversely affect my health or physical function, but only the cosmetic part of me? I want to be in good physical condition by the time of physical screening for the enlistment test.
With these issues in mind do you think it’s best for me to have this surgery? (Considering the postoperative recovery period and the period until the health condition stabilizes)
I am sorry that there are so many questions.
I would appreciate it if you could reply when you have time.
A: In answer to your questions:
1) The implant material does not deteriorate over time.
2) This is a cosmetic skull surgery that has not negative implications for your health.
3) No patient that I am aware has suffered any serious health problems from this surgery.
4) Your operative records will reflect that this was a cosmetic procedure in which no physical restrictions are necessary after surgery.
5) Like all aesthetic procedures it is up to the patient to determine what is in their best interest. My preoperative task is to educate the patient as best as possible about the procedure so they can make an informed decision.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am suffering with insecurities regarding my face, especially my forehead and jaw area. I know I have a facial profile typically associated to those with sleep apnea/mouth breathing and I want to change that. May I ask what I can do to my forehead to reduce the sloppiness of it so that I do not look so neanderthal-like? As I have been bullied for it alot. I am unsure if a brow bone reduction is enough, or should I do with brow bone reduction with fat grafting to the forehead?
Thank you so much for your advice. Have a lovely weekend.
A: What you need is a combination of a sliding genioplasty (in the 15mm range) and forehead (not the brow bone) augmentation. Fat grafting to the forehead would never work for this degree of augmentation. This needs a custom forehead implant. The brow bones should left alone as they are adequate for a male. It is the very retroclined slope to the forehead that is the problem.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My tragus piercing split almost a year ago. Is there any form of surgery that could help covering or fix the cleft? I am really uncomfortable and insecure with it. Thank you.
A: Just like a split earlobe, a split tragus can be equally repaired. The cleft tragalskin can be excised and put back together. The underlying split cartilage also needs to be put back together.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to get information on corners of the mouth lift and under eye hollow implant procedures. I had a midface lift with fat transfer to the undereye hollows several years ago but it didn’t adequately solve the undereye hollows.
A:Under eye hollows can be successfully treated and there are five different ways to implant the infraorbital rim area. It all depends on how much ‘effort’ one wants to put into it and one’s feeling about a synthetic vs autologous approach. The midface lift with fat injections is a typical first line autologous approach but when that proves inadequate a different approach to volume correction is needed. Options includes onlay thick alloderm grafts, dermal-fat grafts, ePTFE sheeting and implants. (standard vs custom) Each of these has their advantages and disadvantages but since you have asked about implants I will focus on that topic. There are three types of so called undereye (infraorbital) implants, standard, custom and semi-custom. (made from my library of existing custom implant designs) I generally avoid standard infraorbital (tear trough) implants because they do not saddle the infraorbital rim…a key dimensional element in creating adequate undereye hollow correction. Such custom undereye hollow implants can have a wide variety of designs around the orbital-malar area based on the patient’s aesthetic needs. (see attached examples)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am 25 years of age, I’ve dealt with plagiocephaly most of my life. The left side of my head is caved in, while the right side is pushed out. There’s a very big issue with the muscles in my neck as well due to this. This has affected the way the majority of my face, and how it’s been shaped over time. I’ve never been able to consistently live a normal life unless I’m doing a ton of maintenance via cardio, deep tissue massage, chiropractor, certain posture, sleeping on my right, refraining from moving my neck too much and so forth. This has affected me greatly. I’m humbled by the condition, but at the same time I’d rather be able to move towards there being some sort of hope or help for the matter. Any sort of feed back would be great.
A: Thank you for your inquiry and detailing your craniofacial concerns. While you have many of the skull and facial features consistent with various expressions of plagiocephaly, it is clear by your description that most of your concerns are associated with significant pain/tissue tightness. That by itself is a very uncommon issue in plagiocephaly but, more relevantly, it is unclear to me how addressing any of the aesthetic issues of plagiocephaly would improve those symptoms. That does not mean they may not but adult plagiocephaly surgery is about trying to improve the skull and facial asymmetries in their appearance. I have not seen nor would anatomically understand how such aesthetic changes would improve these pain-related symptoms.
But since the pain issue is an unknown, what we can focus on is the known, trying to improve the skull and facial asymmetry issues that you see as most important. From that perspective I would be interested in knowing what you feel are the top three issues in that regard.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had orthognathic surgery more than a year ago, in which surgery they also transferred my buccal fat pads upwards to the paranasal area.
I want them removed because it doesn’t look good.
Is it possible to remove them, if not, can Kybella injections fix that?
A: Surgical removal of the transferred buccal fad pad would be a far more effective approach than injections and could be done under local anesthesia with minimal recovery. While this is a very uncommon form of buccal lipectomies that does not mean it can to be done just as effectively as the more c
Dr. Barry Eppley
Indianapolis, Indiana