Your Questions
Your Questions
Q: Dr. Eppley, To what degree can infraorbital implants affect the shape of the lower eyelid? My lower lid is just a touch of roundness to it with the inferior sclera visible to a small degree.
Can a custom infraorbital implants create a narrower eye with a more angular lower eyelid?
A: There is no question that custom infraorbital-malar implants can help drive up the lower eyelid level. Whether that is enough on its own to create a ‘more angular lower eyelid’ depends on the current shape of your eyelids. Most likely it would require some eye inner adjustment as well.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a low set brow ridge that conceals most of my upper eyelid. Even so, it leaves a small semicircular sliver of the upper eyelid exposed. Is it possible to use fillers to conceal this portion of upper eyelid and create a more straight and angular looking upper eye in the process?
A: The best way to know if upper eyelid filler can be effective at reducing the upper eyelid show is to have it done. With an HA filler if it is not as successful as one would like it can always be reversed or let resorb over time on its own. I believe it will help conceal the upper eyelid bit whether it creates a straight or angular looking upper eye is not as clear.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in learning about forehead reduction via forehead bossing and a procedure that can flatten spots on the top of my head from Dr. Eppley:
Could these two procedures and temporal reduction be safely done together?
What would be the individual and total cost of these three procedures?
Are there any video recordings of these procedures? If so, is there anyway that I can view and show these videos to family members?
Could Dr. Eppley please explain or link a recent article about the full operation of these two procedures?
Are there any risks associated with any of these procedures? If so, what is the probability of these risks?
What is the typical duration of recovery from these procedures?
Have prior patients experienced any problems occurring weeks, months and years after surgery?
A: In answer to your skull reshaping questions:
1) Forehead bossing and skull reduction can be done together with temporal reduction surgery.
2) My assistant Camille will pass along that information to you.
3) I am not aware that I have ever shot any videos of these surgeries.
4) Any information on any of these procedures can be found by going to the following: www.exploreplasticsurgery.com and placed in the search box on the hope page the specific procedure name. It will pull up any articles and case reports I have written on the searched topics.
5) Any skull reshaping procedure has the set of risks which vary based on the type of skull reshaping procedure being performed….incision/scar, contour irregularities/asymmetry and over/unercorrection.
6) Recovery from any skull reshaping procedure is largely that of swelling of which the worst of it has usually past by 10 to 14 days after surgery.
7) Other than some minor aesthetic issues I am to aware of any medical sequelae from these procedures.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hey so I’ve contacted before about clavicle lengthening.. something I’m very interested in!! Now, I’m hoping to make the best out of one procedure… is it possible to lengthen each clavicle by 35-40mm? My shoulders are so narrow that they rest rolled over.. and from a cosmetic point of view, I’m hoping to look significantly broader!! Also, was wondering if it’s possible to inject renuva or radiesse into the hands to add volume and thickness to both the back and side of the palms, along with adding thickness to fingers!!
A: In answer to your clavicle lengthening questions:
1) Since clavicle lengthening is done by an interpositional bone graft, and not distraction osteogenesis, a distance of 30 or 40mms is too excessive. The distance of 20 to 25mms per side is more realistic is terms of an improved chance for more rapid and complete healing.
To get to 40mms it would take a combination of clavicle lengthening and deltoid implants.
2) Radiesse or fat are common injection materials for added volume to the back of the hands. Fingers are not injected because of the risk of vascular occlusion due to their tight tissues.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am extremely happy with the outcome of all the surgical procedure Dr. Eppley performed. I had no infections, no complications, and I am more than pleased with the results. I am running 5 miles per day with no pain or complications. I am happy with the professionalism and attention to detail provided by Dr. Eppley’s nurses and staff.
Everything went so well I now wish I had gotten even bigger implants:
-Now the skin has stretched out, would it be possible to upsize the implants?
-if so, how long would I have to wait until the next surgery?
-if so how big could I go?
 A: Given the natural stretch of the tissues that occur with time, you could graduate from your 6.5cm testicle implants to 7.5cm testicle implants. As long as you are six months out from the last surgery, your scrotum should be able to handle the additional 20% volume increase.
A: Given the natural stretch of the tissues that occur with time, you could graduate from your 6.5cm testicle implants to 7.5cm testicle implants. As long as you are six months out from the last surgery, your scrotum should be able to handle the additional 20% volume increase.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am writing to you seeking some advice about my teenage son. When he was a baby (approximately 6 months) we noticed the back of his head was flat. We took him to our family Dr and he said make sure you get him to sleep on his side and rotate him regularly. He also gave us a wedge to try to enforce the side sleeping. To make a very long story short, the little one refused to sleep on anything but his back and nothing we did, helped.
Today he regularly comments on his head shape and how much he hates it. He refuses to cut his hair short because it shows his head shape. I would greatly appreciate some information on the corrective procedure (prep, duration of surgery, recovery time, potential impact on his cycling and costs).
Thank you for your time and consideration.
A: Thank you for your detailed and heartfelt inquiry and detailing your son’s head shape concerns. By your description it appears he has a form of brachycephaly or a flat back of the head. The question is not whether the back of his head can be build out with the placement of a custom skull implant but how much augmentation does he needs to get him to a more self-confident state. I would need to see a side view picture of his head with the recognition that hair is a good camouflage of the extent of the problem. With hair the best way to get a good view of the extent of the flatness is to take a side view picture with his hair wet and combed down.
Once I see a picture of head profile I will do some imaging to convey what I think the placement of a custom skull implant can do. (without tissue expansion first) While a first stage scalp expansion always permits the greatest amount of augmentation there are obvious practical travel considerations that we need to consider.
The custom skull implant is made from a 3D CT scan of his skull. The surgery to place it is a 90 minute procedure under general anesthesia. Given his young age such patients usually stay overnite int the facility in most cases Recovery is mainly about swelling which may or may not make its ways into his face. Such swelling is usually resolved by about 10 days after surgery. Once recovered there are no physical restrictions as such a casual implant is really an inadvertent form of skull protection which can make it much harder to fracture (if not impossible) over the area that it covers.
Dr. Barry Eppley
Indianapols, Indiana
Q: Dr. Eppley, In one of your blog posts you state: “many models display a very strong or exaggerated brow bone appearance. It borders on being an almost angry appearance but is better anatomically described as an ultra low brow bone projection with near complete coverage of the upper eyelids. While I frequently get requests for such a brow bone augmentative change, I have to advise such requests that is almost always not possible. This is due to the fact the soft tissues of the eyebrows is very tight and can not be driven down below the existing brow bones unless these tissues have been first expanded before a brow bone implant is placed”
I assume what is meant by this is that lowering the solid prominence brow ridge is possible, but it will not move the eyebrows into a lower position, creating the angry looking appearance many patients desire.
Are you saying that it is rarely possible to create a lower set, bony prominence, or are you saying that it is rarely possible to get the eyebrows to move along with the prominence when creating a lower set brow ridge.
It seems like if a patient wanted to pursue a lower set brow ridge, without significantly moving the eyebrows, then the soft tissues of the brows would not be a limiting factor in that sort of augmentation.
A: Your understanding of the brow bone and eyebrow movement issues is correct. While brow bones can be augmented such that the inferior level of the supraorbital rim is lowered, and this is regularly done, there is no guarantee that the overlying eyebrows will follow down with it. At least not to the extent that some patients desire it to do so. But for the patient where downward movement of the eyebrows is not important, lowering the horizontal projecting level of the brow bones can be done.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m happy with the outcome and feel that you did a really good job with the overall look of the forehead. There’s still a somewhat noticeable protrusion on the right side of the forehead where the implant meets the skull unlike the left side which blends perfectly but it’s not something I’d want to undergo a corrective surgery for. I’m attaching some pictures for your files and did have a couple of questions to ask regarding some symptoms I’ve experienced following the surgery.
The first has been heavy hair fallout along the scar line, which you can see in the last two pictures. Is this normal to experience and if so, could I expect the lost hair grow back eventually?
The second have been sharp daily pains along my right temple and above my right brow. The pain usually doesn’t last very long but comes on strong and seemingly out of nowhere. It feels like a needle poking sensation. This happens maybe 3-5 times a day, and rubbing the forehead usually helps subside the pain. Is this a common occurrence 2+ months out and is it temporary?
A: In answer to your brow bone reduction recovery questions:
 1) Hair shedding is not atypical along the incisions line and is a reaction to the trauma of surgery. Some et very little while others get more. Shedding should not be confused with with hair loss or death of the follicles. I would expected most of the shafts that have been shed too exhibit regrowth which unfortunately is a slow process given the .1mm per day hair growth that occurs once the follicles reactivate. A helpful aid is to apply Rogainje along the incision line nightly. That can expedite the hair regeneration since that has largely a vascular enhancing (vasodilator) effect.
1) Hair shedding is not atypical along the incisions line and is a reaction to the trauma of surgery. Some et very little while others get more. Shedding should not be confused with with hair loss or death of the follicles. I would expected most of the shafts that have been shed too exhibit regrowth which unfortunately is a slow process given the .1mm per day hair growth that occurs once the follicles reactivate. A helpful aid is to apply Rogainje along the incision line nightly. That can expedite the hair regeneration since that has largely a vascular enhancing (vasodilator) effect.
 2) The dysesthetic nerve symptoms that youare feeling is undoubtedly related to the sensory nerves that are affected in brow bone reduction surgery, most commonly the supraorbital nerves which supply feeling to the forehead. As these nerves regain feeling they typically come back which a variety of abnormal sensations such as shooting pains, itchiness, etc. This is also why they feel better when you rub the forehead (like shaking your hand when you burn or hit it), it causes other story fibers to fire which over ride the and abnormal sensations. At the least I expect much more nerve recovery than you now which can take up to a year for maximum to full recovery…which many patients do experience. So yes at this point this is normal part of the recovery process.
2) The dysesthetic nerve symptoms that youare feeling is undoubtedly related to the sensory nerves that are affected in brow bone reduction surgery, most commonly the supraorbital nerves which supply feeling to the forehead. As these nerves regain feeling they typically come back which a variety of abnormal sensations such as shooting pains, itchiness, etc. This is also why they feel better when you rub the forehead (like shaking your hand when you burn or hit it), it causes other story fibers to fire which over ride the and abnormal sensations. At the least I expect much more nerve recovery than you now which can take up to a year for maximum to full recovery…which many patients do experience. So yes at this point this is normal part of the recovery process.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m interested in perioral lipo due to bulges around my mouth. I wondered why in your notes it says it should be continued to the jaw line? Surely for a man removing fat from the Sulcus and jawline will be aging and weaken the jaw? It seems most people beyond a certain age are having volume added to this exact area to improve the jawline.
A: While the line of perioral liposuction access can be all the way back the jaw angle, that doesn’t mean it needs to be. It all depends on each patient;s aesthetic desires. Most people that have buccal lipectomies and perioral liposuction do so for a complete cheek concats effect which enhances the cheeks and jawline. But for the patient with just true perioral mounds that is not necessary.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, How can I lower my brows? Can brow bone reduction help? I found them too high on the face, not close enough to my eyes! Is eyebrow lowering possible?
Thanks
A: I am not aware of a 100% reliable method for eyebrow lowering. Brow bone reduction topically does not cause the eyebrows to ‘fall’ or lower even in large brow bone reductions. Eyebrows maintain their position because of the length of the forehead skin/soft tissue rather than the bone structure underneath it. Tissue expansion of the forehead skin could be done and the the eyebrows released from the brow bones secondarily to attempt to have drop them down, thus creating more forehead skin. This makes theoretical/anatomic sense but I can to speak to its clinical effectiveness as I have never have forehead tissue expansion for this aesthetic purpose…even though you are to the first person got have asked me about it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Will the soft tissues slid around over silicone facial implants since the tissue do not adhere to them? I am worried that my soft tissues will move around and fall off the implants and look funny if there is no direct tissue adherence to them.
A: While the overlying soft tissues do not directly adhere to the silicone facial implant’s surface (unless perfusion holes are placed in them which is why I almost always do them), a firm capsule of scar develops around a silicone facial implant to which the overlying soft tissues are attached. Thus the importance of soft tissues adhering directly to the implant is really overstated/unnecessary and why soft tissues do not slide around over even a silicone implant. It is all about the biology of the capsular formation and understanding what it does.
The answer to this question is actually also known using another far more commonly done and familiar silicone implant, breast implants. While breast implants are not solid implants the encapsulation process keeps the soft tissue from moving excessively over and around the implants. This makes the implant feel like it is integrated or adhered to the soft tissues.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, When using tissue expanders and brow bone implants to lower the prominence of the brow ridge and eyebrows, what degree of control do you have over the shape of the eyebrows?
If a person wanted a lower, straighter brow ridge, with lower straighter eyebrows to match, would that be achievable using implants and tissue expanders?
A: In the design of custom brow bone implants one has complete control of the shape of the bone bones. However, how the soft tissues respond to tissue expansion and the driving force of the implant can not be as precisely predicted. To no surprise hard tissue augmentation is more predictable than the response of the overlying soft tissues
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Quisiera saber donde ubico la clinica, como es el procedimiento para una rinoplastia, cuanto es el tiempo de recuperacion. Y el aproximado de el costo. Gracias
A: En respuesta a sus preguntas sobre rinoplastia:
- Mi práctica se encuentra en Carmel, Indiana, EE. UU.
- Mi asistente Camille pasará el costo aproximado de la cirugía de rinoplastia. Un costo exacto requeriría una evaluación de imágenes de su nariz.
- 3) La cirugía de rinoplastia se realiza bajo anestesia general en mi centro de cirugía de forma ambulatoria.
- La recuperación de la cirugía de rinoplastia demora una semana hasta que la férula nasal se desprenda, luego de lo cual la inflamación desaparece lentamente en los próximos meses.
Dr. Barry Eppley
Q: Dr. Eppley, I am interested in facial asymmetry surgery, specifically fixing my cheek asymmetry. I had a few syringes of Bellafill to try and help my cheek asymmetry but at the time I did not know surgery was an option. Most importantly the filler has not improved the problem even in the slightest. I visited the provider who performed the injections last week and asked him to remove the syringes in order for the CT scan to show my true facial structure. He informed me the only way to remove Bellafill is through surgery. I certainly hope this will not have a negative effect on the CT scan or the surgery..
Since this did not improve anything, can we still proceed with the surgery? I know eventually the Bellafill will wear off, and I am not sure how that would work with a cheek implant. I am a 99.9 percent sure the Bellafill did nothing to improve the asymmetry. Its only effect has been a slight bump in my cheek area
This is an important issue to address before I proceed with the CT scan and cust4om cheek implant surgery.
A: Having Bellafil in the tissues does not preclude you from having surgery, particularly since it had no external aesthetic effect. The material may be able to see seen on the CT scan but likely will not as the PMMA beads are translucent. We may be able to locate and colorize them as part of the implant design to see how they relate, if at all, to the implant design. Regardless I do not see it as any impediment for designing or placing a custom cheek implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a custom jaw wraparound implant placed in September but now when I flex my jaw, the masseter muscle bulges higher up than the gonial angle. Will it heal automatically? Do you offer any procedures that fix it?
A:You have masseter muscle dehiscence, also known as ‘implant reveal’, where the muscle has become disinserted and retracted up over the implant. While it causes no functional jaw movement issues it is an aesthetic deformity. This is a difficult problem for which there are no easy solutions. Repositioning the muscle back over the implant is the biologic approach but that is very difficult to do and requires an external neck incision to do so. Alternatively trying to fill in the soft tissue defect with injectable fillers, fat injections or subcutaneous implants are all camouflage options.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have been reading a lot about temporal implants. My temples have gotten deflated in the last few years and the sides of my skull are already narrow. During research, I am reading that doctors claim that temple implants usually show a “groove” on the side of the face with aging – therefore, they are noticeable in negative way. Is this true? Also, I read that infections are very common with these implants (especially skull). Finally, I have read that revisions are needed in a high % of patients. Is this true?
A: In answer to your temporal implants questions:
1) Today’s temporal implants are designed to be applied under the temporalis fascia in top of the muscle, thus implant edging is not seen. You are likely referring to what can happen when temporal implants are placed right under the skin…over time their outlines become apparent. This is why this historic pocket location is a poor choice.
2) Temporal implants, like all skull implants, have very low infection rates. So low that I have yet to see one.
3) Like all implants placed anywhere in the body, revisional surgery may be needed for size, position or asymmetry issues. But it is no greater for temporal implants than any other skull, face for body implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,I am a 25 year-old trans-woman. I’ve recently been shopping around for quotes for a breast augmentation as I have not had much growth over the years. I have also been following clavicle shortening over the past few years, as I have naturally broad shoulders and I believe it could help my case. Would these two surgeries be able to be preformed simultaneously?
A: Yes both breast augmentation and clavicle reduction surgeries would the able to be performed together. The real recovery is from the clavicle shortening and the breast augmentation doesn’t add much to the recovery.
Interestingly both breast augmentation and clavicle reduction surgery can be done in the same operative field. And also because of the visual closeness of the two anatomic areas one complements the effects of the other. (upper body feminization surgery)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’d like to ask some short questions about subnasal lip lifts and corner of mouth lifts if that’s ok – as these are relatively rare!
1. How many mm might we take off above the lip?
2. How many mm might we take off above the lip corners?
3. How many mm might we take off to the sides?
4. How many mm might my lips widen from the corner lift?
5. Can we do a corner lift without adjusting muscles (as I sing this is a concern)?
6. There will still be vermilion in the corners?
7, How often do you perform these surgeries?
8. Do you have any additional photos to send?
I very much do appreciate!
A: In answer to your lip surgery questions:
1) A a general rule one should never advance the upper ore than 1/4 to 1/3 of the total upper lip philtral length.
2) In corner of mouths lifts the usual amount of tissue excised is 5 to 7mms.
3) I assume when you say sides you means the sides of the upper lip which are done as a gradual taper tp the corners from the central li[p advancement area.
4) A corner of the mouth lift will usually widen the mouth as a result by 2 to 3mmw.
5) A wedge of orbicularis muscle always needs to be done with a corner of the mouth lift to help the result. There is no adverse functional issues with doing so.
6) By definition my technique in corner of the mouth lifts (the Pennant method) is a vermilion advancement so there is always vermilion in the corners afterwards.
7) I perform many types of lip surgeries such as these on a very regular basis.
8) To acquire further technical and pictorial information I would refer you to the website, www.exploreplasticsurgey.com and you place in the search box the terms of lip advancements and corner of mouth lifts where you will find lots of information I have written on these aesthetic lip surgery topics.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Would it be possible to, instead of reshaping the bone bone as you described it during our webcam consult, print some bio-compatible prosthetic and replace the bone with it entirely? If so, how much would a procedure like this cost? And if not, do you know of another surgeon who would consider performing the surgery?
All the best,
A: In answer to your brow bone reduction questions:
1) By definition brow bone reduction is frontal sinus surgery…meaning whatever is put back will be directly exposed to the frontal sinus cavity. (the brow bone is the cover for the frontal sinus) So the risk of infection would be quite high with a prosthetic material as opposed to replacing the removed bone with your own reshaped brow bones. It is not a question as to whether this can technically be done as it can. But it would be not be a good decision to do so.
 2) I have used computer-generated implant designs to create brow bone ‘reduction’ but in a more indirect method. For the male patient who can not have the incision required for brow bone reduction surgery because of scar concerns, implants can be designed to sit in the supra brow bone break to smooth out the sharp transition from the prominent brow bone into the forehead. This is a more prudent and safer use of brow bone implants.
2) I have used computer-generated implant designs to create brow bone ‘reduction’ but in a more indirect method. For the male patient who can not have the incision required for brow bone reduction surgery because of scar concerns, implants can be designed to sit in the supra brow bone break to smooth out the sharp transition from the prominent brow bone into the forehead. This is a more prudent and safer use of brow bone implants.
Dr. Eppley
Q: Dr. Eppley, I understand everything you said about the correction of my chin ptosis (Witch’s chin) and agree with it. However, I really do not wish to have a submental incision. I also really think I only have a problem with the right side of mentalis muscle. It just needs to be resuspended with anchors is what I really think. It is also the reason for my off centered lip ptosis and chin ptosis on the right. Would it be possible to resuspend the muscle via anchors on the right side, intraorally?
After googling so much about my problem, I stumbled upon a girl who had the same problem as mine, deviated lip and ptosis on right side and she went and resuspended her muscle and centered her lip with three anchors and it fixed her problem completely.
A: While I am happy to do a mentalis muscle/chin pad resuspension and avoiding the submental incision is understandable, I have a lot of experience with that procedure to which I say the following. For every one successful case of mentalis muscle resuspension I can show you ten cases that did not work out as well. It is not a highly successful procedure on every patient. It is most successful when a chin implant is used (with high tissue adherence material like Medpor or ePTFE) at the same time to give the chin pad something to grab onto and hold it. (which is exactly what you don’t need) But by itself it is often an underwhelming procedure, particularly in the face of a real chin pad excess and not pure ptosis alone.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have some questions about caudal sep[toplasty> Is this basically a deviated septum repair? While I didnt originally intetend to ask about repairing a deviated septum, I think Dr. Eppley identified an issue I’ve long had. We discussed that it should bring symmetry to my nostrils, but will this procedure also help breathing? He said he couldnt diagnosis accurately until I was there, but what are the risks? I’ve read some realself reviews septoplasty can have negative effects on the appearance of the nose tip, but others say it improved that.
A: In answer to your caudal septoplasty questions:
1) A caudal septoplasty is a limited form of septoplasty that only address the end of the septal deviation behind the columella of the nasal tip.
2) Generally a caudal septoplasty is more about removing the obstruction in the visible nostril area and improving nostril asymmetry than about improving breathing.
3) It usually does not have any effect, positive or negative, on the shape of the nasal tip…unless the caudal septal deflection is very large.
4) You are correct in that only dissolvable sutures are used.
Dr. Barry Eppley
Indianapolis, Indiana
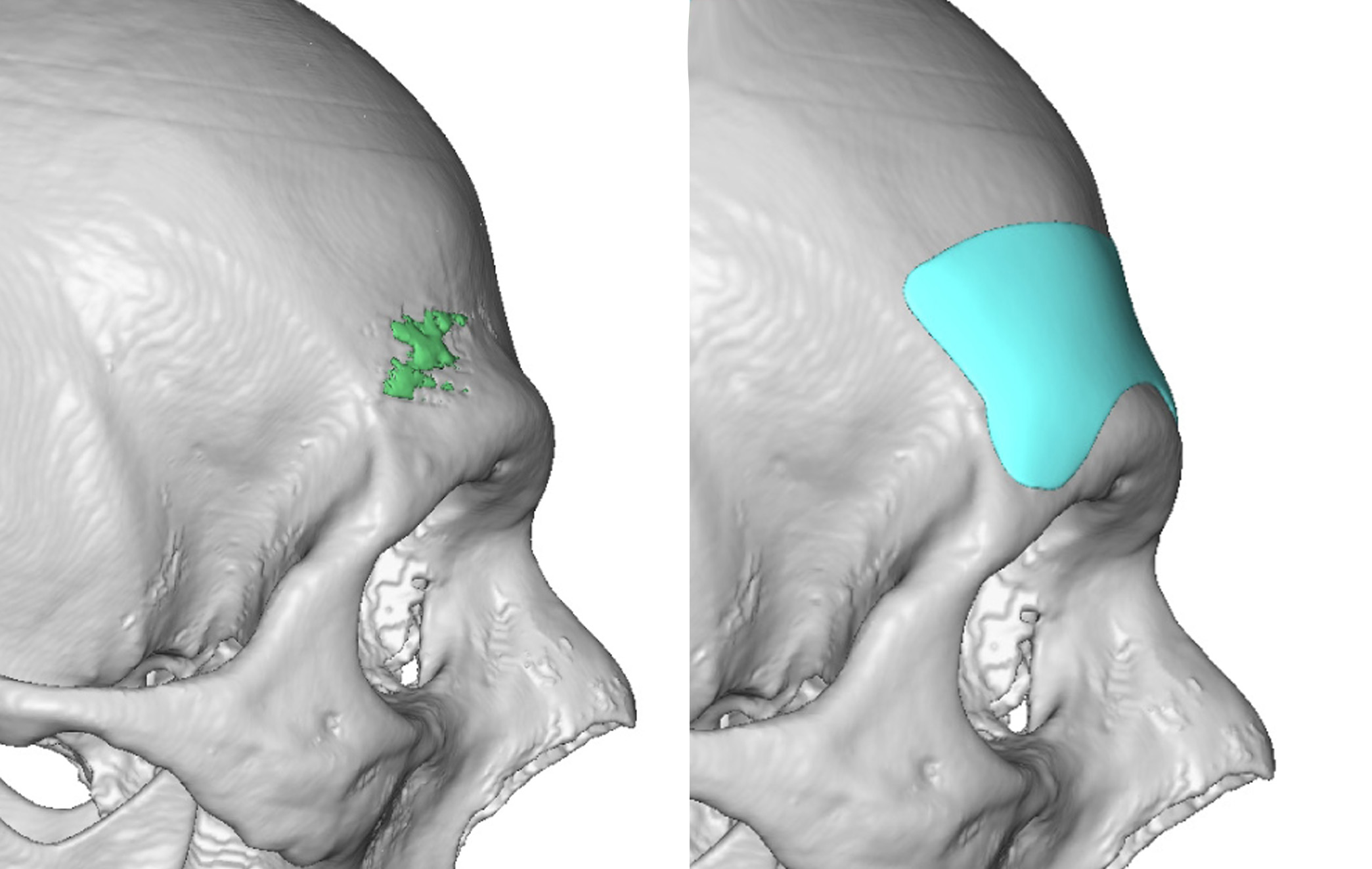
Q: Dr. Eppley, I am interested in forehead reshaping? I’m very unhappy with the ridges & bumps on my forehead. On a side profile view, it looks very straight and doesn’t have a pretty feminine curve. What are your recommendations for improvement?
A:Thank you for your inquiry and sending your forehead pictures. You have four prominent forehead bumps, the paired medial brow bones and the upper paired forehead horns. Normally those would be reduced to eliminate them but that is counterproductive in them presence of a non-curved forehead profile. Thus the forehead reshaping concept of covering over these bumps to create a more feminine curves to the forehead would achieve both forehead reshaping aims. The only debate is whether this should be done using a custom forehead implant with a more limited scalp incisional approach or to use bone cement with a more open scalp incisional approach.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, my head is narrow at the sides, it lacks height and the shape of the skull is smaller. The back is flat with no volume. No overall roundness or volume. I would like my narrow volumeless and small forehead to be more masculine, what’s your outlook on it? What procedure is the best in my case?
Goals: Skull 💀 Taller head, wide at side, Round back of the head sticking out, overall round with volume.
A: The key questions in any skull augmentation patient are; 1) What are the zones of the skull that need to be covered (there are 5 – forehead, top, back and sides(2)) and 2) with how much volume for each area? (the maximum immediate volume that can be placed is 150ccs) While on the computer any extent and size of custom skull implant can be designed, that does not mean it can be successfully placed given the constraints of the tightness of the overlying scalp. The basic principle is the more skull areas that are covered the less each area can be in thickness due to the flexibility of the scalp. This is why in larger surface area skull implant coverages or in subtotal skull implants that are fairly thick, a first stage scalp expansion must be done.
Given some of the examples of skull implant designs you have shown and in your side view drawing these suggest that you would require a first stage scalp expansion to come close to your aesthetic goals.
To help you think about this clearly you need to answer and prioritize these questions:
1) What are the skull zones that need to be covered and what is their order of priority? You have really described a total overage skull implant of all zones.
2) Can you sacrifice implant volumes to avoid a first stage scalp expansion.
Dr. Barry Eppley
Indianapolis, Indian
Q: Dr. Eppley, I want to know if a chin surgery is the solution for my case. I have a kind of small chin but is really protruding specially when I smile, I actually feel difficult to smile like I have to make a big effort with my chin muscles. Also I dislike the dimple on it, i would like you to help me.
A:Thank you for your inquiry and sending your pictures. While you have a smaller chin you also have a deeper labiomental fold and a central chin dimple. This suggests tight musculature which is why it feels difficult to smile. While your smaller chin can be slightly augmented my concern would be whether that would make your smiling issue even more difficult. Thus I am uncertain whether chin augmentation for you is worth that risk. You could, of course, treat the chin dimple by fat injections.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, In references to the challenges of lowering the male brow ridge to create an ultra low brow common among male models, you stated “the soft tissues of the eyebrows is very tight and can not be driven down below the existing brow bones unless these tissues have been first expanded before a brow bone implant is placed.”
Is undergoing tissue expansion before any implants are added likely to make that sort of look a reasonable possibility, or would it still be impossible in most cases?
What I’m trying to determine is if achieving the combination of a low bony ridge brow ridge/low eyebrows—the “angry” look, so to speak—is simply a matter of expanding tissues before the implant is placed, or if tissue expansion preceding brow bone lowering is something of a “pie in the sky” procedure that may work in some cases, but on the whole has a highly uncertain outcome.
A: As I have previously written the eyebrows can only be significantly lowered if ‘excess’ soft tissue is first created. (soft tissue expansion) A brow bone implant will not usually do not alone. The concept of soft tissue expansion is not a theory, its use has a long history in plastic surgery of which eyebrow expansion/lowering would just be another example.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, In one of your blog posts you state: “many models display a very strong or exaggerated brow bone appearance. It borders on being an almost angry appearance but is better anatomically described as an ultra low brow bone projection with near complete coverage of the upper eyelids. While I frequently get requests for such a brow bone augmentative change, I have to advise such requests that is almost always not possible. This is due to the fact the soft tissues of the eyebrows is very tight and can not be driven down below the existing brow bones unless these tissues have been first expanded before a brow bone implant is placed”
I assume what is meant by this is that lowering the solid prominence brow ridge is possible, but it will not move the eyebrows into a lower position, creating the angry looking appearance many patients desire.
Are you saying that it is rarely possible to create a lower set, bony prominence, or are you saying that it is rarely possible to get the eyebrows to move along with the prominence when creating a lower set brow ridge.
It seems like if a patient wanted to pursue a lower set brow ridge, without significantly moving the eyebrows, then the soft tissues of the brows would not be a limiting factor in that sort of augmentation.
A: Your understanding of the brow bone and eyebrow movement issues is correct. While brow bones can be augmented such that the inferior level of the supraorbital rim is lowered, and this is regularly done, there is no guarantee that the overlying eyebrows will follow down with it. At least not to the extent that some patients desire it to do so. But for the patient where downward movement of the eyebrows is not important, lowering the horizontal projecting level of the brow bones can be done.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am writing to you seeking some advice about my 17 year old son. When he was a baby (approximately 6 months) we noticed the back of his head was flat. We took him to our family Dr and he said make sure you get him to sleep on his side and rotate him regularly. He also gave us a wedge to try to enforce the side sleeping. To make a very long story short, the little refused to sleep on anything but his back and nothing we did, helped.
Now as a teenager his head shape bitters him a great deal. He does lack some confidence and is continually commenting on his head shape and how much he hates it. He refuses to cut his hair short because it shows his head shape. I would greatly appreciate some information on this procedure (prep, duration of surgery, recovery time, potential impact on his cycling and costs)
Thank you for your time and consideration.
A: Thank you for your detailed inquiry and detailing your son’s head shape concerns. By your description it appears he has a form of brachycephaly or a flat back of the head. The question is not whether the back of his head can be build out with the placement of a custom skull implant but how much augmentation does he needs to get him to a more self-confident state. I would need to see a side view picture of his head with the recognition that hair is a good camouflage of the extent of the problem. With hair the best way to get a good view of the extent of the flatness is to take a side view picture with his hair wet and combed down.
Once I see a picture of head profile I will do some imaging to convey what I think the placement of a custom skull implant can do. (without tissue expansion first) While a first stage scalp expansion always permits the greatest amount of augmentation there are obvious practical travel considerations that we need to consider.
The custom skull implant is made from a 3D CT scan of his skull. The surgery to place it is a 90 minute procedure under general anesthesia. Given his young age such patients usually stay overnite int the facility in most cases Recovery is mainly about swelling which may or may not make its ways into his face. Such swelling is usually resolved by about 10 days after surgery. Once recovered there are no physical restrictions as such a casual implant is really an inadvertent form of skull protection which can make it much harder to fracture (if not impossible) over the area that it covers.
Dr. Barry Eppley
Indianapols, Indiana
Q: Dr. Eppley, I’ve just come across your Instagram and I’m interested in getting my forehead reduced. It has troubled me all my life, it’s very protruding and I would love to get it reduced so it doesn’t stick out as much. Do you think it is possible for my forehead to look “normal”?
A:Thank you for your inquiry. The ability to reduce a forehead protrusion (forehead bossing) is based on the thickness of the frontal bone that makes up the forehead. Based on my extensive experience with forehead surgery I would predict that you could achieve the result illustrated in the attachment with forehead reduction reshaping. A preoperative x-ray would be needed to assess the thickness of your frontal bone and whether such result as illustrated is possible.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have small breasts and herniated nipples as well. I’ve been told implants alone would work but I’m thinking not. I had a tummy tuck a year ago and looking for a revision as well. I am small in size at 5’ 2” 105 pounds and I am wider in waist after the ummy tuck.
A: Thank you for your inquiry and sending your pictures from which I can make the following comments:
1) Your tummy tuck has some scar irregularities and dog ears at the ends as well as some residual thickness between the umbilicis and the scar line. I would recommend a tummy tuck revision with total scar revision with a little more skin removal as well as liposuction to thin out the residual fullness in the lower abdominal area and flank/waistline areas. I suspect that you did not have the waistline treated by liposuction, hence it now appears wider.
2) Your breasts are small tuberous breasts that have some sag. Implants alone would help considerablly and would be the foundation of their ‘reconstruction’ with periareolar reduction/release for the nipples. I would probably consider transaxillary implant placement and not use the periareolar areas as the pathway to place the implants.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I feel like a have short chin that lacks height. When I push my lower jaw forward and down it creates the chin augmentation effect that I am seeking. What are your recommendations?
A: I have reviewed your pictures and did some imaging to which I can make the following comments:
1) Your chin dimensional needs is largely vertical with slight horizontal, thus they sliding genioplasty (technically open wedge bony genioplasty) would be the preferred procedure.
2) During the bony genioplasty the vertical and horizontal bony gaps would be filled with allogeneic corticocancellous chip grafts (tissue bank bone), not only to fill the expectant bone gaps but also to help soften the labiomentao fold.
3) Submental/neck liposuction contouring would work well with the vertical chin lengthening for the best cervicomenta angle appearance but also would be a convenient fat source for concurrent fat injection grafting into the left chin soft tissue contour deformity from the prior vascular occlusion event.
Dr. Barry Eppley
Indianapolis, Indiana