Your Questions
Your Questions
Q: Dr. Eppley, I’m looking to get a large square chin implant. Wondering if you do custom chin implants?
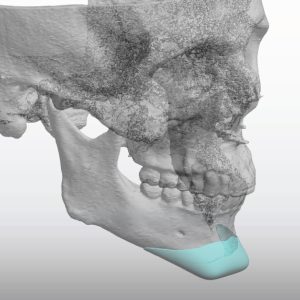
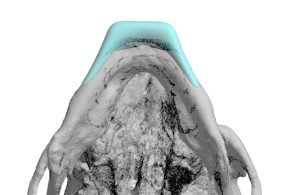 A: You have correctly surmised that the only way to get a really good square chin implant design is to have it custom made. The standard so called square chin implants are not well designed and lack the necessary shape to create a good square chin appearance, instead they just make it look wider. I have designed and placed many custom square chin implants. (see attached example)
A: You have correctly surmised that the only way to get a really good square chin implant design is to have it custom made. The standard so called square chin implants are not well designed and lack the necessary shape to create a good square chin appearance, instead they just make it look wider. I have designed and placed many custom square chin implants. (see attached example)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, can clavicle lengthening be repeated twice?
A: Theoretically it can…but that remains a theory since it has never been yet done. There is no question that it can technically be repeated. I would have concerns, however, that it might not heal as successfully as the first.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My initial V line surgery was done over six months ago. The surgery has left me in a similar place as one of your patients in the gallery. She also suffered from an over done Asian V line surgery.
One of the side effects of having so much taken off is that my bottom lip comes up a lot more than it used to. It complicates many things and is still numb in the center. It looks like I am having, or had, a stroke when I talk or smile now.
That as well as the obvious asymmetry that was already there. My hypothesis is that the asymmetry is from continued pressure supporting my face whilst reading over many years combined with an anxious habit of clenching my teeth, though I am certainly no doctor.
A: Thank you for sending all of your pictures and x-rays after V line surgery. I must say that the V line surgery you had is the most aggressive jaw bone removal that I have ever seen. To call it an overdone V line surgery is an understatement…and I have seen many. While I could have a discussion about how that was the wrong type of V line surgery for you with a natural high jaw angles (which is why the bone cut was so steep and severe) that issue is irrelevant now. Your surgeon should have known better, that was poor judgment on them.
You have correctly surmised that restoration of some of your jawline can only be done by a custom implant design to re-establish some inferior border length from the chin back to the jaw angles bilaterally.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Below are screenshots from a series I did using Facetune. I was able to adjust the skull to what i’d like to potentially achieve… but I am guessing that amount of augmentation is too much?
A: Thank you for sending all of your pictures and your own imaging. It is always hard to do such imaging when hair is present but I suspect your statement about your own imaging being too much is probably accurate….for a one stage skull augmentation. (but not for a 2 stage skull augmentation)
All skull augmentations are limited by how much the scalp can stretch at one time to accommodate an implant placed beneath it. A one stage skull segment ration means the immediate insertion of an implant whose size depends on how much the scalp will stretch. (usually 150ccs or less) A two stage skull augmentation is when a tissue expander is initially placed to stretch the scalp out first to accommodate a secind stage where larger skull implants placed. (usually 200cc to 300cc volume)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I was wondering if fat grafting to the jawline to achieve wider jaw is a good procedure? Will the fat sag in the long term and cause jowls?
A: Fat grafting would not be structurally stable as a jaw augmentation method. As you have correctly surmised it will sag and create jowls…sooner rather than later.Of equal aesthetic importance it will only create jaw fullness, not jaw definition.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, A question for you. As I know he is well renowned about custom made implant. So iIneed entire midface augmentation But I also oneed ne eye moved forward a few milimetters because my right eye is set back more than the left.
My question is can you help moving my eye forward and at the same time using custom implant for complete midface augmentation?
A: Unless the eye is posteriorly placed due to an injury (in which it at one time had more forward projection) you can’t change the natural position of the eye into a more forward position. It is important to remember that the eye is attached by the optic nerve so pulling on it to try and move it forward risk potential vision loss. Moving an eye ur or down is one thing since it doesn’t cause optic nerve stretch/injury but pulling it forward has completely different concerns in that regard.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, In the last few days the swelling from my custom chin implant has decreased a bit and the chin has more normalized but it is still excessively vertically high because the implant is very large and I would like to reduce it above all in height with a revision, I would like to ask you:
1) Going back perhaps the best choice was to opt for a genioplasty but now I have an implant positioned and fixed with screws, having to reduce it, does it make sense to shave it with the bur rather than removing it and doing a genioplasty?
2) Is it possible to reduce the prosthesis by filing it without having to remove the implant from the chin? I think it would be less traumatic to the tissue and also easier to adjust with just the right amount of reduction to do.
3) For the revision, would you make a submental access instead of from inside the mouth as was done at the time of inserting the prosthesis in order not to traumatize the same tissues a second time?
A: The mistake that is often made is that surgeons think they can do adequate reduction/modification of an implant by an in situ technique. (leaving it in place) That may be successful for the most minor adjustments of it but that will never work in your case. That would definitely not be the way to do it. Unscrew it, remove it, do what modifications are needed and then immediately reimplant it. That is the only way to successfully do it.
I also might point out that this is PEEK material…an extremely tough material that does not respond easily to any modification of it. It is the least modifiable of all facial implant materials. It will take considerable work on the back table in surgery to make the needed changes. The challenge of that task should not be underestimated.
As an addendum if you look at three options you now have:
1) Replace with new PEEK chin implant with better design,
2) Replace with sliding genioplasty, or
3) modify the existing implant
Options #3 is actually the least favorable option from an aesthetic outcome standpoint….even if it seems the ‘simplest’.
The impact of surgical trauma relates to the re-opening of the incision which has to be done with all of them so that concern is really irrelevant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi! I have been looking at your work with skull implants. I have two boys ages 7 and 9, both have plagiocephaly. My younger boy had torticollis and it made his head misshapen I tried to talk to his doctor about a helmet when he was a baby but he said it would round out by itself, that didn’t happen. With my older boy he had a skull fracture happen right before his 1st birthday he didn’t have to have surgery but I always laid him on the opposite side of the fractured side and this caused a flat spot. I feel so much guilt and blame myself and really want to find a good plastic surgeon to place an implant to round their heads out. I fear so much that they will be bullied. As a mother I want what’s best for my children. I have so many questions I don’t even know where to start. Is skull reshaping dangerous? Should they wait until they are older to think about having an implant placed? I look forward to hearing back from you! Thank you in advance for your time!
A: Such skull reshaping surgery is not done until they are past puberty and not usually before 16 years of age.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have some questions about clavicle lengthening, my clavicles are not so short but they have a “v” shape and this bothers me, can the clavicle lengthening surgery make my clavicles straighter?
A: I believe when you say V-shaped clavicles that you are referring the pronounced s-shaped curve that they have. Clavicle lengthening can not make an appreciable change in that appearance.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, In hollow wrap around testicle implants does the size of the cavity need to be customized as well so that it fits snugly? Or is there some kind of packing used at the time of surgery to fill in the gap between the natural testicle and the inner wall of the implant?
 A: The size of the internal chamber due to material constraints is fixed based on the length and diameter of the external measurements. The testicle is secured inside the chamber by sutures with the hope that it will be adequate to keep it there as it heals. A snug fit is never going to be enough by itself to keep it in place.
A: The size of the internal chamber due to material constraints is fixed based on the length and diameter of the external measurements. The testicle is secured inside the chamber by sutures with the hope that it will be adequate to keep it there as it heals. A snug fit is never going to be enough by itself to keep it in place.
If you really wanted to have an ideal match between the size of the internal chamber and the size of the testicle one would get a scrotal ultrasound where the measurements of the natural testicles can be known precisely and then built into the implant design.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in removing my current chin implant and replacing it with custom jaw implants. I would like to inquire how does this work logistically for international patients?
I) After completing the virtual consultation with Dr Eppley, are patients expected to also attend the Indianapolis office again in person? Then to the Implantech Accuscan facility have CT head scan?
2) Implant design stage? Do we attend the implant design sessions with Dr Eppley virtually?
3) Flying out for the operation, does the patient spend the first night at the Eppley recovery facility?
A: In answer to your custom jawline implant questions:
1) The needed 3D CT scan is obtained locally.
2) All implant design sessiosn are done in a virtual manner. Patients only come here one time for the surgery.
3) Most patients spend the first night after surgery in the surgery center.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve scheduled a consultation, but just wanted to get some input before.
1) Can a sliding genioplasty and custom wrap around implant be done in the same surgery?
2) I have an implant that adds 6mm of horizontal lengthening, can the custom jawline wrap add extra mms to this? Or will there be too much strain on the face? Will there be too much strain if the custom implant also adds width and squareness to the face?
3) From rough measurements I would guess I would need around 18mms in total of horizontal lengthening to achieve my goal, is this possible with the combined procedures?
4) What would be the approximate timeline/surgery date, assuming a 3D scan is provided by the initial consultation?
A: In answer to your questions:
1) A sliding genioplasty and jaw implants can be done during the same surgery and it is not uncommon to do so. It is done when the chin augmentation movement for the total jaw augmentation needed exceeds what the chin soft tissues can safely tolerate from an implant.
2) and 3) With a indwelling 6mm chin implant this has a tissue expander effect so a jawline implant that has greater than 6mms can be done. But if the goal is 18mm chin augmentation then an implant can not be used and it has to be a sliding genioplasty to get that much horizontal chin projection.
3) 3 to 4 months is the typical lead time from when the implant design process is initiated until it would be ready for surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in clavicle reduction surgery for shoulder narrowing. I’ve attached some photos for reference. Some additional possibly relevant information for my request for shoulder narrowing… my bideltoid measurement is somewhere between 18″-18.5″ and my biacromial is between 15.5″-16″. Ideally hoping to get my bideltoid closer to 17″.
A: Thank you for sending your pictures. I think it is realistic to go from an 18/18.5 inch (47cm) bideltoid distance down to a 17 inch (43 cm) bideltoid distance with clavicle reduction osteotomies.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, For a long time i have been very insecure about a few aspects of my jaw. For one i have quite a short vertical jaw (or lower third of the face ) length which looks bad compared to my forehead which is much longer. At first i had considered forehead reduction but I already have a very small face compared to my body and don’t wanna make it worse.)
So I really want a vertical lengthening of my jaw. BUT i do not want any implants. So I’ve browsed the internet for months now looking for a solution that uses just bone to fix my problem and I think I might have found a couple. But I don’t know if these are possible and if any surgeon will help me with them.
So I read alot online about it being possible the create a gap between two bones,and that bone would regenerate between the gap eventually filling in the gap, is this true? I’ve also read that in some instances a bone graft material can be used to fill in the gap which will eventually become normal bone, is that also true?
My ideas of what could possibly be done :
idea number 1 :
a cut alongside the entire jawline is made, below the important nerves, much like the cut in a full chinwing osteotomy, of which ive provided a picture, the cut off bone is then moved 5 to 10 mm vertically ( downwards ) and put together with screws and plates to hold it in that place, from here, either the bone would regenerate ( as seen in the second picture ive provided ), filling the gap, or perhaps bone graft material could be used. this should eventually leave me with a vertically longer jaw that is completely natural bone material.
idea number 2 :
starts off the same, a cut alongside the entire jawline, but instead of a clean horizontal cut, the cut is like the one done in standard jaw surgery, where they slide the jaw forwards if you have a receding lower jaw, in this cut, they cut the bone in a way that they can slide it outwards without there being an open space between the cut. could this cut also be performed vertically along the jawline? so that it can be slid downwards without it creating an opening between bone.
idea number 3 :
if none of the above is possible, could a distraction osteogenesis of any kind perhaps be performed? ( picture provided ) i assume this has never been done for vertical length gains before, as i cant seem to find any evidence of that, but would it be possible ?
even thought you can find alot on the internet, its very hard to know what is real and what not, and if real, how well known and used the techniques are. so i really wanted to ask a professional .
I really hope you can help me, because to be honest, i seem to get more and more anxious by the day about this topic. i know that in the end none of this means the end of the world. but it is affecting my life quite a bit. and has been for a couple of years now.
thank you very much for your time! i hope to hear from you.
A: The only two viable options you have are a chin wing osteotomy, which is only going to get 5 to 6mms vertical lengthening or a vertical lengthening chin osteotomy which can easily get 10mms. Ideas # 2 and #3 (distraction osteogenesis) are not viable aesthetic options for a variety of reasons.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m looking to get my genioplasty plates removed from a procedure two years ago. However this would be my 4th procedure on my chin. For a timeline , 2 years ago I had a genioplasty with a chin implant placed at the same time. After my procedure I had hardware failure so after a month the surgeon went back in and plated everything properly, however after two months the chin implant got infected and had to be removed. Making in total 3 operations on my chin. I’m hoping to get plate removal in the hope to resolve some tightness and what I feel to be inflammation from the plates. I also have a concern as one of my plates goes beyond the lower mandible border. One of my major concerns however is the mentalis muscle, I am worried as I’ve had three operations already that my mentalis must be traumatized , would having to cut through a 4th time pose a risk. However I really would like to have these plates removed. My surgeon has refused saying there is no need, and I hear you are one of the best.
A: By your own description you appear set on having your chin hardware removed so I am not sure in that intent what difference it will make in terms of the mentalis muscle sustaining more surgical trauma.
What I can say that is useful is that I have seen many patients that come to me after a genioplasty done elsewhere who have had tightness and their surgeon removed their hardware to relieve it…and not a single one has developed an improvement in their chin tightness symptoms. This does not surprise me since hardware would not cause tightness…it is merely an easily identified potential cause because it is an implant. The reality is it is a soft tissue deficiency problem that is often not diagnosed whose cause, in your case, is multiple surgeries. You simply can’t cut through the attachment of the mentalis muscle numerous times and expect their to be no soft tissue ramifications from it. Incisions are not zippers, there is no opening and closing them repeatedly without consequences.
While you can have your hardware removed, expecting improvement in your chin tightness symptoms in only going with a concomitant soft tissue management strategy. (dermal-fat grafting)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr Eppley, I have a question, I’m male and have very wide hips and I’m very insecure about it. On some anatomy pictures I saw that the widest width of your hips is caused by the outwards sticking bone part on the top of the leg bone where the leg bones connect to the pelvis. Can this bone perhaps be shaved down a bit on both sides making the hips just a little less wide? I’ll take any cm I can get it reduced. I couldn’t seem to find any purpose for this part of bone so i guess I can miss part of it.
I’d like to hear what you think.
A: If you are referring to the greater trochanter protrusion of the femur, then no as this extension of the femur can not reduced due to the large number of muscle and ligaments attachments which are important for leg movement. The part of the hip width that can be reduced is the most outer aspect of the iliac crest.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in clavicle lengthening surgery. I have a couple of questions:
1) I’ll be traveling from Europe and so will need to fit this around my work schedule. How long would I need to stay in America for the surgery and follow up care?
2) Is it possible to add deltoid implants at the same time as the clavicle lengthening to gain the maximum possible width?
3) If so, what would be the approximate cost of that procedure (clavicle lengthening + deltoid implants)?
4) Would the surgery be able to be done in late February or March of this year?
A: In answer to your clavicle lengthening questions:
1) How long you should stay here after the surgery depends ion whether you are coming by yourself or with someone. But as a general guideline one week should be enough.
2) Deltoid implants can be done at the same time as clavicle lengthening.
3) Getting on the operative schedule with such ‘short notice’ would not be possible in the next 1 to 2 months.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am writing to you because I am very sad as I had surgery on my chin but the result was not what I expected and now it is very hard. Due to a retruded chin and chin asymmetry, I entrusted myself to a maxillofacial surgeon and decided to insert a customized peek implant.
The implant (as you can see from the attachments) was designed with 14mm forward projection and only 1mm in height, although the height of the implant is almost insignificant my chin now appears much higher than before, perhaps it was my chin bone which was already very high before but being retuso it was not noticeable in height, now with the same height but with more forward projection an exaggeratedly long and heavy chin appears for my face.
Only 10 days have passed since the operation but the height is really too much to think that it will change a lot in the next few days, I have some questions:
1) The problem is due, as I suspect, to the length of my chin which is retracted but also very long, so bringing it forward with a prosthesis will it seem taller than before?
2) In case the problem is the length of my chin bone if I made a customized prosthesis that as it comes forward it rises and shortens in height would it be a feasible solution to make the chin less high or in this way my chin would look strange?
3) What would be the best solution to overhaul the chin so that it is shorter in height?
4) Being already sure that I will have to do a revision of the chin, how long is it best to wait before doing a new operation on the chin?
It’s hard to trust other surgeons now I only trust you, for this I really appreciate your opinion
A: In answer to your chin implant revision questions:
1) The first thing to realize is that you are early in the recovery process and have a lot of swelling. You are not even 50% of the way into the recovery process. So I would expect at just 10 days after surgery to have a lot of swelling and tissue distortions…which are not representative of what the outcome may be. You also have to realize that this is a very large chin implant, way beyond what most patients get, so the swelling and tissue firmness/distortions will be extreme. I never judge the outcome of any chin surgery until at least 6 weeks after surgery. This is the minimum time to make even a preliminary judgement.
2) It is likely the soft tissue chin pad is riding high, besides the swelling, is because a 14mm implant creates a large implant mound to try and get the soft tissue chin pad to be able to be pulled over it during closure. Quite frankly I would never try toput in a chin implant over 10mms unless the patient had an indwelling chin implant to help stretch out the soft tissue chin pad first. Given your initial significant chin deficiency I don’t think a chin implant of this size was a wise choice. When you want this much horizontal chin movement this is the role of the sliding genioplasty where these soft tissue chin problems do not occur.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m not familiar with much of plastic surgery vocabulary but what I’d like is for my face to look years younger.
From what I can see, there is volume loss, and loose skin (including double chin, there is barely any fat under the chin but still looks like double chin).
I am scared of fillers because they need to be refreshed every few months and overtime give you a puffy look. I’m also scared of RF Microneedling or Ultrasounds because they have melted face-fat for many people based on pictures I’ve seen.
A mini facelift (for MEN) before/after picture seems like it can reverse aging significantly and does not require repeat visits every few months.
But please analyze my pictures and let me know what you think is the safest and best procedure and cost.
I’ve attached a picture from low-angle too.
A: If the goal is to improve the double chin and lax skin along the jawline, and that is what you feel will make you look year younger, then you are correct in that only a lower facelift will most effectively create that change. This is not what fillers are used for anyway and any non-surgical treatments (like RF) pale in comparison to their results of that of a surgical lower facelift.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello id like to get my chin and jaw /cheek / midface implants. i want to know the cost range please let me know.
A: Just based on a description alone it is impossible to say what type of facial implants you would benefit by having. (what areas, standard vs custom) Thus trying to provide accurate costs is not possible. The way to make that determination is to first get some pictures for my assessment and imaging and a description of your concerns and goals. Once that is determined then accurate costs can be provided.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I may have asked this question in my consultation, but is osteotomy not possible for the infraobital area? I think you had stated not,even with the orthognathic surgeries I brought up, which is why I am choosing implants.
I had a few reasonable questions about the long term survival outcome of the implants however – Do they become absorbed by the facial bone over time? What is their material? Most importantly, how do they react to the aging process, (e.g. osteoclast cells/ bone reabsorption) into old age? Just want to know if they will last all the way to grave (given what we know from the long span of time they’ve performed these). Thanks for answering.
A: In answer to your infraorbital-malar augmentation questions:
1) There are no infraorbital osteotomy techniques for augmentation, there are only implants.
2) Implants are structurally stable, they can not change form or degrade over time. They only change physical form at 375 degrees F. Your tissues may change around them as you age, which would be expected, but the implants themselves do not.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi I’m a 28 year old Asian male. I have a concave midface, and I’m interested in what you’ve described as a midface mask implant. Not sure if that changes the nose, would rhinoplasty be needed? Also what is the recovery like?
A: In answer to your midface mask implant questions:
1) Unless there is a reason to be having a rhinoplasty independent of the midface mask iimplant, there is no reason to undergo one because of it.
2) Recovery is largely about swelling and some numbness which is probably close to the same or perhaps less than a LeFort I osteotomy.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, can a secondary “jowl tuck” lift (for incipient jows and neck skin laxity) and secondary upper bleph (for slight recurring skin laxity) be done under sedation by intramuscular (not IV) midazolam? Might IM sedation be comparable, or preferable, to IV sedation in efficacy and/or safety? Original procedures, 16 years prior, under IV sedation, were: SMAS lift (w/retrotragal incision), platysmaplasty (submental incision), upper and lower (subconj) blepharoplaties.
Thank you for feedback.
A: I am sure someone may try to tackle that type of secondary upper blepharoplasties and jowl tuckup under this ‘modified’ sedation approach…it just wouldn’t be the way I would feel comfortable doing it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, For hip augmentation surgery for hip dips for fuller looking hips would you be able to use a standard buttock implant small one so I could have curvier hips? Please do let me know thanks
A: The question is not whether you can take a small buttock implant and place it in the hip dips….as you can. The real question whether it would have a smooth look and blend in to not look like there is an implant bump there. That has been my experience in doing so. It seems like the implant has a good shape until the swelling goes down and the soft tissue shrink down around it and then instead of a dip there is now a bump.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can you do the intramedullary instead of plates and screws for fixation of clavicle reduction osteotomies? (shoulder reduction)
A:In regards to the intramedullary nail my research indicates that, while it works for fractures that have an established length, if one is trying to shorten or lengthen the clavicles it may not be very stable at length retention. Knowing how hard it is physically to drive the shoulders in to get the outer half of the clavicle to meet the inner half when a bone segment is removed, it would be suspect that it could maintain keeping the two segments together. It would work if the two bone ends freely laid together without much tension (as in a normal fracture) but the shoulder girdle is both heavy and powerful. As a result, a single intramedullary may look good on the operative stable but its true effectiveness is what happens between the two bone ends after surgery when continuous tension is applied to it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I want to get botox in the forehead and eye area. Is there a risk that my custom infraorbital malar implants you inserted last summer can get infected if the injections happens around the area where the implant is?
A:Those injections are above the level of the IOM implants so no they should not get infected. I would just have them be cautious by the side of the eye where the implant is close to the injection site…although the orbicularis muscle (target of the Botox injections) is much more superficial than the implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, i had a chin shield type of genioplasty done approximately 8 months ago. This specialized cut made my face a bit more on a feminine side (34 year old male) , the cut still left both side of my chin deficient in horizontal forward and it did not achieve my desired goals which are broader chin and forward projection past my lower lips. I also noticed that my lower lip was also rolled in a tiny bit post procedure. Would it be possible for you to perform a revision genioplasty with this type of cut to accomplish a more masculine chin with more masculine chin with more forward projection? Based on the photos and x-rays, how many mm would you recommend for both horizontal and vertical ?
A: That type of chin osteotomy is designed to make the chin more narrow not wider. So your chin narrowing result is no surprise. Once this type of chin osteotomy is done the ability to secondarily redo it with a more horizontal osteotomy pattern, which would help make it wider, is lost. All that can be done now is to design a custom chin implant that would fit over and around the bone to create your desired chin shape change.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, One leg is bigger than the other in width, can i get them equal??
A: You can get closer but never equally equal with a calf implant and fat grafting. That appears to be a classic clubfoot calf which means the muscle is both smaller and the soft tissues very tight. The best result is going to come from a two stage approach, first stage fat injection grafting to stretch and soften the tight soft tissues and a second stage calf implant to augment the deficient muscle.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in making my side profile more forwardly grown overall, specifically in my middle and lower third region (maxilla and mandible) because they look flat. Does the midface mask implant push out the upper maxilla and the lower maxilla? Last but not least, I was wondering if the midface mask implant had a similar effect the infraorbital rim implants do to the eye area.
A: As you likely know your two options for moving your lower 2/3s of your face forward are either bimax double jaw surgery or overlay camouflage implants. Each has their advantages and disadvantages. But to answer your specific midface questions:
1) A midface implant pushed out the entire midface with the exception of the dentoalveilar area. (in other words the front teeth and upper lip vermilion would not change.
2) The midface mask covers all area of the midface and it can be designed to do whatever one wants to do including an IOM (infraorbital-malar) augmentation effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon