Your Questions
Your Questions
Q: Dr. Eppley,I previously underwent orthognathic surgery with mandibular advancement and genioplasty. My primary concern is aesthetic rather than functional. I would like your opinion on whether a revision orthognathic procedure could provide a meaningful aesthetic improvement.
More specifically, I would like to know whether additional maxillary advancement could improve facial harmony, midface support and upper lip projection, and how it might affect the appearance of my nose (wider/larger versus more balanced and harmonious).
Based on the records provided, do you believe there is significant aesthetic potential for improvement through revision surgery?
Thank you for your time.
A:The simple answer is no. You have already obtained the most aesthetic benefits in what bimaxillary surgery with a genioplasty can do. Further aesthetic facial enhancement are going to come from adding on with other procedures to what you already have such as secondary chin augmentation, rhinoplasty, and midface implant augmentations.
Bimaxillary surgery rarely achieves all of any patient’s objectives because it is a dimensionally limited procedure with its his primary benefit in increasing facial projection. But there comes a point when more facial projection by bone movement is not effective or even counterproductive.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I developed scoliosis and had a long fusion 6 years ago. I’m interested in rib contouring to address rib asymmetry.
A:Rib asymmetry is the norm in scoliosis which is usually most manifest in the lower rib cage. While the rib asymmetry can never be fully corrected it usually can be improved by identifying the rib(s) that causes the greatest protrusion on the convex spine side. This is done by a 3-D CT rib cage scan and then matching that with what the patient sees on the outside.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, O have been researching deep plane facelifts and am seeking advice on how to combine that with an orbital-malar implant.
A:Thank you for your inquiry and sending your picture and that of the AI generated image. As you have astutely noted an Ai image is an ideal goal that can never be fully achieved. An Ai image makes many other soft tissue changes but either aren’t in the scope of what the patient wants to do or are simply not possible. For example in your AI image it has completely eliminated your nasolabial folds (not possible with any form of the facelift), enlarged your lips, narrowed your nostrils and even changed your eye color.
But that being said it is tremendously useful from a structural standpoint because those are changes that are very possible. Eliminating/reducing your undereye hollowing with higher cheekbones exactly is what an infraorbital – malar implant can do and will produce higher cheekbones and a lifting effect that can never be achieved In any type of facelift surgery.
If the question you are asking is can you combine a deep plane facelift with custom infraorbital-malar implants and that answer is absolutely. That is not a technical question but a logistical one. The key to that combination, as it is with any type of niche procedure in plastic surgery, is finding a surgeon who is capable of doing both. The facelift part of that equation is easy, it is the custom implant part that becomes more difficult given the rarity of surgeons are actually perform it.
But if you had to stage it, and I’m not saying you should, you would do the custom implant first to establish the skeletal foundation and then do the facelift secondarily.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I am interested in learning more about your custom testicular enhancement procedures, specifically the side-by-side displacement implant technique.
My goal is a substantial cosmetic enlargement rather than a subtle or natural-looking enhancement. I have reviewed your website extensively and have seen references to implant sizes ranging from 6 cm to over 10 cm.
One aspect of my history that may be relevant is that, although my resting scrotum is relatively tight, I have performed saline infusions into my scrotum, reaching maximum size of around 17.5″ in circumference. I understand that temporary expansion is not the same as permanently supporting large implants, but I wanted to mention this in case it is relevant to tissue elasticity, implant sizing, or the potential for staged enlargement.
My questions are:
1. Based on my anatomy and expansion history, what implant size range do you think is realistic?
2. Would you recommend a staged approach, or could my desired result potentially be achieved in a single procedure?
3. Do you think I could ultimately be a candidate for very large implants (9–11 cm range)?
4. What is the largest sized implants you have used in a patient?
A:Thank you for your inquiry and detailing your testicular enhancement objectives. Your history of saline scrotal infusions is very relevant as this suggests you would have a large scrotal stretch skin capacity. This along with your height and weight, indicating you are not a small size male, would indicate that very large testicular implants would be appropriate. Just based on that information alone I would think that the size range of 9 to 11 centimeters, as you have noted, is well within the range of what will likely fit.
The largest testicular implants that I have a placed is 11.5cms. As you might guess at that size this patient also had a history scrotal expansion and it also graduated from an initial 8.5 cm to the 11.5 cm size.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I need a custom PEEK implant to square off a narrow, pointed chin. My side profile and forward projection look fine to me, so the implant needn’t be thick in the center to preserve my current profile. My goal is strictly to improve the front and 3/4 views by widening the lower corners of my chin. Geometrically, I think the new corners should sit slightly wider than my nostrils, but remain inside the corners of my mouth. That’s just my view, but would like to hear from Dr Eppley.
As an international patient from London, I would appreciate clarity on your workflow?A:Thank you for your inquiry and sending your pictures. What you are describing is squaring out the natural shape of your chin but not adding any significant horizontal projection. Certainly a custom implant design can do that very effectively I have done it many times.
From a workflow standpoint:
1) You get a 3-D CT scan in London (we send you the order) which is then sent to me.
2) I created the first design and then share it with you virtually in which we can discuss and finalize the implant design.
3) You come here only for the surgery in which you would be able to return home in 1 to 2 days after the procedure.
4) All follow-ups are done in a virtual manner until I know you are fully healed and have a satisfactory outcome.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Hello, I am sending you this message to obtain the initial opinion of the professor of craniofacial surgery and I am a young man::
.Accurate description of the condition:
Forehead and temples: The forehead from the front is normal, but my head suffers from a severe transverse narrowing that starts from above the ear upwards to the top of the head and downwards to the forehead, and the narrowing is concentrated especially and severely at hairline area, and when looking at my head from above (from the top) the shape looks close to narrow or a triangle, but it is not a true triangle compared to the back of my head which is completely normal and enjoys a normal and healthy width and does not have any defect or structural problems. This anterior transverse deficiency amounts approximately and visually to about 5 centimeters (at a rate of 2.5 cm on each side). I need a fully natural biological solution to increase the width of this area, round it, and give it a real bony texture, and I completely reject fat injection. So what are best and most suitable biological solutions for it from your side?
A:I don’t know what do you mean exactly when you say suitable biologic solution, but if that means an autologous approach (using your own tissues) then there is none. The only effective solution to such head augmentation changes in an adult is custom skull implants.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I am writing to follow up regarding the forehead implant surgery you performed for me. I need to undergo an MRI scan, and I wanted to confirm with you whether it is safe to do so with this specific implant. Are there any precautions I should take, or specific materials I should mention to the imaging technician?
Thank you for your time and guidance.:Both the implant and the screws used for fixation (titanium) are non-ferromagnetic materials which makes them perfectly for MRI scans.You may tell them you have an extracranial forehead implant but that is merely done so they don’t interpret what is there as ‘pathologic’.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Ihave my screws on my head implant is it safe to do an Mri or will the screws heat up. I read titanium is safe. I just wanted to double check Overall I am very happy with everything.
Thank you so much
A: Good to hear from you after all these years and I hope everything is well. For your skull implant you have titanium screws which are non-magnetic which means you are perfectly safe to have any type of imaging to your head whether it be a CT scan or MRI.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I’m 28 years old and I recently found your clinic online while researching cosmetic testicular enlargement.
I have been interested in this type of procedure for some time. Although my testicular size is within the normal range, I have always felt that a moderate enlargement would help me feel more comfortable with my body, improve my self-confidence, and achieve a more proportionate appearance.
My testicular volumes, measured by a recent ultrasound, are approximately 15 ml on the right side and 13 ml on the left side.
I would be grateful if you could provide some information regarding:
* Whether I could be a suitable candidate for this procedure.
* What results could realistically be achieved in my case in order to obtain a natural medium to large appearance.
* How the procedure is performed in your clinic.
* The most common risks and possible complications.
* The approximate total cost of the treatment.
* The expected recovery time.
Thank you very much for your time and I look forward to hearing from you
.A:Thank you for your inquiry and detailing your objectives. In answer to your questions:
1)When it comes to a young male with normal testicle size, which your volumes suggest (about 3.5 cm in length) the most common cosmetic testicular augmentation technique is that of a custom wraparound implant.
2) How much of a size increase the implants could achieve depends on your goals which require it to be put into an actual number (5.0, 5.5 etc). But within reason virtually any size amount as possible since the implants are custom-designed to whatever the patient wants to accomplish. It is not likely that your scrotal capacity be a limiting factor although I cannot past final judgment on that until I know what your exact augmentation goals are.
3) The most common risk of the wraparound testicle implants are infection and secondary dislodgment of the implant from the testicle.
4) recovery time is largely about swelling and its resolution as well as linking your return to all normal physical activities of any strenuous nature… Of which I would say most swelling goes away in 2 to 3 weeks after the surgery and the return to any heavy physical activity would be 6 to 8 weeks after surgery.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I had MMA surgery 12 months ago. Now looking for custom peek implants to restore jawline continuity and improve asymmetry (not looking to make the left and right the exact same measurements, but mirror each other congruently for perceived symmetry/facial balance).
The questions I have are:
1) Do you use custom peek implants or just custom silicone?
2) Is it likely the implant on the right side would be visible or look uncanny (at rest and during movement) since it would be adding height and width through jawline continuity to congruently mirror the left side and restore lost contour from bone loss from the mma surgery? Essentially do you think it would have poor soft tissue coverage, and if so would that likely make the implant visible (exposing ledges of the implant and visible transitions between the mastication muscles to the implant)?
3) I don’t want to add any width or true vertical height to the left side that wasn’t there prior to surgery, but I would like to restore some of the contour that was lost from bone loss and fill in the bsso gap so the jawline is a little more smooth at the bsso plate. Would that be a high risk/low reward for the left side? or a good idea to create better facial symmetry/balance?
4) Since the right side is adding a decent amount of vertical height (guessing around 6mm at the peak deficit) , how likely is it for masseter dehiscence to occur?
A:Thank you for your inquiry, sending your scans and detailing your surgical implant objectives to which I can make the following comments:
1) When it comes to implant material I use whichever material the patient wants provided the material does not limit surgical placement and achieving the desired aesthetic effects.
2) I believe what you are asking about soft tissue coverage over the jaw angles is do you have any increased risk of masseteric muscle dehiscence. That answer lies in the observation that any patient who has had prior jaw angle surgery, weather from an osteotomy or prior implant, where muscle has previously been elevated are at an increased risk of a soft tissue coverage problem. How significant that risk is is going to vary with each patient but it is fair to say that risk is higher thanthe patient whi has had no prior surgery at all.
3) Trying to achieve the minimal contouring effects on the left side is going to be very difficult to do without some added width and height. You can’t make an implant of any material less than 2 mm in thickness so are by definition there is going to be some augmented change minimal as it may be. In just looking at what you have drawl on the left side as your objective I would say leave it alone.
4) I refer you to answer number 2 above.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Do youperform medial z plasty to make eye’s inner corner downturned and if how long it lasts. My concerns are mostly about my area being short and round and little bit feminine .I would want it to be more longer in palpebral fissure length term.I do think it will work in medial canthus in z plasty .but can orbital osteotomies or osteotomies in eye area increase palpebral fissure length such as tripod ,or combined procedures.or is it being performed
A:An inner eye corner Z-plasty is a permanent procedure which adds length as well as turns it downward.
Orbital osteotomies can increase palpebral fissure length primarily in the lateral or outer corner increase.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I feel like my profile is recessed due to a short chin. And from the front my smile is uneven and gummy. I would also like to achieve a more v line chin. Does it make sense to send some photos of other women of the results I’m hoping to achieve? To see if it’s possible with any surgery.
A:Thank you for sending your pictures. You do have a recessed chin in which bringing it forward would add projection. Narrowing the chin bone at the same time would help create more of a V-shaped appearance in the front view. How much of that chin shape that would be seen externally depends on what the thickness of the overlying soft tissues will allow. At the same time a gummy smile correction via a lowering vestibuloplasty could be performed.
In regards to other peoples pictures they are helpful to some degree and they serve as a bit of a guide to determine the patient’s flavor of desired changes. But in the end imaging of your own pictures is what is important to see what is possible as that is actual face we have to work with.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Hi, I saw this posting: https://www.exploreplasticsurgery.com/custom-silicone-implant-replacement-of-a-saline-testicle-implant-comparative-assessmen. Do you have access to and offer the gel filled testicle implants?Are you using the brand from France called Eurosilicone? Can I only get them in other countries? I do not like the saline versions.
Thank you,
A: I have developed an ultrasoft solid silicone testicle implant with a hollow chamber for maximal softness…so it is unlike any other silicone implant.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Can anything be done about the straight line on my scar?
 A:Thank you for your inquiry and sending your pictures. Whether a scar can be improved buy scar revision surgery is highly dependent on its orientation to the relaxed skin tension lines of the face. Your scar, which runs from the mouth corner to the ear lies perfectly along the natural relax contention line of the face. Thus it already lies in its most favorable orientation even though the straight line makes it visible.
A:Thank you for your inquiry and sending your pictures. Whether a scar can be improved buy scar revision surgery is highly dependent on its orientation to the relaxed skin tension lines of the face. Your scar, which runs from the mouth corner to the ear lies perfectly along the natural relax contention line of the face. Thus it already lies in its most favorable orientation even though the straight line makes it visible.
In theory, geometric arrangement of the scar, making a straight line irregular, should make it less visible. But whether it would make it less visible or just create a more irregular scar that makes it more visible is the interesting question and is why scar revision in many patients is a gamble when the scar line lies parallel to the relax skin tension lines.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I am wanting to have my butt either lifted or possible implant and maybe an upper abdomen tummy tightening..wanting to see what I could do to help with my body shape.
A:Thank you for your inquiry and sending your pictures. I do not really any buttock ptosis (overhang of the inframammary fold) so a lower body lift or talk would not seem appropriate. The best approach may be adding the volume to create a fuller and ‘more uplifted’ buttocks. In other words an implant for adding volume would be more effective than trying to lift any buttock tissues to create fullness. While fat injections is the most common form of buttock augmentation surgery due to your prior tummy tuck and perhaps having had some liposuction as well you do not really have adequate fat stores to do so.
Having had a prior tummy tuck it is very common that residual fullness remains in the upper abdominal skin flap. Most surgeons, rightfully so, do not liposuction the upper abdominal skin flap at the time of the tummy tuck. It is safest to do this secondarily where one can be much more aggressive about the fat reduction without any concerns of safety of the abdominal skin flap.
In your case you are a good candidate for what is known as composite buttock augmentation. This is where the placement of intramuscular buttock implants is complemented by the injection of fat in the subcutaneous tissue over it. The combination of both techniques creates the optimal buttock augmentation effect that can be achieved in any single patient. While you do not have enough fat from your upper abdomen and flanks to do true BBL surgery you do have enough fat to be used for layering mfat layer above the muscle at the time as the placement of the intramuscular buttock implants. This technique still creates the profound diametric aesthetic effect seen in BBL surgery where increasing buttocks size and decreasing abdominal fullness creates the best body shape change.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I had a tummy tuck last year. I am mostly happy with the results, but have a small shelf above the scar that doesn’t go away with weight loss. There is also a small dimple at the end of the scar on one hip. The scar is also still very dark and obvious. I was hoping to get some advice on what we could do to reduce these issues. Thank you for any assistance.
A: Many tummy tucks require secondary revision for optimal results. The two most common revision needs are dog years or dimples at the end of the lower abdominal scar line and residual subcutaneous fat fullness above the scar line. The latter is due to the difference in the subcutaneous fat thickness from the upper abdominal skin flap that is brought down and attached to the lower scar line for closure after the wide excision and removal of the excess lower abdominal tissues.
While I cannot speak for your darker scar line since I have not seen any pictures of it but by nine months after the surgery the improvement in the scar is probably not likely.
As a result, based on your verbal description alone you would probably benefit by complete abdominal scar revision with liposuction of the abdominal fat shelf above it. Fortunately such secondary tummy tuck revisions are nothing like undergoing the original procedure in terms of
recovery.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Hi, Im interested in jaw angle implants (custom or stock) combined with a sliding genioplasty. I’ve attached my current profile images along with a simulation of the realistic results I hope to get. I have a long history of allergies that resulted in a class 2 malclussion, so I think hiding the skeletal issues is the best approach since I don’t particularly have functional problems prompted for a BSSO.
A:Thank you for your inquiry and sending your pictures. In looking at your pictures it seems reasonable to do a jaw argumentation with a sliding genio plasty and stock jaw angle plants. I did not see the simulation of your jaw augmentation goals. But until I see them I will assume that it is achievable. Ultimately the questions will be 1) many millimeters of horizontal advancement does the sliding angioplasty need to be and 2) how much jaw angle with should the implants provide. My initial estimation based on the unchanged natural pictures is an 8 to 10 mm sliding genioplasty with 5 to 7 mm width jaw angle implants.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I am interested in a virtual consultation as soon as possible regarding skull contouring. My primary concern is a crown/sagittal ridge prominence on the top-back portion of my skull, along with a shallow depression immediately in front of the ridge.
Based on photo review, I estimate the ridge prominence may be approximately 3–5 mm above the adjacent contour. My goal is to create a smoother crown contour while preserving my forehead shape, forehead slope, facial proportions, and lower occipital contour.
I would like your opinion on whether approximately 3–5 mm of ridge reduction and, if appropriate, 1–3 mm of augmentation of the adjacent depression using PMMA bone cement would create a smoother contour, and what results may be achievable based on CT imaging.
Thank you for your time, and I look forward to your assessment.
A:Thank you for your inquiry and sending your pictures. I would certainly agree with your skull shape assessment of the presence of a higher crown area with a classic coronal dip/valley in front of it to which I can make the following comments:
1) You have a higher crown area, not a sagittal ridge. The difference is the wider shape and broader need for bone reduction.
2) I would not treat the coronal dip with bone cement which is plagued by contour irregularities unless one is going to make a long scalp incision where it can be placed and shaped under direct visual access. I would assume that in a shaved head male avoidance of long scalp incision would be a priority to avoid.
3) The coronal dip is best treated by a custom skull implant in which its shape and contours are assured and it can be placed using a very small scalp incision.
4) I think the real critical decision here it Is do you just treat the coronal dip alone or with crown skull reduction. I make that distinction because to do an adequate crown reduction the scalp incision is definitely going to have to be longer. Whether the length of that scar would be a reasonable trade-off is going to require further discussion.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, here are some current photos of me now and then photos of me before I had my chin implant done as well as aesthetic goals as well. I’ve since had the chin implant removed after it cause fairly severe bone absorption and had a genioplasty to try and repair it but I found its not quite back to the sort of square chin and less rounded nature I have now. I think it looks good but I find it just bothers me still because of the rounded edges and because it isn’t square like how my chin used to be.
A:Thank you for your inquiry and sending your pictures. While a sliding genioplasty can be a very effective chin augmentation procedure the one thing that it cannot do is square out the chin. This is a chin reshaping effect that only an implant can achieve. I have seen your exact situation numerous times and is treated with a custom square chin implant overlay with the greatest emphasis on bringing out the sides of the chin more than the center to create a more square chin look.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I have two questions.
1) With custom Peek infraorbital-malar implants, what is the minimum increase in bizygomatic width in millimeters, and what increase levels do you generally prefer?
2) I have inwardly turned gonions and I want to neutralize them or make them slightly outwardly turned. With custom Peek jaw implants, approximately how much of an increase in bigonial width would be necessary? I don’t want my face to look too wide and blocky.
A:In answer to your questions:
1) The minimum increase in the width of an IOM implant at the zygomatic level depends on the patient’s aesthetic preference. In other words how strong of an effect do they want which is obviously going to vary for each patient. If you define the minimum width as the least amount of material that can be manufactured that would put it in the 1.5 to 2 mm range.
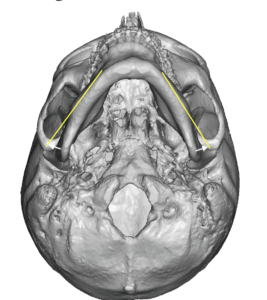 2) By normal anatomy the ramus of the mandible in many male patients turns inward and is not in perfect linear alignment with that of the body of the mandible in front of it. If the goal is to neutralize the inward angulation of the ramus this would be determined on a 3-D CT scan where it can be accurately determined (see attached picture).
2) By normal anatomy the ramus of the mandible in many male patients turns inward and is not in perfect linear alignment with that of the body of the mandible in front of it. If the goal is to neutralize the inward angulation of the ramus this would be determined on a 3-D CT scan where it can be accurately determined (see attached picture).
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I have two questions. Will a subnasal lip lift get rid of the overhang that I keep biting? Will rhinoplasty make the tips of my nose less droopy when smiling?
A:Thank you for sending your pictures. A subnasal lip lift will certainly shorten the distance between the base of the nose nx the upper lip. However it’s lip lifting effect is unlikely to significantly elevate the lower part of the lip in which you are probably biting. There is not a one-to-one correlation between the amount that the lip is listed under the base of the nose and how much the bottom part of the lip lifts. Therefore if that is a significant concern you may need to consider doing some mucosal resection on the inside of the lip at the same time as the subnasal lip left to reduce or eliminate that problem.
When it comes to the rhinoplasty it is important to recognize that this is a static procedure not a dynamic one. Meaning it’s effects are best seen in a static or nonsmiling posture. What the effects of a rhinoplasty procedure may do when you are smiling is completely unpredictable. Thus you would only consider a rhinoplasty for what his benefits would be in the static position for their overall shape of the nose. Should there be any inadvertent benefit to your smiling concerns that would be considered a bonus and not an absolute expected sequelae of the surgery.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Hello, I am wondering which surgery would be helpful for me. I am 99% sure I would be a good candidate for sliding genioplasty, specifically targeting the vertical length, as I feel I suffer from slight short face syndrome, as well as having a deep labiomental fold and a long philtrum. That is why I am not considering implants, as I feel I have good side chin projection; it’s just the vertical length that I would like to increase. I have included pictures of my overbite as well. On a side note I am completely open to what you think would help as well
A:Thank you for your inquiry and sending your pictures. You’re absolutely correct and that you have a vertically deficient chin. You have adequate horizontal projection but between your overbite, flat mandibular plane angle and shorter lower third of the face vertical lengthening is your chin need. You’re also correct in that in a vertical opening bony genioplasty is the correct solution. The only debate to be had about it is how much vertical lengthening is needed, and it is probably in the 6 to 8 mm range, although this is yet to be more fully investigated buy imaging.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, My shoulders aren’t that narrow, so I wouldn’t need more than 15mm-20 mm of increased clavicle length to get to my goal. I just would like to discuss the postoperative journey after and actual risks. And if any of your precedent case was able to get back to 100%
A:Based on the degree of change that you feel you need those shoulder lengthening goals are the limits of what clavicle lengthening can achieve based on current techniques.
Whether it is shoulder reduction or shoulder lengthening the postoperative recovery protocol is the same. I put patients on gradual increase of arm movement over a six week. At which point arm motion should be fairly normal. When it comes to strenuous activity this is delayed until three months after the surgery to allow for more complete bony consolidation.
Like all aesthetic clavicle surgery the primary risk is fixation failure and a nonunion. These risks are a bit greater in shoulder lengthening then they are in reduction. The key to lowering these risks shoulder lengthening is to not try to exceed the 15 to 18 mm lengthening that usually can be achieved.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I am concerned that if he litigates one artery, it’s going to cause another one to be enlarged. If that is the case, will he know exactly when he like one artery if the other one is going to be enlarged? And if so, can he undo the one that he located if that’s the case? Also, after the procedure, we noticed that there is one that is enlarged and I am unhappy with it. What can we do at that point? I just want to know what a Plan B with be. How would we do a repair if that’s the case? Thank you so much. Please let me know
A:In my extensive experience with treating prominent temporal arteries through a multi ligation technique I have never seen new arteries develop in the area that aren’t associated with the temporal artery.. In a minority of cases it is possible to have some ‘recurrence’ of its prominence, although very uncommon, but that should not be confused with new arterial prominences developing.
In the few instances in which I have seen some recurrence of the temporal artery Monster years later it is simply a matter of adding a few more ligation points.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Fourteen years ago, I underwent a procedure in which calcium phosphate bone granules (β-tricalcium phosphate) were placed in a subperiosteal pocket over the zygomatic region of my right cheek. A fixation screw was also used. Since then, I have experienced persistent facial asymmetry, a visible and palpable bulge, chronic tension in the surrounding muscles (masseter and temporal region), and ongoing discomfort that has significantly affected my quality of life. Given the duration of the implant and its subperiosteal location, I am particularly interested in your experience with the removal of these types of structures. I recently obtained a high-resolution facial CT scan (0.5–1 mm cuts) focused on the zygomatic region. The doctor who reviewed the scans noted the following: • The imaging shows persistent calcium-based particulate material located superficially to the zygomatic bone. • Importantly, the underlying bone itself appears intact, without destructive changes or aggressive remodeling. • The material does not appear to have fully integrated into the bone, but rather presents as clustered granules embedded within the surrounding soft tissue. (I have attached screenshots with arrows indicating the particulate matter.) • This appears consistent with long-standing β-tricalcium phosphate that has only partially resorbed and is now embedded within fibrotic tissue. • The findings correlate with my clinical symptoms, particularly the fact that firm manual pressure temporarily improves the facial symmetry. The reviewing surgeon suggested that a reasonable next step may be a surgical approach aimed at relieving the mechanical effect of the material. This would involve re-entering through the original intraoral access, with the possible addition of a subciliary approach (under the eye) if necessary. The proposed plan would include removal of the mobile particles using a burr or other instruments, removal of the fixation screw, and release of the surrounding fibrotic tissue. He also mentioned that a midface suspension procedure might be required if extensive fibrosis is encountered, in order to prevent descent of the tissues during healing. In that case, bilateral treatment might be necessary for symmetry. Whether the procedure would involve partial or more complete removal would ultimately depend on the intraoperative findings and the degree of adherence of the material. Any remaining contour irregularities could potentially be addressed later with conservative fat grafting after the tissues have stabilized. Could you please let me know whether, based on your experience, it may be possible to remove these granules and improve the associated fibrosis and asymmetry? Do you have experience with these kind of surgeries? Please find attached screenshots from the CT scans, with arrows indicating the particulate material. Thank you very much for your time and consideration
A:I have removed HA bone cement many times. Given the method by which it was placed, intraoral,and in the scan showing it sits in the subzygomatic position it should be able to be removed completely through an intraoral approach. I would like the outcome of its removal to determine whether any soft tissue suspension is needed, which I doubt, and when you’re dealing with a problem be certain that you don’t create any new problems by doing a concurrent procedure which has its own set of risk and complications and whose need is completely unknown.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Hi! I wanted to know if I could get some advice on what the best route would be for getting my chin fold removed. I have a pretty deep fold and paired with my thin lips it doesn’t look attractive at all. It’s my biggest insecurity. I was just wondering if fat grafting would be the best permanent option for me or if I should try something else instead? Any feedback is greatly appreciated. I have also attached an AI generated image of the result I would like to have
A:You have a deep labiomental fold for two very specific reasons. First you have an over projecting chin with a large soft tissue chin pad. With excessive horizontal projection even a normal labiomental fold is going to look deep. Secondly the labiomental fold is very highly positioned very close to under your lip which is also a direct reflection of the large chin projection. In essence this is a chin projection problem not really an isolated labiomental fold issue. The correct approach needs to be hey Chin reduction
involving both bone and soft tissue chin pad done through a submental technique.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, considering the two options, I feel that testicle implant displacement is what I’ve been considering most. Where I am less sure is what size I would be happy with.
A:Aesthetic happiness is a personal objective. Effectiveness of the technique is the only definitive measured outcome I can comment on. As a general guideline for the displacement technique you want the custom implants to be at least 70% or more larger in size than that of your natural testicles. So for example if your natural testicles are 3.5 cm in size that means the very minimum size you should have for succesful displacement is 5 cm and I would probably hedge that up to 5.5 or even 6 cm to be certain they are ideally effective.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Male with prominent iliac crest . I am a 51-year old cis male interested in the iliac crest reduction procedure. Assuming no medical conditions or concerns revealed in a physical examination or in x-rays, would I be eligible for this procedure, given my age?
A:From my perspective age really has nothing to do with whether one can have iliac crest production. The question is not a chronological one but that of effectiveness….meaning I would need to see some pictures of your hips to determine if you are a good candidate for the procedure.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, Can the dip across the top of my head be treated by bone cement?
A:Thank you for your inquiry and sending your well illustrated pictures of a classic coronal dip skull indentation. This is best treated by a custom designed implant rather than bone cement. A custom skull implant can be placed through the smallest incision (;ess than 2cms, it also provides the best material transition into your skull bone to avoid any external visible edging. In the shaved head mail even the smallest edge transition can become visible. Bone cement performs very poorly in these regards.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I am writing regarding aesthetic hypotelorism and orbital/midface asymmetry. My measurements are approximately: * IPD: 57.5 mm * ICD: 27.5 mm * Eye width: 28 mm * Bizygomatic width: around 133 mm My main concerns are: * slightly close-set eyes relative to my facial proportions and midface length * left-sided orbital/zygomatic recession and asymmetry * downward curvature/scleral show of the left lower eyelid * deviated nose, likely related to the asymmetry I previously consulted another surgeon who proposed a traditional 360-degree transcranial orbital box osteotomy, but after researching the coronal/craniotomy approach and its morbidity, I no longer feel comfortable pursuing that route. I found your discussions regarding the modified subcranial/inferior 180-degree orbital box osteotomy and wanted to ask whether my case sounds potentially suitable for that approach instead, since my desired increase is relatively modest (approximately 4–5 mm total IPD increase). I would also like to ask: * how much true IPD and ICD increase can realistically be expected from this procedure * whether the procedure produces actual globe movement or mainly orbital framing/perceptual widening * whether you have before/after cases of patients with similar measurements/goals * what the lower eyelid and infraorbital nerve risks are in your experience * whether custom orbital rim/malar implants, canthoplasty, and septorhinoplasty could potentially achieve most of the desired improvement without orbital osteotomy. Thank you for your time.
A: The only truly effective procedure for increasing the IPD 2 – 3mms per side is 360° orbital box osteotomies. But as you have appropriately determined the potential trade-offs of the procedures are not worth its benefits. This then raises the question as to whether a lesser degree of orbital box osteotomy could be effective. It possibly could but requires a 3-D CT scan to look at the orbital anatomy, evaluate bone cut location etc to provide a more qualified answer.
Certainly building up the rims and cheek area with implants is not going to be helpful and will likely worsen the appearance of the current eye spacing.
A rhinoplasty is only helpful to create the illusion of an increased IPD if significant nasal bone narrowing is needed. This is clearly not needed in your case.
Dr. Barry Eppley
Plastic Surgeon