Your Questions
Your Questions
Q: Dr. Eppley, I supposedly have a Peek chin implant, it does not project enough and is skewed pointing off to my left. I would like my chin to be symmetric with more outward projection. It was interesting that you wrote that the flesh adheres more readily to the Medpor implant as apposed to Peek, as I feel that this could/might also produce a better outcome (my bottom lip has no overhang anymore and when my mouth is relaxed all my lower teeth and gums show). Could you please tell me my options, thank you.
A: The outcome from any facial implant surgery, chin implants included, are based on the shape and size of the implant not its material composition. Material composition of an implant affects how it is inserted and removed but not its aesthetic outcome.
Thus when considering a new chin implant the key issue is the exact shape and dimensions of what lies in you now. Knowing the exact dimensions of what you have is invaluable information in how to design an implant with better dimensions for your needs. Any PEEK implant would have to be custom made and thus there would be an implant design file for it. I would need to know more about your existing chin implant. Your implanting surgeon should have this information.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in pectoral and testicle implants. Do I need custom implants or will standard implants work for both? How much does a testicle implant weigh?
A: Thank you for your inquiry and sending your pictures to which I can provide the following information:
PECTORAL IMPLANTS The key in pectoral implant selection is to have an understanding of the patient’s exact chest shape goals. Then the implant is selected by knowing the height and width measurements of the chest and the amount of projection and is location along the implant that the patient wants. This is how one knows whether a standard vs custom pectoral implant can most effectively achieve the desired outcome.
TESTICLE IMPLANTS Many of the testicle implants I do are in patients that seek enhancement of what they already have, not replacement of a missing testicle. Thus by definition these are almost always bigger in size than what standard testicle implants (max size 5.0cms) can achieve. Most custom testicle implants are in the 6.0 to 7.0cm size. (90 to 120cc volumes per each implant) The weight of a solid silicone testicle implant is completely controlled by its size. While size is obviously important the other major decision is the choice of the side by side vs wrap around implant technique. There are advantages and disadvantages with either approach.
Pectoral and testicle implants can be done during the same surgery.
For now I will initially assume you need standard pectoral and custom testicle implants with the wrap around technique. But this open to further discussion and at the least is a starting point of that discussion.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have another question which I think we may have covered during my consultation but I want to confirm…
I currently have and have always had low blood pressure. My last blood pressure reading was 90/70, but it sometimes goes lower. I want to confirm that temporal artery ligation is safe in my case and won’t cause problems such as dizziness, lightheadedness or more serious complications. I will also double check with my neurologist. The first time I checked with him he didn’t seem to think the procedure would be unsafe for me.
I very much want to have this procedure and hope there is nothing that will prevent me from doing so. I will probably have more questions that I forgot to ask Dr. Eppley during our consultation, but I think we covered most everything!
Thanks very much!
A: Low blood pressure is not a contraindication to temporal artery ligation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m looking for my cheeks to be more prominent and have a good Ogee curve? What should I do, giving the photos. What would you recommend?
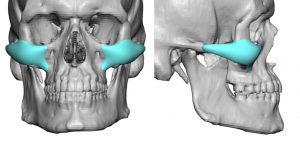 A: Thank you for your inquiry and sending your pictures. While the concept of ‘prominent cheeks’ in a male can have different interpretations, most commonly they seek a so called high cheekbone look which has a good Ogee curve. This can be seen in the attached custom cheek implant design.
A: Thank you for your inquiry and sending your pictures. While the concept of ‘prominent cheeks’ in a male can have different interpretations, most commonly they seek a so called high cheekbone look which has a good Ogee curve. This can be seen in the attached custom cheek implant design.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have some questions about skull reduction. The height of my skull bothers me and I want it reduced. I read your blog and three procedures got my attention: grid pattern skull reduction, occipital skull reduction and sagittal crest reduction and I have the following questions:
1. Are the occipital and sagittal crest procedures encompassed in the grid pattern skull procedure? If yes, then the first one is for someone who would like the entire skull to be reduced and the other two are for specific areas only?
2. Is the technique used for reduction in all three the same or different?
Thanks in advance.
A: In answer to your skull reduction questions:
1) Sagittal crest reduction is reducing linear line of bone while occipital reductions are usually done by a grid or sunray technique.
2) In the end any form of skull reduction is done by a burring technique. The pattern by which the reductions are done is just a method to ensure an even bone reduction across generally what is a curved surface.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a chin implant removal and a genioplasty about three years ago. I had the implant in for over 20 years. It was placed too high, but I really did not like how long, square and masculine my chin looked. The genioplasty took about 4.5mm in vertical height off and moved forward approx 3mm. I believe my surgeon did a good job as far as the bone went, but the tissue did not shrink down to the bone like he thought it would. It looks like my old chin, but deflated and it seems longer to me. The pocket from my old implant is dimpled and textured along with the soft tissue irregularity from my old chin shape. I have also lost feeling in my lower gums which I am assuming will be permanent considering the length of time since the surgery. It is very difficult to smile. If I smile really big, my chin juts out and looks longer and dished out. My lower lip is pulled in and now my lips are uneven and look crooked when I talk. The muscle feels constantly tight and uncomfortable. My surgeon has done botox and filler in my chin but I can’t keep doing that indefinitely. I am concerned he doesn’t know what to do about my situation. So that’s why I am writing to you. I have been reading your articles online looking for some answers. Thank you for taking the time to read this and look at my photos. If you have time, please let me know if there is a way to at least make it look better. Maybe then the loss of function would be more tolerable. Thank you.
A: Thank you for your inquiry and sending your pictures. When reductive chin procedures are done, whether by a primary chin reduction or an implant/genioplasty change, you have to be aware that the expanded soft tissue chin pad is never going to shrink down smoothly to a smaller bone support. This is a fundamental chin concept that many surgeons and patients frequently overlook.The naturally tighter already stretched out soft tissue chin pad will end up with exactly what has occurred in your case. When the mentalis muscle length shortens, scar/muscle contraction occurs and external contour irregularities will invariably occur.
This is a very difficult problem to try to improve and injectable strategies are the logical initial treatment strategies. There are surgical strategies to try and improve the situation with the concept that some of the problem comes from soft tissue excess. A submental tuck will certainly shorten its length and may or may not improve some of the contour irregularities. And it will probably provide improvement of the chin pad protrusion when you smile. However it is not clear that it would provide any improvement on lower lip symptoms such as tightness, asymmetry or pull down.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Your work is beautiful. I have a bone growing above my left eyebrow but not my right eyebrow. I am also having headaches concentrated only on the left eye. I am not sure if the 2 are associated. How much is the cost to have this bone shaved down? Also will the surgery help with the headaches as well? Thank you for your time.
A: Thank you for your inquiry and sending your picture. It would be a fair assumption that the enlarged brow bone and the location of headaches in the ‘same neighborhood’ is likely not coincidental given the location of the supraorbital nerve. Compression of the supraorbital nerve is a classic etiology for frontal migraines in some patients. Thus it would also be logical to assume that in reduction of the prominent brow bone, with concomitant supraorbital nerve decompression, that headache relief is possible.
Another important consideration is why the brow bone on that side is enlarged. While I have seen numerous patients with brow bone asymmetries they usually don’t have associated headaches. Thus this merits evaluation with a 2D CT scan to ensure that the brow bone enlargement is due to typical over aeration of the frontal sinus on that side and not from an actual bone overgrowth pathology. (e.g., osteoma, osteoid osteoma)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a young male who was born with hydrocephalus. My head size is almost 28 inches in circumference. Thankfully I have not had any complications of any sort in my teenage and adult life. But as you can imagine it has restricted me from certain activities. I cannot fit any helmets, hard hats or ball caps. I would like to get a standard head size so that I can wear proper headgear for safety.
A: Thank you for your inquiry and sending your pictures. The question you are asking is whether your skull can be reduced sufficiently to allow the activities you can not do now to be able to finally do. This comes down to whether the skull bone is thick enough in many different areas to be safely reduced. To definitively answer this key question requires a 3D CT scan in which the the various thicknesses of the skull can be measured
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m interested in the webbed neck surgery. Am I good candidate?
A: Thank you for your inquiry and sending your picture. Webbed necks like yours are the most difficult to get sustained neck reshaping results due to the tighter neck tissues that exist. A good preoperative test is the pinch test on the back of the neck/lower scalp. A certain amount of tissue stretch/flexibility must be present for the procedure to be successful. There is also the issue of scar visibility on the back of the neck in women with very short hairstyles that is a potential aesthetic concern. These two issues would have to be assessed to determine if this is a viable neck reshaping procedure for you.
Dr. Barry Eppley
Indianapolis, Indiana
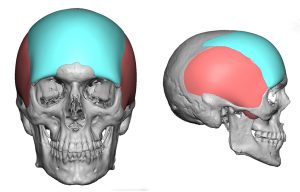 Q: Dr. Eppley, I was interested in the forehead widening procedure that Dr. Eppley performs as I have a very rounded narrow forehead and browridge and would like for them to be widened and advanced using implants.
Q: Dr. Eppley, I was interested in the forehead widening procedure that Dr. Eppley performs as I have a very rounded narrow forehead and browridge and would like for them to be widened and advanced using implants.
More specifically, I was interested in this specific model shown on the website. Also, is there a threshold for the amount of implant that can be squeezed in? I would require a fair bit of advancement so I’d like to know what the limits of such an implant are.
A: The limits of any skull implant is based on its volumetric expansion. As a general rule scalp stretch can accommodate up to 125 to 150ccs in most people. The specific forehead implant to which you refer is 86cc with a maximum thickness of 5mms.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello – I have Permalip implants along with some really tight scar tissue, so I was thinking of having them removed. Will removal eliminate the scar tissue? Or is the tissue not stuck to the implants since the implants are smooth?
A: Removal of your lip implants will not completely eliminate the scar tissue. The surrounding capsule of the implants will be left behind…which will shrink down over time but probably never 100% go away.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a sliding genioplasty lengthen 7mm down and advanced forward 8mm. I also had lipo under the chin and buccal fat removal. I now deeply regret my decision and am extremely unhappy with my end result which has given me an Over projected chin, a chin and jawline that do not match, decreased lower lip size, constant tightness and pain, a chin that is off to one side and a more aged appearance.
My surgeon is making me wait over a year before he will revise and wants me to decide on a full reversal or a partial revision (setback 4-5mm). This is the part I am unsure of, as I was happy with my face before. But with the complications associated with the changes in the soft tissue I am unsure how much to revert the chin by. I also do not understand why I have to wait so long before I can have the revision.
A: I can not answer the the timing decision made by your surgeon. My approach is that when the patient has identified an aesthetic dissatisfaction after the swelling has resolved then one can proceed with a revision. I would be cautious about complete sliding genioplasty reversal as they are now going to to be some softt tissue redundancy issues.
Dr. Barry Eppley
Indianapolis, Indiana
As A Female With A Wide Chin And Now Squarish Smile What Type of Chin Implant Replacement Do I Need?
Q: Dr. Eppley, I think as a female my current chin implant is a bit wide (smile is squarish). What type of chin implant repalcement do I need?
A: Thank you for your inquiry and sending your picture. In regards to your chin implant:
1) When was the surgery done?
2) Was it an intraoral or submental incision placement?
3) What type of chin implant material was used?
4) What was the style and size of chin implant used?
Knowing this information is critical when deciding if a different chin implant may be better. It is also enormously valuable to know where on the bone the chin implant is actually placed which is why a cone beam or 3D CT scan of the chin would also be needed.
While your first chin implant was a guess as to what the outcome would be, we use the information that has been gained from the first surgery to make the second surgery (chin implant replacement) have a more predictable/desired aesthetic outcome.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello! I am very interested in the shoulder narrowing surgery since my shoulders are about 43-45 cm wide (not really sure). I should inform that I am a dancer and a big concern of mine would be that the surgery might constrict certain movements that require a lot of force. Would that be an issue? (Of course I mean after a healthy recovery).
A: Requesting shoulder narrowing surgery and being a dancer is a new combination for me. Having never seen his combination before I can not say with absolute certainty that it poses no long-term issues in regards to exposing one’s arms to a large range of motion with a lot of force. But it would be logical to assume that when one is fully healed (3 months) that would not be a problem since the bones would be fully consolidated and back to normal bone strength. While my current recommendation is that patients can return to all normal not highly strenuous activities in 6 weeks I would push that recommendation to 12 weeks in this more highly strenuous activity.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I wanted to ask a question regarding iliac crest reduction. I have a wide bony iliac crest (photo attached) and as a man, it kinda bothers me. You are the only surgeon I could find online that does iliac crest reduction. I was wondering do you have any before and after photos to see how much of an iliac crest actually gets removed? From my understanding, just a little, and I’m not sure if it’s worth it to go through a procedure.
A: Thank you for your inquiry and sending your picture. I believe you are referring to the two anterior points of the iliac crest known as the anterior superior iliac crest points. (see attached) They could be reduced by a small 3 cm incision over them. Ironically those who have the least prominences benefit the most. (meaning get complete reduction)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, These are the two procedures I was hoping to discuss:
1) Buccal fat pad removal with perioral liposuction to get a more defined jaw line and decrease my chubby cheeks. I’ve had chubby cheeks my entire life and I was hoping as I got older they’d get smaller. They have a bit – but not to the extent that everyone was telling me they would. At complete rest it doesn’t look as chubby anymore but the moment I smile even a little or talk – they return.
I’m not worried about the potential effects of buccal lipectomy that can happen when 20-25 years down the line. I feel like when I’m 60 I’ll address the issue then and I’d rather not be so self conscious and have the jaw line I want now rather than worrying about what’s gonna happen when I’m 60.
I’ve attached pics below showing me at rest and laughing.
2) Upper lip lift. I don’t want the size of my lips to change because I do think they’re proportional to my face. But, I’m to achieve two things:
1) to show more of my upper teeth (I think this will also ensure I don’t smile “so big” therefore reducing the chubby cheek effect when I’m laughing 🙂
2) since birth I’ve had an extra layer of skin located under my nose (I’ve attached a pic below). At rest it’s not overly noticeable, when I talk, you can somewhat see it. The pic I’ve attached is me prominently protruding it. As a child a surgeon suggested I have it removed but my parents were worried it would leave a mark/scar and that’s really been the only thing that’s stopped me from getting it taken off. I happen to come across your work on a message board and would like to discuss whether he thinks a bullhorn lip lift would ensure that this layer of skin is taken off.
Thanks so much,
A: Thank you for your inquiry to which I can say the following:
1) The buccal lipectomy/perioral liposuction procedure is straightforward so I don’t have any new insights into them.
2) By definition it is not possible to do a subnasal lip lift and not change the size of the upper lip…unless that subnasal lip lift is 3mms or less. If one only wants to show more upper teeth a smile line reduction (mucosal excision along the lower border of the lip) is the procedure to do so. This will, however, make the upper lip look a bit smaller.
3) If there is a roll of extra skin right under the nose of the upper lip, a subnasal excision would be effective. I did not see an attached picture showing this roll so I don’t know exactly where it is or how big it is.
4) The combination of a subnasal excision and a smile line reduction would cancel each other out in terms of lip size….but would improve tooth show and reduce/eliminate the subnasal roll.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Back in 2017, a surgeon convinced me to get a chin implant alongside a rhinoplasty to give me a better profile and to relax my strained mentalis muscle.
The implant felt tight and worsened my strain, giving me a pebble chin so I had it removed in 2019.
My chin sagged in the worst way and I couldn’t close my mouth naturally without forcing and making my chin ball up.
Another surgeon told me that it was scar tissue and advised me not to touch just massage and let it heal by its own, but I didn’t listen to him and went to another surgeon who performed a sliding genioplasty on my chins months ago (9mm horizontal advancement and 2mm vertical) to stretch the tissues.
It semi worked as it reduced the ptosis and I’m now able to close my mouth more naturally, but as you can see on the pictures, the ptosis is still there and not totally fixed.
I still feel like I have to force my lips together a bit and I sleep with my mouth open. I also get spasms and random contraction around my mouth. It’s like the muscles are trying to move by their own.
Do you think that you can help me? I’m very depressed.
A: Thank you for the additional information. Your case is a tough one as having had two prior surgeries you really don’t want to have a third…unless there is great assurance that it will actually make you better. With your still very short chin and having gotten some improvement from the prior sliding genioplasty (not sure why any vertical was ever added as you need to drive the chin forward as much as possible) it is certainly tempting to think that doubling your forward chin projection (out to 16 to18mms) would help even further. But to know if that is even possible would require either a lateral cephalometric x-ray (maybe your surgeon did it after surgery) or a cone beam scan of your chin.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to know if I am a good candidate for frontal bossing shaving and hairline lowering. I understand you may not be able to make my forehead flat but I was hoping that shaving it down a little and pairing that with hairline lowering could make a difference for me.
A: Thank you for your inquiry and sending your pictures. You are correct is that te frontal bossing can not be completely reduced and that a hairline advancement will help reduce some of the frontal bossing appearance. Both procedures are synergestic to each other…particularly the hairline advancement to the frontal bossing.
The key question now is what amount of hairline advancement do you need and would that amount be realistic. To help answer that question you would need to draw on your forehead or on the actual picture where you would want the hairline advanced.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had the tricep implants in the attached photos 3 years ago (subfascial) and I have not had a chance to change them yet- unfortunately the margins can be seen.
I’ve been reading one of your articles on tricep implants- https://exploreplasticsurgery.com/technical-strategies-triceps-implants/?doing_wp_cron=1619401676.5458180904388427734375
As it says in the article, the implants are placed sub-fascial (underneath the fascia, but above the muscle).
1) Which implant from implantech- does Dr Eppley use/recommend for tricep muscle implants?
One of the calf implants?
Or one of the contouring blocks- style 1, or do you adapt style 3 which is a bicep implant for the tricep (like the attached photo)
2) Is it possible to place tricep implants sub-muscular instead of sub-fascia without nerve damage to better hide the margin of the implants
Many thanks,
A: To provide any improvement in the tricep implant edge visibility, you have two options:
1) Keep it in the subfascial space with an implant with the identical footprint by with a more feathered edge. (whether that is the same implant modified or a new one doesn’t matter…the key is an implant with an identical implant footprint)
or
2) A new implant in the submuscular space on the humerus bone.
The problem with option #2 is that the external aesthetic effect would not be the same (it would be less because a smaller implant is needed) and there is always the potential albeit low risk of motor nerve injury.
Thus option #1 seems the best due to the least risk.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a jaw wraparound done in Europe but very unsatisfied as it has lost me all my angularity even before the surgery, me cheeks now bulge out like there’s air in them especially when I talk, I feel like I have to bite them in to look good. Is this an implant issue or could it be another issue, if I get them removed and new ones placed in, will the soft tissue return back to normal after removal?
A: I can not comment on the cheek issue as that area should not be affected by a jawline implant.
From a jawline result standpoint this is a classic example of an implant design issue. While it looks like it would be good on the skeletal model you now know what that implant shape and dimensions creates externally. From my experience that design looks like on the outside exactly what I would think it would. It is not a sharp angular design but more rounded at the corners. (chin and jaw angles) You learn by considerable experience that in patients with naturally thicker tissues (like you) the implant must be exaggerated in shape at the corners and with the connection between them to get a more angular result. It takes a lot of experience to come that implant design realization.
I would also ask did your surgeon do preoperative computer imaging on your pictures to determine your exact jawline shape goals on which to base the design? If that was not done then there was never a good chance that the desired aesthetic outcome could be achieved.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am biologically male, and have been undergoing hormone replacement therapy (HRT) for about a 18 months now. I am more comfortable with most of my body now, except for my shoulders, which seem out of proportion to me. From at-home measurements, my bideltoid width is about 47cm. I would like to bring it down a few centimeters, to get a shoulder-hip ratio that falls within typical female range. I am however quite concerned about the risks of long-term pain and reduced movement, and would like to discuss them.
A: Thank you for your inquiry and sending your picture. With a typical reduction of 2.5cms per side, you cold reduce your bideltoid width down to 43cms. To date no patient that has had shoulder narrowing surgery by clavicular reduction osteotomies has developed any postoperative issues with chronic pain or any restriction of shoulder or arm range of motion.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi! I’m contacting you regarding the article here https://exploreplasticsurgery.com/case-study-transgender-rib-removal-surgery-body-contouring/?doing_wp_cron=1619818519.8208200931549072265625 , I’m also transgender and am interested in rib removal to reduce my waist circumference, but I didn’t know that ribs could also be reshaped to change the way they protrude. Would it be possible to alter the size or shape of the upper part of my ribcage? I don’t like how big my chest appears, and if there is a way to make it slimmer I’d be very interested in that. thanks
A: While the lower rib cage can be laterally modified (ribs 10, 11 12), the same can be safely done for any ribs north of #10. (9 and above) which is what you are referring to in changing the shape of the upper ribcage.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to know if an operation is possible. As you can see from my attached photos (+ MRI), I have a lump in the vault of my skull. It makes me very self-conscious. I would like to know if it is possible to reduce it very slightly simply at the point.
To give you an idea, when I press hard on this bump and the skin comes in for a few seconds, the shape suits me at that time. Is it a malformation of the skull? If this operation is possible, is there no danger to the skull? What would be the price approximately for this operation?
I thank you in advance.
A: Thank you for your inquiry and sending your pictures and CT scan. What you have is a classic posterior sagittal crest/ridge. This skull ridge can be safely reduced and it is an operation I do all the time. You have demonstrated how much reduction you need by your skin compression test which is very achievable. Typically the sagittal crest can be reduced 5 to 6mms as illustrated on a drawing on one of your pictures. This is very safe to do as your CT scan shows that there is ample bone to do so.(see attached)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, As you may know, I’m currently deciding between a custom chin implant and a “standard” implant. I have a question for you, if you wouldn’t mind. It is: If we discount the superior aesthetic flexibility from the equation, does it still make sense to choose custom over a standard chin implant for minimizing the risks of malposition and micro-movements that could potentially cause erosion? Particularly in my case, since I have had previous bony chin augmentation.
Thanks so much for the help!
A: The only reason to use a custom chin implant is if there is an aesthetic effect that can not be created by a standard chin implant. There would be no differences between them when it comes to their potential imprinting effect on the bone.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, What is the side by side custom testicle implant? It is hidden when cold and hangs down when it is warm. So I am not sure if you are thinking one or two silicone prosthetics .. wouldn’t it be weird to have 4 balls to touch .. 🤔 I probably did not understand.
A: The side by side technique is where the much larger testicle implant displaces the smaller natural testicles up and out of the way. In most patients because of their naturally small testicles they are not usually felt. This approach avoids the 10% to 20% risk of testicle displacement out of the wraparound or clamshell style testicle implant.
All testicle implants are ultimately just going to hang regardless of the temperature. Natural testicles contract because of the muscles in the attached cord. Testicle implants have no attached muscular cord.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m in the beginning stages of planning a facelift. I’m a 32 year old male who lost 100 lbs when I was 17. I went from 285 to 175 – and with that weight loss, came some loose skin around my body. My face is my biggest concern as it’s hard to cover up and has not shown any signs of tightening up.
I know 32 is young for a facelift but I’m open to other suggestions/options. My biggest concerns are my skin sagging around my cheek and mouth area, jaw line and neck area are not defined very well, some brow area is sagging a bit, and my whole face drops when face down (there’s an awful photo I included). My face is also not symmetric – not sure if that is solvable. I’ve attached some photos for reference.
Looking forward to hearing more
A:Thanks you for your inquiry, sending your pictures and congratulations on the weight loss. With that amount of weight loss there is going to be some expected loose skin in the face. At your young age the skin has a great ability to shrink but at a 100lb weight loss even young skin can not shrink down completely. Given that the vast majority of your concerns are around the neck, jawline and lower facial area, a lower facelift would be the appropriate treatment for it. The question is not whether you can have a lower facelift but whether the scar locations can be adequately hidden (which is always challenging in a male patient) and still get enough of a result to justify the effort. While most of the time I can just look at a picture of a patient and know the answer to these questions, yours is a unique challenge in that regard. This is the one time that I think seeing you in person will help me evaluate whether this is a good procedure for you and will help you best understand the incisional/scar locations for a lower facelift surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I notice a lot of wraparound jaw implant cases from your practice. I myself am looking into jaw and chin augmentation and was wondering what justifies recommending jaw implants over orthognathic surgery besides the respective recovery periods? Are the transformations in appearance generally not as drastic with orthognathic surgery alone? Are implants primarily to place patients within normal cephalometric discrepancies or are they more to do with patient esthetics? Does an objective improvement in the jaw always positively correlate with being in normal ranges based on ceph tracings?
A: There are major differences in aesthetic outcomes and indications for surgery between orthognathic surgery and facial implant augmentations which primarily include the following:
1) Orthognathic surgery is first and foremost a functional operation whose primary goal in most patients is occlusal correction. Any aesthetic benefits are byproducts of that effort.
2) Equally important is that orthognathic surgery mainly affects the sagittal plane, it can not create width or specific definition to the face/jawline beyond that of chin projection.
3) Custom facial implants of the facial thirds produces far more dramatic aesthetic changes than orthognathic surgery that are highly controllable.
4) In custom facial implants cephalometric evaluation/norms are irrelevant. While it is a bone-based procedure the whole intent is what effect it has on the external soft tissues. Thus patient aesthetics rule.
In short, orthognathic surgery and custom facial implants are not comparative operations nor are they interchangeable. Both are done for different reasons with non-comparable aesthetic outcomes.
Dr. Barry Eppley
Indianapolis, Indiana
Can A Hairline Advancement and Upper Forehead Contouring Be Done In A Male Patient At The Same Time?
Q: Dr. Eppley, is hairline lowering + forehead augmentation possible during one procedure and for a male patient? I have a slight asymmetry in my frontal bone where one side bulges out and is more prominent while the other side is flat and has a slight dip. This can be seen in pictures. The result I would like to achieve is seen in pictures 5, 6, and 7. I’d like top of the frontal bone more rounded with the side profiles raised, so that the hairline drops down and wraps around the curve and sits straight relative to my face as seen in picture 5.
From what I’ve read online, a scalp advancement/hairline lowering is not typically recommended for men due to problems resulting from male pattern baldness/receding hairline and the eventual visibility of the incision scar. If this procedure is done, could minoxidil/Rogaine be an effective measure to prevent the hairline receding and hide the scar?
If the scalp advancement/hairline lowering is not done, what other ways could we achieve the result in pictures 5, 6, and 7?
A: Thank you for your inquiry and sending all of your pictures to which I can say the following:
1) A frontal hairline advancement and upper forehead augmentation can done during the same surgery.
2) Like any hairline advancement the first question is always whether the patient’s new hairline position is achievable. Based on your own simulation, by pushing your hairline forward, and the natural scalp flexibility that comes with darker skin pigments, I would say the 10 to 15mm advancement you are simulating appears to be possible. (see attached)
3) There are two significant considerations to make in a male hairline advancement, particularly with darker skin pigments….1) how well will the hairline scar do in such a visible area and 2) as you have mentioned what is the permanency in a male of their frontal hairline position? These are two very relevant aesthetic questions of which the answers can never really be completely known…until you do it. I certainly have done darker skin pigmented males for combination hairline advancements and forehead work and have yet to see these potential adverse issues. But not having yet seen them does not mean they can not occur in the next patient.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I believe I have hyperdynamic chin ptosis as my chin appears normal at rest, however it is very prominent when I smile. I have never had any surgery done, so I believe this might be genetic. I would like to have this issue adressed so that I look the same when at rest and when smiling (my chin no longer looks so prominent/witch-like). What procedure would be best suited for this? Ideally I would like to have the surgery this summer.
A: Like many hyperdynamic chin ptosis patients you have a borderline larger chin at result due to a larger soft tissue chin pad. This larger soft tissue chin pad then pulls down over the edge of the chin bone when you smile. This can only be improved by a submental chin reduction technique in which the soft tissue chin pad is reduced and tightened around the lower edge of the chin bone.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I recently had upper forehead contouring surgery. (attempted forehead horn reduction). The discussed outcome however wasn’t met, as my forehead had been made flat on one side with the other side still having a horn/bump on it, to the point where my forehead is sloped and uneven. The side where my forehead bone has been shaved down too much has also caused my skull to flatten on this side, and I fear that this is dangerous as my brain has essentially had to become squashed into a smaller and flatter skull area. This has definitely affected my concentration. I wasn’t informed that my skull/head would be made flatter prior to the forehead contouring surgery.
As an expert craniofacial surgeon and someone’s work I’ve seen and admire with regards to forehead shaping, I wanted to ask what corrective work can be done as a result of this? I’m looking to potentially fly out in the future and also wanted to ask for your advice on whether the surgeon’s prior work is considered to be medical negligence?
A: In answer to your after surgery forehead contouring questions:
1) I do not comment on other surgeon’s work or abilities, I can only comment on the anatomical problem that I see and what may done about its improvement.
2) There is no medical or harmful issues with your current forehead/skull shape. External bony reduction does not affect the intracranial space or the brain as they are on the other side of the skull. The inner cortical layer of the skull remains intact.
3) Based on your current forehead shape and concerns the indicated correction would be a small right upper forehead augmentation and further left upper forehead reduction.
Dr. Barry Eppley
Indianapolis, Indiana