Your Questions
Your Questions
Q: Dr. Eppley, For a long time Ive been thinking about improving the profile of my face by adding some projection to the mandible.
Doctor, you are renowned Plastic Surgeon, I observe your results and you are a surgeon of my choice.
Do you do online consultations based on sent photos and CT-scan?
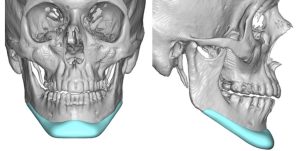
I’m wondering what would work better for me: chin implant or sliding genioplasty.
A: Thank you for your inquiry and sending all of your pictures. Based on some preliminary imaging (see attached) your chin augmentation needs are in the 8mm range for which both an implant and a sliding genioplasty can accomplish.The key aesthetic difference between these two chin augmentation procedures at this normal range of horizontal augmentation is how they differ in chin width and what your feeling is for that chin shape consideration. A chin implant can make it wider or more square while a sliding genioplasty will either keep its same shape or make a bit more narrow.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley ,Some 30 years ago I had cheek implants and I always thought they were a little to big for my face. Fast forward to present day and I had Juva \derm Voluma done to fill out some hollows mid cheek. I believe the person that did the injecting did it too high. It was also my bad for not stating up front I had implants. It never crossed my mind this would even be an issue all these years later. Could this have displaced the implant? Same thing was done the other side and its fine. Can you also advise what types of implants were used back then and can they be removed without a lot of hassle and the cost of removal? Answers aren’t readily available because of age of implants. I’d really appreciate any help you can give me.
A:Thank you for your inquiry and sending your picture. Undoubtably your cheek implants are silicone in composition and can be removed by the route in which they were placed. (intraoral) Because deflating the cheeks by implant removal will have a facial changing effect i would leave the filler alone for now and see how it looks afterwards.
Injectable fillers can never displace cheek implants, particularly ones that are as old as yours are. They are very likely surrounded by calcifications which is very common in ‘ancient’ cheek implants.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am emailing to enquire about reshaping of the skull. This has always been a massive insecurity of mine and it’s become even more prominent in my every day confidence. The back of my head is wider and that is my main concern. I have included a medical letter from a doctor I’ve already seen. I would love to reshape my skull to create an overall more symmetrical appearance. I would appreciate any advice, support or procedure that could be suggested.
A: Thank you for your inquiry and sending your pictures. As your attached letter implies, while parietal eminence reductions scan be done, will it make a significant visible difference externally? In my experience it does because the actual removal involves both bone and a portion of the posterior temporal muscle. Technically what you need is better described as reduction of the posterior temporal lines of the skull. Referring to it as just parietal eminences is a very limited approach and understanding of the actual problem.
A preoperative 2D CT scan to look at the thickness of these tissues in this area would be needed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
 Q: Dr. Eppley, I am currently 26 years old with a standard chin implant in. I am interested in a custom chin implant and I was wondering what the price was.
Q: Dr. Eppley, I am currently 26 years old with a standard chin implant in. I am interested in a custom chin implant and I was wondering what the price was.
I am currently trying to decide between a vertical lengthening sliding genioplasty or a custom vertical lengthening chin implant.
I have included the implant in an attached photo. I want to know if the implant in the photo is considered just a chin implant (though it extends into the lateral mandible) or if it is considered a wraparound implant.
A: You are referring to an extended custom chin implant which costs the same whether the extended wings are there or not.
FYI such an implant design and a vertical lengthening bony genioplasty do not create the same aesthetic effects. While both add vertical length (the bony genioplasty greater than the implant) only the implant adds width to the chin and creates a seamless transition back along the jawline. In other words you are not comparing apples to apples so to speak.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I got a sliding genioplasty last year and my bottom lip is still tight. The area under my lip feels stiff and or like its being pulled. My lips close fine, although my bottom lip appears a little smaller now. I have read a lot of your posts and it seems like the intraoral release with fat filler is something that you often recommend for this. I spoke to my surgeon about it and I was told that a V-Y procedure is something that she offers. Is that similar to what you do? Is it as effective? I am worried that this might make it worse. thank you!
A:Tissue tightness indicates scar contracture which ultimately means there is a tissue deficiency. Tissue deficiency issues are improved by a release, creation of a new dead space (tissue expansion) and filled in with a tissue replacement. (aka fat graft) In other words you solve tissue tightness by adding more tissue, not by simply moving what is already deficient around. (e.g., V – Y advancement) You have justifiable concern that a tissue rearrangement approach would not make it better and may make it worse. (more scar)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a custom wraparound jaw implant placed about a year ago. I have some significant asymmetry, with my right side jawline being smaller and not as sharp. What options would I have in regards of symmetry by augmenting the right side without a total replacement. Could I have a goretex strip overlay? Could I just have the right side of a one piece wraparound replaced without damaging the chin and left side?
A: When one has asymmetry of a custom jawline implant the first question is whether this is the result of implant placement, implant design or some differences in the thickness of the soft tissues. Knowing that most custom facial implants are designed with mirroring software, asymmetries due to design are very uncommon. The most common cause of jawline asymmetries, by far, is placement. Even slight asymmetries in position along one side of the jawline can make for a very visible external appearance change between the two sides. Thus you never consider a revision until you know exactly why it looks the way it does with a postop 3D CT scan. Such scans are tremendously revealing and will help make the choice whether it is to adjust the implant position or perform an overly implant for the smaller less defined side.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a full jaw implant three years ago by a surgeon in Europe. My jaw wraparound implant got infected a few months ago somehow and formed two fistulas on either corners of chin. I took antibiotics and so far no more problems thank god. But the muscle when I smile looks botched as it curves up then straight down giving me a witches chin as I smile. Are you able to fix the fistula holes and the irregular chin muscle ? My worry is if I try fixing anything the infection may return hence causing me to lose the entire implant.
A: That is certainly unusual to have an infection years later. But the fact that it occurred in a such a delayed fashion and is on both sides of the chin suggests to me that this is where screws may be located and are the source of the fistulas. That aside a fistula represents an area of scar contracture and soft tissue deficiency. Thus they are acting as scar anchors that cause distortion when the chin pad moves. (smiling) They would need to be excised, a dermal-fat graft placed and then closed primarily. What effect that may have on recurrent infection is unknown since we don’t fully understand why it occurred so late after the initial surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Im interested in finding a way to reduce my skull and came across your site. I have a very large, elongated cranium that has bothered me my whole life. It has a circumference of 64,5 cm. Since I guess its not possible to change or replace parts of the cranium itself, maybe the burring approach could help reducing the circumference and the overall appearance. See attached images (I have a full CT scan). In my case I would like to reduce both the back of the head and the front to “shrink” the elongated look and maybe get some headwear to fit. Questions: What is the estimate cost for a procendure like this? I am living in Norway so its a long way. Are there any partners in Europe that offers the same type of surgery? How long do I have to stay away from work?
A:You are correct in that burring reduction is the only approach in an adult to reduce an elongated skull. As a general rule half of the skull’s thickness can be reduced by burring. If we move beyond whether the scar to access these to do the surgery is a potential issue, the question then becomes whether that amount of skull length reduction is worthy of the effort. Ultimately the best way to answer that question is by taking a side view picture and doing some computer imaging of the potential change.
I am not aware of any other surgeons in the world that do this type of surgery although there may be.
I don’t know what type of work you do but it should be no more than 10 days at most.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have my initial virtual consultation with you in a couple months, all of which so far are regarding various face concerns. I am now wondering about your custom biceps implant. Personally, I am satisfied with the anterior projection of my biceps muscle. However, I do wish for the lateral and medial sides of my arm to be larger if possible. I have not worked out in awhile right now in these pictures, but even after months of strenuous lifting exercises in the past. I had still found the sides of my arms to not be sufficiently pronounced (mainly the anterior and posterior arm become more muscular). I am wondering if you could design a custom implant to make as minimal as possible augmentation to the anterior arms but rather would fill out my arms’ medial and lateral sides, perhaps fill out the hollowness that is visible at certain angles. I have a few questions though. What is the chance of long-term motor or sensory issues? What are the risks in general of this procedure? Would a triceps implant be better for this? Would this be able to be done at the same time as face surgeries (such as with a combination infraorbital implant, rhinoplasty, and genioplasty)? Thanks so much, Dr. Eppley!
A:Thank you for sending your pictures. Because bicep implants either go under the muscle fascia or under the muscle they can only provide anterior projection that parallels the bulk of the muscle mass. What you are asking is not a function of having an implant being designed to do the job but the anatomic limitations of whether such implants can be placed.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, For orbital rims if you are on a lower budget is fat grafting better then non custom implants? I have a flat face and am worried fat grafting won’t make much difference.
A:You are correct that in your face with very significant midfacial flatness fat grafting would be a wasted surgical effort.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am a big fan of your work. I was wondering if you would perform a medial lacrimalplasty, z-plasty, whatever you would like to coin the term since this surgery probably hasn’t been performed for superficial aesthetic reasons. Ideally I would like to extend the medial canthi vertically downwards, I know it can affect the lubrication of the eye, tear troughs, it carries the lacrimal fluid, and it is one of the most insane eye surgeries hypothetically speaking besides orbital box osteotomy. Are you capable of extending the palpebral fissure length of the eye medially? My optometrist measured my palpebral fissure length, and interpupillary distance and said I have 66.5 mm IPD, and 34mm PFL which is way above average, but ideally I would like 2.5mm+ of PFL.
A: Based on your pictures and description you are inquiring about a Y-V advancement of the lacrimal lake region of the inner eye. This has nothing to do with the inner canthi which, unliket he lateral canthi, can not very easily be moved short of more extensive exposure. (e.g., orbital box osteotomies) This would create some increased palpebral length since the skin-mucosal junction is moved more medially. A Z-plasty is used when the angle of the inner eye is needed to be lower…a shape that you already have.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am considering a revision sliding genioplasty as I had a 4mm advancement which made my chin overprojected (this was two years ago). I have a mild tightness and altered sensation on the right side of my chin which is only in a small area. I read here that this might have something to do with soft tissue entering the ‘dead space’. If I were to have a revision genioplasty to put my chin back 2-3mm, is there anything that can be done to alleviate this tightness/altered sensation.
A: You would probably benefit by he placement of a small fat graft at the same time to add soft tissue fill.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have an virtual appointment with you this December. I plan to get custom facial implants, probably some time Summer or Fall next year. What is the timeline for when you get the CT and also how long before does the final implant design need to be finalized? Isn’t it a good idea to get the CT as close to the surgery as possible since there may be some minor bone changes just from aging?
A:It is generally a 3 month process from getting the CT scan to having the implant ready for surgery. It does not matter when the CT scan is done barring any surgery in the area of potential implantation. Some patibnts use scans that are years old for their custom facial implant designs. Contrary to popular perception there are only very minor bone changes that occur with aging, barring loss of one’s teeth, which do not affect implant designing and implant fit. Almost all custom facial implants are done in patients 59 years or younger where any bone changes due to aging are very minor and irrelevant.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in cheek implant removal and willing to fly over to USA for it. But I have 2 questions
1) WIll cheek go back to normal after removal of small implants, it has only been in for 1 year and its silicone based implantech
2) Are any ligaments cut during placement and removal of an implant like osteocutaneous ligaments?
As some doctors here claim ligaments are NOT cut? Is it possible?
A:By definition placing a cheek implant requires the release of osteocutaneous ligaments. Thus when removing cheek implants there will be some soft tissue sag. The only question is whether it will be particularly noticeable or not.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I hope you’re well. I have midface hypoplasia and want to correct this. The problem is I believe the recession is too great for just implants. Would getting a malar osteotomy first be ideal? Here is my lateral ceph. Thank you.
A:Thank you for your inquiry to which I can say:
1) What is your anatomic basis for saying that your midface hypoplasia is too great for implant augmentation? What is reasoning behind make that conclusion? I see nothing in your x-ray that would lead me to believe that is true.
2) Malar osteotomies create lateral width not forward projection.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 28 year old male writing to you because of my aesthetic concerns about my wide head. I am interested in your skull reshaping surgery because I have a wide head and it has always bothered me psychologically and I have always wanted to reduce its width.
My current head width from side to side is a little over 6 inches and I find my skull to be wider than almost everyone I encounter. I also work in construction and the fact that my hardhat needs to be set to almost the most loose setting makes me feel more conscious about my head size and makes me look more bulky. I get comments about how I look like an “overgrown baby” because my large head combined with relatively narrow shoulders creates a very neotenous look.
I have read through your aesthetic skull reshaping content on your website and I know you explained that a good amount of temple width comes from muscle and not bone but what I wanted to know was if it was possible to actually reduce the bone width as well because I would like a significant reduction in skull width. For example, if we could reduce or take out the muscle width by 9mm on each side and then remove another 9 to 10mm of bone per side I believe that could be a significant change and very strong improvement for me. I know that removing the muscle alone will result in some degree of change but I really desire the maximum reduction in head width because my starting point is very wide. This is my biggest concern about my face and I know that you are more willing to make significant changes surgically to achieve stronger results so I hope you can facilitate this request. My current head width from temple to temple is a little over 6 inches and the more reduction I can achieve the better and this would really improve my confidence and I would really like a narrower head. I would really appreciate your time for a virtual consultation so that we can discuss how to plan this surgery. Thank you so much for your time and I look forward to hearing from you.
A: To answer the question as to whether removing any temporal bone will add to the reduction benefits that the must provides, as well as makes the additional scar length on the side of the head worthwhile, a CT scan is needed to make that determination.
As a conjecture I would imagine that at least the reduction of the parietal bony eminences would be beneficial.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I don’t like the shape of my chin, how there’s a sharp dip from my lip to my chin, and my cleft. I am a very serious patient. I have spent a lot of time researching surgeons and when I came across Dr. Eppley’s before and after photos I was really amazed.
A:Thank you for your inquiry and sending your pictures. You have a classic horizontal bony chin excess which is why your labiomental fold is so deep. This requires a submental chin reduction approach to remove both excessive bone and soft tissue. (see attached imaging prediction of a potential submental chin reduction change)
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I had a chin implant placed in the fall of 2019. It was placed crookedly, and in my opinion too high. Although I voiced these concern’s to my surgeon, he would ultimately tell me each time that the implant was placed perfectly and I looked great. Even if this was the case, and I did look great, I didn’t feel great, and the chin implant was mightily uncomfortable. My lower lip didn’t have the depression most lips do when you smile, talk, or make general facial expressions. Each time I brought up these concerns, he would say it “takes time”. I am aware of the time it takes for the body to heal, but also aware that it should be at least close to normal after a year, but, it was not. The lip was stiff and seemingly stifled in the middle and the sides. I gave up and gave in, tried to live with it for awhile, but four years is all I could take until I needed to seek help. Finally, I went to another surgeon and got the implant removed in the spring of 2021. When I showed him the implant he was appalled at the placement, and said it was heavily mal-positioned. I hoped that removal would help my lip mobility and tightness, and I wouldn’t say post removal has been net zero, I don’t think it’s even fifty percent better. My question is if anything could be done to improve, my feeling and lip mobility? The feeling is like a chin strap, and shape of the implant still lingers. In a perfect world I would go back to my original chin, but the world is not perfect. Oh well. What is your opinion?
A: While you did not say what route the chin implant was placed (submental vs intraoral) this sounds like a classic post intraoral chin implant placement issues. Usually tightness does not occur from a submental approach. Thus this is scar contracture which really means a soft tissue deficiency. In this situations I usually do an intraoral release and fat graft to relieve the tightness.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I underwent chin implantation (extended anatomical chin, large) 2 years ago, with postop course c/b persistent right lower lip numbness. We later found the right wing of the implant was malpositioned superiorly and could be clearly palpated externally and intraorally. Aesthetically, the malposition isn’t very noticeable. Right lower lip sensation is currently 85% of normal
In a few weeks I’m tentatively scheduled for revision since my projection was insufficient (pictures attached, before implant and after). My surgeon plans to place silicone (cut from a block) behind the implant for more projection. But he said that he wouldn’t feel comfortable revising the implant wing since it could cause more trauma to the mental nerve and risk recurrent or worsened numbness. I’m concerned adding silicone behind the implant may make any minor asymmetric aesthetic differences more noticeable
Is trauma to the mental nerve typical with revisions like these, or would I be better served by obtaining a formal second opinion/consult with you or another surgeon?
A: By your original preoperative picture and the type of chin deficiency you had a chin implant was not the best chin augmentation procedure for you. When the chin excess exceeds 10mms and the chin is vertically long a sliding genioplasty is the best approach. The chin can be moved significantly forward and vertically shortened. (see attached imaging) It is important to remember that chin implants worjk best for modest to mdoerate chin deficiencies not signifincant or major chin deficiences.
Stacking silicone chin implants is rarely a good idea. (if you need that much projection and want to use an implant make a custom one as one piece) There is no biologic validity that removing your silicone implant is going to cause increased mental nerve damage. Furthermore why would you try and stack another implant behind a chin implant that is obviously malpositioned??
I assume you have a 3D CT scan which confirms the exact implant positioning on the bone and where the implant is believed to be sitting is not based on external assessment alone.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 29 year old male who has forehead bossing. I am very self conscious of my side profile and would love to find a fix to the problem. In addition to that, I have a pretty sloped forehead with a hair hairline which does not help. I have thought about doing something with my chin to take the depth of the forehead away, but I don’t know what’s right. I am a cop and train boxing often. I am concerned about options holding up long term. I would love to speak to you and learn more. I am ready to fix the issue!
A: Your forehead only looks sloped backwards because of the brow bone protrusion. Once the brow bones are setback the forehead slope looks improved. (see attached imaging) Increasing chin projection will improve the lower facial shape but will not make the brow bones look less protrusive.
Dr. Barry Eppley,
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have some questions about custom pectoral implants:
- Do you believe it is safe to work out the pectoral muscles in the gym after having pectoral implants (especially if big), and if so, when can one start chest exercises safely after surgery?
- What is the risk of seroma and/or displacement (highly theoretical or actual risk)
- Finally, if the implants are patient specific and made to fit perfectly pectoral muscle, are there any limits as regards to implant thickness i.e., projection?
A: In answer to your custom pectoral implant questions:
1) Just like breast implants there are no postoperative exercise restrictions once fully healed. Pectoral implants stretch out the muscle between origins and insertions but does not damage these attachments. But I would wait a mont after surgery before doing so.
2) Displacement is a non-issue. Seroma is a low risk issue having seen it only one time in my experience.
3) There is always going to be some limits with implant projection thickness, regardless of the footprint dimensions of the implant, due to the size of the incision to insert it and the stretch of the muscle to accommodate its volume.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am inquiring about a genioplasty. I would like to make my chin vertically taller and gain significant forward projection. Ideally around 10-12mm. I would also like to hear your expert opinion on whether my entire jaw looks recessed and if I would need more invasive jaw surgery like a BSSO for example. But ideally, I am fixed on getting a large movement genioplasty. Thank you!
A: I would not be able to determine whether orthognathic surgery would be a better option for your lower jaw based on pictures alone. This requires an x-ray and occlusal assessment to make that determination.
All I can do based on these pictures is have the discussion of what type of chin dimensional changes are your seeking. To begin that discussion I have done some initial imaging of one type of change and await your response to it. But with significant forward projection increases (yet to be determined as to what significance ant means) there are limits as to how much vertical height can be done at the same time.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to know if I would be a candidate fordeltoid implants and or shoulder lengthening/clavicle lengthening. (pictures attached)
A:I would definitely opt for deltoid implants as your shoulders are already broad based on your pictures. It is just that the ‘corners’ of the shoulders are rounded and lack a more defined shape. (the deltoid muscle is underdeveloped) Clavicle lengthening may make them broader but won’t give the upper deltoids a more prominent shape.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley,Hello I am interested in surgery to my chin. I want to increase vertical height, reduce the depth of the labiomental fold and if possible decrease horizontal projection. I have been advised this is not possible as my horizontal projection is caused my muscle and fat and it is too complicated to surgically remove this. Can you please give me your opinion? It’s worth noting that I have filler in my lips, if the lower lip filler is contributing to the downward turn of the lower lip, increasing the harshness of the labiomental fold?
A: By definition when the vertical height of the chin is increased the labiomental fold will get less deep and, if the vertical lengthening is done by wedge or hinge opening some horizontal projection will be decreased as a result. These effects are related to the amount of vertical lengthening done, the greater the vertical lengthening the more profound these effects become..
Whether the lower lip filler is contributing to the depth of the labiomental fold (which I doubt) should be known to you as what did the fold look like before you ever had lip filler placed.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I had 2 really big love bands before I had a lower eyelid surgery. I had little extra skin under my eyes and just wanted to look refreshed and the surgeon removed the extra skin and said she also did fat transpostioning. I now still have a big love band under my eyelashes on one eye but the other eye barely has one now and I was hoping to get my love band back on that eye too. I seen you do the love bands with fat transfer and was interested in it. I got filler in my tear troughs hoping it would make my eyes look better but it actually made them look worse because I have lumps of filler in my tear troughs so I plan on dissolving the filler in my tear troughs soon. I sent a picture of my eyes after surgery but before I got the filler and a picture of my eyes now after I got filler but like I said I am going to dissolve the filler soon. Please help me get my love band back so I will have 2 love bands again. Thank you.
A:T hank you for sending your pictures. Since you already have had a lower blepharoplasty procedure injecting fat is less likely to be successful due to the scar. It would be more effective to use the scar that exists and lay a thin piece of Alloderm graft to recreate the love band.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Would like to know more about this procedure. As you can see in the photo I have a skull bump in the back of my head that i can do without. I have a short haircut and would like to know if scarring will be visible after the operation? And how much healing time before I can go back to work after procedure?
A: Thank you for your inquiry and sending your picture. You have a classic occipital knob skull protrusion which can be effectively reduced. In answer to your occipital knob skull reduction questions:
1) The small scalp incision used for the reduction heals in an inconspicuous manner in most patients. No patient has ever requested a scar revision due to its ‘visibility’.
2) You should be able to return to work the week following surgery almost regardless of what your vocation is.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I want to consider total midface augmentation with custom implant.I know you are one if not the best in the world using implants. I have a question. I suffer for years from chronic allergic rhinitis.I would like to know if a custom midface implant may be effected from allergic or sinusitis. In that case is it any problem if i use implant. Could the implant cause more sinusitis infection or increase allergic symptoms? An opinion from you is very welcome due to your experience.
I thank you in advance
A:Your question concerning any possible adverse connection between a midface implant and the maxillary sinus is a understandable one. While the two are in close proximity there is no direct communication between them. They are separated by the anterior bony wall of the maxillary sinus. The bone thickness of the maxillary sinus wall may be thin but it still serves as a solid separation between the sinus air cavity and where the implant would rest on the bone. So no a midface implant would not cause a maxillary sinus problem nor aggravate an existing sinus condition.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I’m thinking about having a couple of skull reduction surgeries and I was wondering if you could provide a price estimate for all the surgeries together. Overall, through these surgeries I would like to decrease the overall look and size of my skull. Here are the surgeries that I plan on having.
Temporal reduction: I would like my temporal muscles removed to decrease the width of my head.
Occipital reduction: I would like bone at the back of my head reduced so that it looks more flat, and less bulging than it is now.
Forehead bone reduction with hairline advancement/lowering: I would like to the bone under my forehead reduced so that it doesn’t look as bulging as it is now. I also have a pretty long forehead which makes me look like I have a receding hairline. If possible I would like to have my hairline lowered by 1 inch, or 2.5cm.
Top skull reduction surgery: I would like the bone on top of my skull reduced so the vertical length of my skull is reduced. Just like in the pictures of the large skull reduction surgery. So that the distance between the top of my hair and my hairline is not too big after having the hairline advancement surgery.
I also have another question in regards to these surgeries. When I do get them, will they all be done together in one session, or will they have to be done separately? Like will I have to wait a couple of months between each surgery? Just so I can know how long it will take to get them all completed.
Thank you
A:Thank you for your inquiry, detailing your objectives and sending your pictures. All such procedures could be done at once if desired. (see attached imaging) Besides the temporal reductions the back, top of the head and hairline/forehead procedures are interconnected and the effectiveness of one impacts the other two so the ‘front to back’ skull procedures need to be done at the same time. The temporal procedure is independent of the other three and cold be done separately or as part of the other three, that is just a personal choice.
Whether you could get as much as 25mm frontal hairline advancement can not be predicted beforehand and depends on the natural stretch of your scalp. But certainly the back and top of head undermining/bone reductions is going to maximize whatever hairline advancement is possible.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, For a customized jaw implant, do you use a CT scan and special software to design the customized implant?
A: All custom facial implants are designed for each patient off of their 3D CT scan using Geoform implant designing software.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Can midface implant make nasomaxillary complex more forward and change the angle of “cheek line”. By a cheek line I mean a line from lower eyelid to nasal base; on flat midface is it more vertical while on projected midface it is more sloped(I attach photos to make it clean). Standard double jaw surgery with counterclockwise rotation doesnt reach. Probably the best solution to that would be Lefort 2 with counterclockwise rotation or other nasomaxillary osteotomy but its probably more risky. Rhinoplasty also wouldn’t make a difference to cheek line since it would only make nasal tip more projected why the midface is still flat/vertical.
A: A midface implant can very well change the cheek line as you have indicated by improving the projection of the nasomaxillary complex.
Dr. Barry Eppley
World Renowned Plastic Surgeon