Your Questions
Your Questions
Q: Dr. Eppley, What would be the process be like to design new implants precisely if I already have other implants that cover my own jaw?
Even if i have had the implants for almost 9 years now, could they be safely removed and replaced with new ones in the same operation? I have read that when removing medpor implants the bone and soft tissue itself can be detached, so this aspect worries me quite a bit. Does Dr. Eppley have experience removing this type of implants in the mandibular angles succesfully?
Finally, approximately how long it would take for the swelling to go down significantly?
Thanks in advance.
A: With Medpor implant replacements there is no designing implant replacements precisely because they can not be seen on a 3D CT scan unlike other materials. Unless they were custom implants originally, where their exact designs were known before placement, there is no way to know see the implants now on the bone.
I have removed hundreds of Medpor facial implants and they can always be successfully removed…albeit with more trauma to the tissues than when they were placed.
Medpor Implant replacements will have similar swelling and recovery period as the original implantation surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in shoulder narrowing surgery. I have been very impressed with the results presented on your website and, as far as I’m aware, most people who had undergone this surgery seem to be rather happy with their outcomes. I would like to ask you a few questions about this surgery:
1. As I am currently a bit underweight, I would like to know whether I need to gain more healthy weight before proceeding with the surgery itself, for an easier recovery process. Is that correct? (I will provide all the measurements below)
2. If I understand correctly, reducing the clavicle bone length would slightly roll the shoulders forward. Should I try to compensate for this effect by exercising my core back muscles before and/or after surgery? On a similar note, would using a posture corrector after the clavicles heal enough be of any use in correcting the posture initially?
3. Lastly, I would like to know whether having a smaller ribcage and quite broad shoulders allow for a slightly greater clavicle width reduction.
Height: 5’9″
Weight: 110lbs
Thank you for your time and consideration.
A:In answer to our shoulder narrowing surgery questions:
- One’s weight is irrelevant to the surgery. The thickness of the soft tissues over the clavicle has no bearing on doing the surgery.
- Your weight is less important than your nutritional health. If in doubt you check your protein and albumin levels which are indicators of the ability of tissues to heal.
- The rolling in of the shoulders is a temporary effect of the postoperative positioning of the arms in recovery. It is not a long term effect.
- The amount of clavicle bone that can be removed is related to the length and shape of the clavicles, the width of the ribcage has no bearing on how much clavicle bone can be removed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I need to speak with the surgeon about how he intends to prevent hypertrophic/keloid scarring from rib removal surgery. I’m prone to hypertrophic scars when not managed right. I’ve had surgeries successfully without them and had a couple where I did keloid because of messy/shoddy stitching.
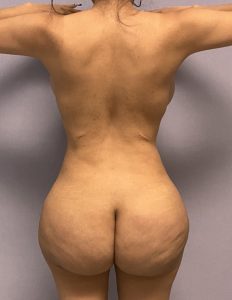 A:Based on my experience in rib removal surgery hypertrophic scarring is not what I have seen. It is true that thicker more pigmented skin does not scar as well as thinner less pigmented skin but an average scar result in such skin from rib removal surgery is shown in the attached result.
A:Based on my experience in rib removal surgery hypertrophic scarring is not what I have seen. It is true that thicker more pigmented skin does not scar as well as thinner less pigmented skin but an average scar result in such skin from rib removal surgery is shown in the attached result.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, i’ve reached out before because the shoulder narrowing is something i’ve definitely wanted to get done. I was thinking about doing one side at a time. i’ve notice that my right shoulder’s clavicle is a bit more curved, and i know that you put straight plates in there, so idk if my case would be a problem?
A: A staged approach to shoulder narrowing is perfectly valid and has certain advantages in terms of recovery. It is common that one clavicle is longer and/or more curved than the other. That does not pose any problems for the surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi is there a surgery to make the inner eye corners more down turned I read on your website about z plasty.
A:Yes there is. Turning the lake of the inner corner of the eye down can be done by either a Z-plasty or a Y-V advancement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a very long upper lip. My teeth was not showing when I smiled. Then I had a bullhorn lip lift 2 times. The middle Part is now perfect but the mouth corners are too low in my opinion. This gives me a sad or uninteresting face mpression ff I do not mmile slightly.
In your opinion would the upper lip ook more harmonic If the lateral corners were lifted?
A:A subnasal lip lift affects the central 2/3s of the upper lip which becomes fully apparent when it is done twice, creating vermilion show disproportion. Lateral vermilion advancements would be the only to make for more proportionate vermilion show from one mouth corner to the other. Although be aware the effect of these lip procedures will make the upper lip fuller (more vermilion show) than the lower lip.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have read many of your articles and I am impressed with your ability and skill to help many patients that other surgeons cannot seem to.
I have issues with my chin after surgery in the same way as some of your case studies suggest.
I had bimaxillary jaw surgery in 2007, in which the surgeon performed a sliding genioplasty that left me with a chin that was too horizontally and vertically large, as well as far too projected past my lip. In 2010 I had the lower jaw screws removed, as they were creating visible lumps on my jaw. This was via an intraoral incision.
In 2018 I finally had a chin reduction, I think by burring, and via an intraoral incision. The surgeon also performed a mid-facelift to help with tightening the skin after reduction- although I would have thought it should have been a lower. Not enough was taken off the chin, however, and in 2019 I had it revised via another intraoral incision. It was flattened projection-wise, but not narrowed or shortened enough, leaving a rather wide, and vertically long (mainly when I smile) chin still, but with excess soft tissue that now is unsightly and causes me problems including lip ptosis.
My lips no longer sit together when relaxed, and talking is very uncomfortable- some times more than others, as I have to stretch my top lip down to pronounce certain words, and my mouth feels very tight when doing this. (I also have a long mid-face, which may contribute to this). I also have a very dimply/scrunchy chin unless I get Botox/Dysport in it, which doesn’t entirely fix it.
I also embarrassingly find myself dribbling sometimes if I am not consciously holding my lips together, which is uncomfortable to do all the time.
I have since tried to do some research and realised that the intraoral approach can create lip/chin ptosis. Especially since I have had it four times for the varying reasons. I am looking for someone to help me tighten the chin area with soft tissue excision, correct the lip ptosis, and even further vertical and horizontal chin reduction. I am aware it would likely require an external incision approach and I am happy to undergo that to fix the problem. I live in Sydney, Australia, and first would sincerely appreciate if you knew of a good surgeon in Australia (preferably NSW), who could surgically address my concerns. Otherwise, if I could get some advice or have a consultation with yourself about the steps I need to take to fix it.
Thank you so much for your help, and kindest regards,
A:Thank you for sending your pictures and detailing your surgical history and current lip-chin problems. In summary you have a redundant soft tissue chin pad with some lower lip incompetence. These are very diametric problems as soft tissue chin pad excess is treating by the removal of tissue (submental excision) while lip incompetence is treated by the addition of tissue. (intraoral vestibular shortening and dermal-fat grafting) But the soft tissue removed from the submental excision could be used as the tissue graft for the vestibular release. So while there are diagnostically diametric they are procedurally synergestic.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Why does increasing width on the wide of my head restrict augmentation on the back of my head? I am asking because I have a bit of a flat head. I also am wondering if I could also increase the width of my face during one procedure around my head. I have a narrow face so I would like to increase the total width in general but minimally because I want it to look as natural as possible. Overall, I am looking to increase the total width of my face by around 7-8 mm and I am looking to increase the total circumference of my head from around 55.5 cm to 56.5 cm. And if possible I would also like to fix the back of my head which is flat. I want to keep the same look on my face, just slightly bigger, I don’t want anything that looks unnatural.
A: The scalp can only take so much implant volume. It does not have a endless ability to be stretched. Thus if you buildup the sides there may not be enough scalp stretch to add anything to the back.
Since the scalp provides implant size/volume limitations there is no risk of looking unnatural…which almost always refers to a size change that is too big.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in cheek implant revision surgery. I had cheek implants several years ago but because the implants did not provide me with the volume enhancement I wanted, I subsequently had fillers in both the malar area on the edge of the implant and in the submalar area right under the implant. Although I was satisfied of the combined effect I experienced twice manifestation of infection on one of the implants which has been addressed both times by antibiotics but I understand it is likely to come back (if biofilm has been created). So I would like to inquire about removing existing and replacing them with new ones that also provide the desired volume reducing the need for fillers.
A:While you did not state the exact style and size of the indwelling cheek implants they are clearly of the submalar variety of which there is a style 1 and 2. Also what is more unknown is where on the bone the implants actually are. Just because it is sitting a certain way on the model example does not mean how it is actually placed that way on the bone underneath it.
While the first cheek implants were a ‘best guess’ approach to get a desired result that should not be how you approach it the 2nd time. If you don’t know precisely the cause and effect relationship between implant details (style, sise and placement) and the effect it would just be guessing again the 2nd time. The point is I don’t consider implant replacements without a 3D CT scan so this information is clearly known. With that information then I can decide is there a better standard cheek implant that will work or do we have to go the custom design process to make it work.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Greetings, regarding Skull/Head Augmentation, is the 1st-stage expansion required for all of the surgery methods or only a few when it’s for large implants ? From what I have understood the 1st-stage expansion alone would help to be able to get bigger implants such as 200cc to 350cc ? So the 1st-stage expansion could help someone with a tight scalp to get a bigger implant that he could naturally have without the expansion ?
To have an idea – what is the equivalent in thickness (in mm) of a 200cc & 350cc implant?
A:Your concepts about the need for a first stage scalp expansion for implant volumes greater than 150ccs – 200ccs is correct. While the surface coverage area is one of the most important aspects of a custom skull implant, and I obviously don’t know what your surface area coverage needs are, it is not possible to say exactly what thickness any implant would be at those volumes. But it is fair to sat it is likely any implant projection thickness over 15mms.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a young male and I am not happy about my mid face/under eye area. I’m not sure if I need implants, fat transfer or if my bone structure is weak. Also my forehead bone looks like it excessively sticks out and it’s narrow at the sides. I did consider bone shaving because I also don’t have much of a brow bone like males do. I was unsure because I was told by a surgeon that my mid face is weak that’s why the forehead looks prominent.
Also, is there anything that can be done about the fat coming down at the sides of my nose (nasolabial folds… I think), can the fat or tissue be repositioned?
A: In answer to your questions:
- You have a relatively significant undereye (infraorbital-malar, IOM) bony deficiency.
- For which fillers and fat injections are both ineffective and not good treatment for it.
- Only custom IOM implants can make a reliable and effective improvement.
- Your nasolabial and the tissue above them reflects the lack of IOM bony support above it which allows this tissue to ‘fall down’ onto the nasolabial folds. Such fallen heavy tissue can not be repositioned but IOM implants may help lift it a bit.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I’m considering surgery to reduce my occipital knob. Are there risks for this kind of procedure? What kinds of scar would I expect? Is there any chance I could lose hair?
A: In answer to your occipital knob reduction questions:
- Occipital knob reduction surgery has no significant surgical risks.
- It is done through a 1 inch incision which heals well and leaves no visible scarring.’
- No hair is shaved for the procedure nor is there any resultant hair loss from doing the surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, with regards to lengthening of the face, to my knowledge (I am by no means an expert on anything surgical related so please forgive me if I’m wrong), craniofacial distraction osteogenesis is used for lengthening the whole face and the cranium for patients with deformities. I wonder, could this process be used for non deformity cases and now I am also questioning if it really does lengthen the face (as you said jaw implants were the only surgical option for lengthening the face).
If it does in fact lengthen the face but cannot be used for non deformity cases, may I know the reasons why?
And finally, do you think in the near future there would be advancements such as internal nails (I did Quadrilateral Leg lengthening in 2015) which are used for the lengthening of the limbs?
A: Distraction lengthening, while being a useful procedure for severe craniofacial deformities, has no role in aesthetic facial concerns for variety of practical reasons. The application of external devices, scarring and protracted distraction and healing times makes the concept of ‘bone expansion’ in aesthetic facial surgery unacceptable to almost all patients.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My goal is to have a chin that just extends a little further than my lips.
Would it be possible with the xl Flowers Mandibular Glowe of 14mm or is it best solved with a custom implant?
I have measured that my chin is short of about 15mm.
I think these are VCN questions:
1. Would you in any case recommend the use of an XL Flowers Mandibular Glowe implant with a total horisontal projection of 14mm? Or is it generally better to use a custom implant to adress this amount of horisontal projection?
2. Also, does the amount of a chin implants horisontal projection translate 1:1 with the actual achieved horisontal projection that is gained once it is inserted?
A:My general rule is that once the chin deficiency exceeds 10mms a sliding genioplasty is better than a large mass of implant on the chin. But if one wants to use an implant the only standard option is the mandibular style.
- It is never an exact 1:1 ratio of bone augmentation to the external softy tissue contour change due to the compressibility of the soft tissues. It is about 0.9:1 change.
- The role of custom facial implants in aesthetic surgery is two-fold; 1) when the aesthetic goals can not be achieved by the use of any standard implant or combination of standard implants and 2) when there is obvious asymmetry of the bone shape.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have had two double jaw surgeries in the past. My last surgery was in 2020. However, I think my upper jaw/nose has sunken again and I have read your article about paranasal implants. I was wondering if this might help to solve the case. I have included some pictures to show you my problem.
A: Nasal base hypoplasia is treated by paranasal, premaxillary or premaxillary-paranasal augmentation depending upon exact location of the deficiency. After having maximally changed the bone implant augmentation would be remaing treatment choice. Based on your pictures I would say that paranasal augmentation alone, as you have stated, appears to be the correct area of nasal base augmentation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I really appreciate the effort you put in all your articles and case studies. I am interested in back of the head augmentation. Since I only would need a small amount of additional volume for a more aesthetic and rounded head shape, I think your article of using fat grafting (especially for augmentation of the area lower than the nuchal line) is very interesting.
Since you and also other plastic surgeons say that fat grafting is not a permanent solution in this area, I wonder if there are any patient cases, where x % of the transfered fat really stayed at the desired positions for many years? I would be extremley happy, if it could be a permanent solution. Even if a 2nd fat transfer would be necessary. I attached an image which shows the little volume increase I desire. I am looking forward to your reply. Thank you very much in advance!
A: I think the use of injectable fat grafting for small areas of head shape deficiencies is a viable low risk non-incisional approach to select head augmentations. Its potential success is based on two factors, 1) how much fat survives (which is largely known by 6 weeks postop) and 2) how much donor fat is available for harvest. In young male patients I am more focused on #2 than #1.
In my experience with injectable fat grafting to the scalp, which is where it is placed for head augmentations, it generally works fairly well for low volume needs. Its long term retention (meaning years or a lifetime) I can not say nor have ever commented on because it is unknown. One should not confuse survival vs retention as they are two different fat fate issues.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in M2F body contouring procedures around the hips and waist to provide for a more feminine presentation. I have been using a padding technique to create the appearance of typically feminine curved hips for years, but find that the logistics of keeping them secured limit my options to high-waisted and knee-length clothing which are not compatible with the hobbies I enjoy like swimming and dance.
My primary goal would be to add visual width to my hips between the iliac crest and the greater trochanter regions in a way that creates a natural-looking curvature from the waist down through the outer thigh. Secondary to that would be to create a more defined waistline with a gentle transition from the ribs without significantly reducing my waist measurement. I understand that a smaller waist would provide the appearance of larger hips by contrast, but I am concerned that reducing the waistline would also emphasize the larger ribs and shoulders in an undesirable fashion.
My questions then stem from the potential options to meet those goals:
-I’ve read about augmenting the iliac crest with an implant onto the bone structure, but how far down into the greater trochanter would that impact?
-At the current time, I’m not interested in augmentation of the buttocks, but if that changes in the future would it be possible to perform a fat-transfer or implant augmentation once the hips have been completed?
-Would a partial removal or reshaping of the lower ribs be appropriate to lengthen the waistline and ease the transition from the ribcage?
-What would be your professional recommendation on how to achieve the desired results.
A:In answer to your questions:
- Iliac crest implants augment the crest only, they do not extend below the crestal bone., In other words they augment one and only area of the upper hips.
- Iliac crest augmentation does not preclude future buttock augmentation efforts.
- Lower rib removal does not lengthen the waistline as they are not visible ribs.
- Where you put the padding is your proven method of the desired area of augmentation. I would have to see pictures of what that padding looks like and where is placed on you to determine what procedure(s) may replicate that effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, If I get the plates removed after clavicle reduction surgery (shoulder narrowing) will my clavicles be in any way weaker in the long term? is there long term evidence existing on people who have had plates in and then removed?
A:When hardware is removed from the clavicles the healed osteotomy site may not be as initially strong as the plate as protected it. So patients need to be careful about too stenuous movements in the first few months after their removal as the bone ‘relearns’ how to sustain full weight bearing.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,There is something I would like to hear your option about. About 1 month ago I got a surgery for a saggital crest removal, like you did in many of your cases. The plastic surgeon removed about 1 mm of it and told me, there is no way to go deeper, because of the diploic space. In your cases you describe about 5-6 mm wich would have been more than enough for me. I think he was scared to burr deeper, he definitely haven’t got the experience in those cases as you.
Let’s say he is right and he was close to the diploic space, is there no way you can burr a little bit into it as well? (Maybe close it again with bone cement f.e.) Btw. No x ray scans were taken
I am looking forward to visit you, I was wondering, how do you reach the 5-6 mm ? A answer would mean a lot to me
A:I obviously can not speak to what was observed during your sagittal ridge reduction surgery or how thick your sagittal ridge actually is. What I can say is that based on my experience it would be unusual for a 1mm bone reduction to end up in the diploic space and there would be a need to stop there. Certainly if you don’t have a lot of experience in skull surgery and don’t have a preoperative CT scan to absolutely know the thickness of the bone I can see why a surgeon would stop short of a maximal reduction.
That being said don’t presume before having another procedure what the bone thickness is. Approach any further sagittal ridge reduction knowing what is both possible and safe. That is how I would do it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in the largest custom butt implant that I can obtain with or without fat transfer. Is 1,000 ccs the largest available? Do you place tissue expanders in the buttocks as an option? Thank you.
A:Unless you have indwelling buttock implants you have correctly surmised that first stage tissue expanders would be first needed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I want to increase the width of my face/head. My forehead area feels especially narrow and I defiantly want to make it wider, including my jaw and cheekbones. My concerns are that my eye and brow area is aligned with my forehead so by increasing my forehead width would my eye area look small and disproportionate? Secondly I also want to increase the width of my skull and at the back too because I have a flatter head. Another one of my concerns is with the safety and scars associated with these procedures.
A: in answer to your skull augmentation questions:
- While the side of the forehead and side of the head can be augmented with custom head widening temporal implants whether that may make your eyes look small can only be determined by looking at these effect swith computer imaging. I would need a front view picture to do so.
- While the sides of the head can be increased that would either eliminate or restrict any augmentation on the back of your head.
- Skull augmentations like these discussed are perfectly safe and can be done with remarkably minimal scarring.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, wrote a month ago with regret after a chin reduction procedure, and if you don’t mind, would you answer some further questions? I had a CBCT scan done before my reduction. It was done intraorally, and the surgeon removed 4.9mm bone from the bottom of my chin then smoothed and rounded the shape. He did not cut into the bone to remove a wedge. I am still regretful, I miss the old length and squarer shape to the chin, despite this being more masculine looking (I am a female) I do think it suited my face and figure better and I miss how I used to look.
The surgeon has suggested another CT and comparing the difference between this and the pre surgery CT and having a custom made chin implant from PEEK material.
My questions are as follows:
1. In your experience with similar cases, with this method how likely is it that my chin will look like the old one?
2. The tubercles of the chin were removed with the reduction, will the custom implant shape give the appearance of these back?
3. The surgeon spoke of placing the implant via the intraoral route, he did not give a reason and I will need to ask his reasoning at our next appointment, but do you see any reason this can’t be done submentally and with local anaesthesia only?
4. The implant will be fixed in place with titanium screws, is this painful, and a reason for using sedation or general anaesthesia?
5. For patients you have seen with facial contouring regret and subsequent restoration with implants, are they generally happy with the results of the implants and do they report that they feel like/recognise themselves again?
6. In this situation, how long should I wait from the initial surgery to having a custom implant made and placed or does it not matter? Is there a possibility my chin bone changes/bone regrows at all?! I’m concerned then that putting an implant on top will make the chin bigger and different to the original. I am looking to have as close to my original chin as possible.
Thank you for reading Dr Eppley, and best wishes to you.
A: In answer to your chin reduction questions:
- It is fair to stay that with a pre and post reduction 3D CT scan you would come as close as humanly possible to restoring your original chin shape.
- A custom design would replicate the original chin shape with the lateral tubercles since you have a pre reduction scan.
- The custom chin implant could be placed submentally. The choice of anesthesia is between the patient and the surgeon, both have to feel comfortable that the implant can be successfully placed regardless of the anesthetic choice. I could answer that question more decisively in regards to local anesthesia once I saw the size of the implant.
- While screw fixation is essential it is not painful.
- Most facial bone restoration patients move on after they have ‘returned back home’ or as close as they can get to it.
- Given that the custom implant design process is several months in duration you initiate it as soon as you are convinced it is needed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a small head and face and I want to increase the width of my jaw and mid face. I also want to increase the width of my forehead and temple area as it is very narrow. My concerns have to do with the time it would take to heal and the overall safety and scar. Would I be able to keep my hair short or would scars be visible. I also want it to look somewhat natural. Lastly my concern is that my eye area would look small in proportion to my face if I increase the width of my temple area, unless I can somehow increase the width of my eye area.
A: in answer to your skull augmentation questions:
- While the side of the forehead and side of the head can be augmented with custom head widening temporal implants whether that may make your eyes look small can only be determined by looking at these effects with computer imaging. I would need a front view picture to do so.
- Skull augmentations like these discussed are perfectly safe and can be done with remarkably minimal scarring with incisions behind the ears.
- The recovery from any form of skull augmentation is about the swelling and/or bruising that will result from the surgery. It usually takes ten days or so afterwards to look presentable/normal.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, 1. Will the bone grow back to its original size or close to its original size (will the surgery money being spent be in vain after a period of time due to bone regrowth)?
2. Is a consultation done over Skype for those that don’t live nearby?
3. If the surgery doesn’t do enough the first time can it be repeated?
A: I assume you are referring to skull reductions:
1) Bones does not regenerate or come back after it has been reduced.
2) All consultations, regardless of the patient’s geographic location, are done in a virtual manner. (Zoom)
3) All skull reductions are done to the maximum possible (down to the diploic space) where such reductions have to stop. Whatever result that can be achieved then will have been done. There are almost no skull reduction revisions, as once it is done, that is all that can be done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, looking for a resolution for my left shoulder. I had an AC joint injury in 2019, which required surgery. Since the surgery, my left shoulder is smaller than the right one. So, I’m trying to find a solution that will make my shoulder more symmetrical to the other.
A: Thank you for sending all of your additional pictures. They conform that this is an overall shoulder issue.as I would have expected given the origin of the problem.
They are two approaches to take for aesthetic improvement; 1) injectable fat grafting or 2) deltoid/trapezius muscle implants. There are arguments to be made for either approach and neither is wrong. It comes down to the classic debate of autologous (fat = unpredictable volume retention, use of your own tissue with as close to zero risk of infection as possible vs. implant = assured volume, placing a foreigh material in the body with more risks of infection than fat)
It really comes down to your preference.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I recently had cheekbone reduction which caused my face to look flat and lose so much volume. It caused it to sag. I look 10 years older.
A: Such sagging is a known aesthetic risk of cheekbone reduction due to loss of bone support and soft tissue ligamentous attachments. Partial or total reversal is typically done with implants, preferably custom designs
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q:Dr. Eppley, Hello. I wanted to tell Dr Eppley that my forehead masculinizes my face. There’s a bossing I would like to reduce. And a ‘line’ diving my lower and upper forehead I would like gone if possible. I had a hair transplant 2 years ago.
A: Thank you for sending your pictures. The frontal bossing can be reduced within the limits of the thickness of the bone. While visible reduction will occur I suspect that it can not be reduced enough to eliminate the valley between the bossing and the brow bone area. To smooth out this transition, which will also make the bossing reduction look even better, will require filling in the valley a bit using some bone cement. Whether this addition will absolutely be needed as part of the bossing reduction can be known beforehand. That will have to be an intraoperative judgement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, how long does the swelling from a chin shave via submental incision last? After 16 days, my chin still looks large. When will I look normal? 🙁
A: Significant resolution of swelling from an inferior border chin shave takes 4 to 6 weeks to occur and complete resolution 2 to 3 months. You are early on in the process and I would expect you to not yet be in the ‘benefits’ phase of the surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have gotten a Vertical chin implant and was satisfied with the horizontal projection but the 45 degree angle vertical projection , I tried to like it but feel like I did not need the extra vertical or 45 degree angle look. My question is, if I switch the implant to a Terino square chin implant, will I lose the vertical height and 45 degree projection length and have almost the same horizontal length projection of the chin implant.
A: With the chin pad stretched out at 45 degrees I would be aware that switching to a pure horizontal projecting chin implant with the same horizontal projection may leave some loose tissue vertically. Whether that is significant can only be known by doing it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in testicle enlargement purely for aesthetic reasons. I just want very large testicles.
I’d like to explore these options, and the pros and cons for each. For example, can I still go on a 6 mile run with either approach? How about ejaculation? How long do the implants last?
I also have a small hydrocele on one testicle. Do I need to get this removed beforehand?
A: In answer to your testicle implant questions:
- While there are two method for testicular enlargement (wrap around and side by side) I am not enthusiastic about the wrap around method due to the high rate of complications. (testicle-implant separation) The side by side method is best of one has naturally small testicles not normal size ones.
- Large testicle implants may interfere with running given the larger masses betwen your legs.
- Testicle implants do not interfere with ejaculation.
- A hydrocoele would need to be removed first.
Dr. Barry Eppley
World-Renowned Plastic Surgeon