Your Questions
Your Questions
Q: Dr. Eppley, I had a question regarding a potential facial fracture I was hoping you could answer.
So back in January I took a couple falls after drinking a little too much. There wasn’t any terrible pain or obvious swelling, however I did have a lingering feeling in the mid face for several months. Additionally, I feel as if my face looks less symmetrical, although there is no obvious deformity.
I was wondering whether I could have fractured something in my face despite not having the obvious symptoms of a fracture? Additionally, would imaging show a theoretical fracture even if the incident happened 7 months ago? This has been bothering me a while, and I’m unsure whether an imagine/exam would be able to confirm whether I had a break? Thanks for reading,
A: In answer to your facial fracture questions:
1) It would be very unlikely to have had almost any form of a facial fracture without some swelling/bruising or other physical evidence that it had occurred.
2) Even if some small fracture line had occurred, it would likely not he evident any longer in a typical x-ray. What may appear in a 3D CT however would be any evidence of an area of depression or abnormal shape that resulted from the fracture which would be most relevant in the midface where the thinnest bones on the face exist.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m a young student thinking of getting a genioplasty for my weak lower jaw. I’ve spoken to an orthodontist who recommended either a genioplasty, or more extensive lower jaw surgery. I’ve attached the diagnostic records from my orthodontist’s office. I’d welcome any recommendations for improving my appearance as I don’t have very good judgment with these sorts of things. For now, my priority is fixing my lack of chin projection such that my face looks more balanced/harmonious, as my chin and lower third seems disproportionately smaller than the rest of my face. I also have a few questions:
Would a genioplasty be appropriate for me? Could you provide a quote? When would be the earliest I could get the surgery? I have dislocation of my TMJ and some pain/fatigue of my TMJ– would this warrant jaw surgery with braces or would that not make much of a difference to my TMD? If I were to travel to Indianapolis for surgery, when should I plan to fly back home after the surgery?
Thank you. I look forward to hearing from you.
A:Thank you for your inquiry and send your pictures and orthodontic records. In answer to your questions:
1) With a Class II malocclusion and TMJ symptoms a solid argument can be made for a functional procedure like the sagittal split lower jaw advancement. While there is no guarantee that it will cure your TMJ symptoms it at least offers the potential for improvement while a sliding genioplasty does not.
2) As a young patient that probably needs a 10 to 12mm horizontal advancement the sliding genioplasty is a good procedure. With a naturally more square chin there are not the typical concerns about creating a chin that is too narrow afterwards.
3) I advice attached a side view image of one potential type of chin projection change.(more or less can also be done)
4) My assistant will pass along the cost of the surgery to you on Monday..
5) You would return home either the next day or no later than 2 days after the surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hey I really like the custom implants you have available. I’m looking for something to augment my jaw angles, and change my chin in three dimensions. I’m also looking to obtain high cheekbones that are prominent in terms of width and length along with some type of under eye support like an infraorbital extension. Now I don’t know if all of these are necessary to achieve the look I desire, it’s mainly to make my face more masculine and to achieve the hollow look. I currently have a few questions, if I were to decide to do my surgery with you the process of manufacturing these implants takes around three weeks from what I’ve read, now does the surgery take place during this time or is it scheduled for another time in the far future?
A: Thank you for your inquiry. To help you determine if custom cheek and jawline surgery can achieve your desired facial changes I would to see some pictures of your face for computer imaging purposes. From a logistical standpoint, custom facial implants are made from a 3D CT scan that the patient gets where they live. Once the scan is received it takes an average of 6 weeks to got through the design process and have them ready for surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is it possible to look half ~ fully caucasian with a custom brow bone and nasal ( possibly chin ) implant and a blepharoplasty with the goal of making the eyes look as white as possible? My cheekbones are relatively high and wide and I have little to no facial recession.
A: Thank you for your inquiry try and sending your picture. I am not completely certain how one would define or judge what ‘half Caucasian’ as that is open to personal interpretation. But I think we have to realize that your facial canvas is Asian and that surgery may influence that to some degree but I have yet to see where a major change in facial appearance occurs no matter how the facial structure is changed. It is probably fair to say that you would end up somewhat less Asian but that should not be confused with being seen as partially Caucasian. The procedures you have mentioned would be the correct ones in that type of facial reshaping effort.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to inquire about scar revision in chin implant revision problems. I’ve had multiple unsuccessful Medpor chin implant surgery from the intraoral incision. Now it’s almost a one-year postop, and I have scar contracture both mucosa and under the skin.
Basically, the web banding inside the month feels very uncomfortable/stretching. The scar tissue (capsule) between the skin and the implant feels very thick, thus making the skin less pliable, which is especially evident when I make facial expressions.
Though I know each surgery is invasive and creates scar — is there any way to revise the scarring issue? Is that possible to release the intraoral mucosa scar (sth like z-plasty/v-y closure), excise the capsule, and change for a sliding genioplasty (which eliminates the recurrence of thick capsule)?
I’m a little confused, as I heard some surgeons said the new scar will always tighten after any surgery, and some surgeons said it’s not hard to revise the scar/excise the scar and make them feel comfortable. I would like to hear your opinion since you’re considered an expert in chin revision surgery. Will the scar revision surgery make things worse? Thanks, and I’m looking forward to hearing from you.
A: When you have scar contracture, tightness, fixed immobility and otherwise chronic discomfort, you are not going to improve the problem by shifting or rearranging the scarred tissues by any scar revision technique. The problem is lack of good tissue quality AND quantity. You have to add back new unscarred tissue into the chin implant revision surgery after release and/or excision of scar tissue. This is basic plastic surgery 101. Whether that is done by injectable fat grafting or the open placement of en bloc solid fat graft can be debated but the key is tissue recruitment. Every surgery does create scar tissue but it can also add new tissue as well.
Whether this should be done with the existing chin implant in place or removed and replaced with a sliding genioplasty depends on other factors not yet known to me.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I read your article “Plastic Surgery’s Did You Know? Fat Atrophy after Trauma”. I bit my lip quite hard a few months back and now have atrophy at that area. Does atrophy resolve itself without intervention, and if so, how long does this take?
Please let me know,
A: Once fat atrophy occurs the fat tissue is not going to regrow…the fat cells are lost. But time will answer that question. But after six months if the lip indentation persists it can only be improved by fat grafting to replace what has been lost.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m wondering if you could be so kind as to help provide me with an opinion as to one aspect of my surgery.
My surgeon is proposing a standard Lefort 1 movement of my maxilla. However, I’m not convinced this will adequately address what I perceive as the deficiency in my midface (cheeks/nose).
Does you have a view on this and what the other options might be? I appreciate it may be difficult to say for certain based only on photographs
Thank you for your help. I’m just looking to get as much info as possible at this stage.
Kind regards,
A: As a general statement a LeFort I osteotomy moves the lower third of the midface that contains the alveolar bone and teeth. While there can be some midface aesthetic benefits with forward movement, they are going to be limited to the base of the nose and upper lip. How significant those effects would be depends on the amount of horizontal movement. But anything less than 5mms will have a negligible effect in that regard. In short most LeFort I osteotomies are done as a functional operation that corrects malocclusions. (minus bimaxillary osteotomies for sleep apnea) They can have some limited aesthetic benefits with significant anterior movements. But such benefits are a byproduct of the operation not its primary intent. Midface implants are more effective because they specifically target the desired areas of augmentation and are not dependent on where the underlying teeth are located.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m a huge fan of your work! I am considering two procedures and was hoping to learn more about their logistics, including price, transportation, and recovery. General advice on whether these surgeries are appropriate would also be greatly appreciated.
First, I want to get a sliding genioplasty to increase both the vertical and frontal projection of my chin. Second, I want to get some form of enhancement to add lateral width and overall thickness to my cheekbones. I am intrigued by your “model cheek” implants with long emphasis on the zygomatic arch. However, I have some concerns with implants and was wondering if a zygomatic osteotomy could achieve similar results. I am looking for 5-6mm of augmentation on each side, which I anticipate will look harmonious with an increase in chin length from the genioplasty. I am also hoping the cheek augmentation will provide an upwards lifting effect on the tissue on my face.
So, in conclusion, are these reasonable expectations/desires for surgery?
A: Thank you for your inquiry, sending your pictures and detailing your concerns/objectives. In the spirit of an autologous facial augmentation approach, both the sliding genioplasty and zygomatic sandwich osteotomies (ZSO) are effective procedure for chin and cheek augmentation. The sliding genioplasty is well known and the only aesthetic question are the dimensions of change. (how much forward and how much done) The ZSO is the only autologous option to the extended cheek implant but it will not have the identical aesthetic effects as the bone can never be removed with the same magnitude in the same locations as the onlay augmentation provided by an implant.
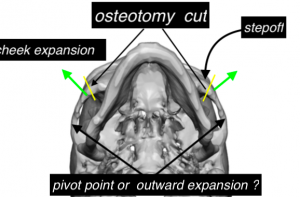 The ZSO works by expanding out the posterior bone segment right behind an osteotomy line which is vertically cut through the main body of the zygoma. This allows the anterior arch/cheek to move outward. This adds lateral cheek width although the step off has to be managed for any more anterior cheek fullness. The traditional ZSO does not move out the posterior arch, which limits how much of the arch is seen as it moves posteriorly, but that can be moved out as well if the full arch effect is desired.
The ZSO works by expanding out the posterior bone segment right behind an osteotomy line which is vertically cut through the main body of the zygoma. This allows the anterior arch/cheek to move outward. This adds lateral cheek width although the step off has to be managed for any more anterior cheek fullness. The traditional ZSO does not move out the posterior arch, which limits how much of the arch is seen as it moves posteriorly, but that can be moved out as well if the full arch effect is desired.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had Sculptra injections to restore mid-facial volume and help correct nasolabial folds. The lower face/jaw was not supposed to be touched, heaviness in front of ear to chin under my cheek bone (if you can still see my cheek bones). Attached is a front/right/left side photos of today.
A: Thank you for sending your before and after facial pictures. What I would say is that in general the injected material did what it was supposed to do…fill out your face. But it is just too much of a good thing so to speak. You really have two options at this point:
1) Wait it out until the Sculptra eventually absorbs. It may take 12 to 15 months but it will eventually happen.
2) Through facelift incisions excise the thickened scar tissue over the undesired areas of the lateral face and jaw angles.
While options #1 is not very time efficient it is the non-invasive and will be effective. Option #2 while effective is invasive but is more time efficient.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I train boxing/mixed martial arts. Once a chin implant or sliding genioplasty was performed, would I need to stop boxing permanently? Would a punch to the face with gloves on possibly damage or dislodge an implant?
A; While I don’t think that would damage a healed sliding genioplasty, there is a low level of concern with that of the chin implant. (which is why they are screwed in) It is a common question I get but I have never yet heard of an actual chin implant being displaced by trauma. Like many things in life, there are risks in doing them and you just have to calculate whether the risk is worth it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a transgender man with several body contouring questions:
1) Would it be possible to reduce the female pevis area in such a way that it is similar to a male pelvis? (Iliac crest reduction, Q angle reduction, etc.)
2) Is it possible to widen the shoulders at all?
3) How effective is liposuction of the saddle area for those transitioning from female to male? I’m struggling to find results of this as those who receive liposuction to their hips don’t tend to go as far as I would be wanting (as far as possible)
4) Have you had Female to Male patients in the past and if so, could you share some of the procedures they typically have to result in a full transformation as well as other procedures you would recommend?
5) I have ptosis with both of my eyes and will be needed upper and lower belpharoplasty and I am wondering if it is possible to lower the eyebrows during this? I have two other family members who have had blepharoplasties, however, they both received brow lifts. Does this procedure naturally lower the eyebrows if you do not ask for a brow lift?
6) How far can the width of the face be reduced? I would say I have very wide cheekbones though I think it may be my head in general as I also have a wide lower jaw. I understand there is jaw shaving for the lower part but what about the eye / under eye section of the face?
Thank you so much for your time, I very much appreciate it.
A: Thank you for your inquiry. In answer to your body contouring questions:
1) The iliac crest bone can be reduced at its widest mid portion. It may also be possible (although I have not done it as no one has requested it) to reduce the anterior superior iliac spine which is what I think you are referring to when mentioning the Q angle.
2) Shoulders can be widened by three methods including deltoid muscle fat grafting, deltoid muscle implants and clavicular bone lengthening, each with their own advantages and disadvantages.
3) Saddle bag or outer/upper thigh liposuction is commonly done. But you are not likely to find a straight line result as that is not how it is commonly done in cis-females. (over correction) Whether you would be able to a achieve a straight line result with aggressive liposuction depends on the fat component of your saddle bag areas.
4) Regardless of the direction of the gender change every patient has different needs and different levels of effectiveness with various procedures. Each patient has to be assessed for what procedures would have the greatest value to their gender transitioning. In the face as well as the body computer imaging is very helpful in making these determinations.
5) An upper blepharoplasty will not lower the eyebrows. Actually there is no surgical procedures that can lower the eyebrows short of creating more forehead tissue through tissue expansion.
6) Facial width reduction is most commonly done by cheekbone osteotomies and lower jaw shaving/ostectomies.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Do standard implants placed after genioplasty have a higher rate of infection/complications (such as erosion, shifting, or poor fit) compared to a standard implant placed on a non-augmented chin? Would a custom implant be preferential in my situation based upon these factors, or would it be more of a personal/aesthetic preference instead? In general, are custom implants less prone to shifting/erosion/infection than off the shelf implants in your experience?
Thanks for the help!
A: The value of custom facial implants (including custom chin implants) is in their ability to create a type of chin augmentation effect that otherwise would not be possible with standard implants. Because of the custom design process they may be less prone to intraoperative malpositioning because features can be built Into them are useful for placement in surgery. Otherwise they share all other similarities with standard implants.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I feel like I have a weak chin that makes my nose look out of proportion with my face. I was curious to know how i could fix this with a sliding genioplasty or with a chin implant. Also the amount of movement (if its sliding genioplasty) and the rough cost?
A: The key decision in whether a chin implant or a sliding genioplasty is preferred is based on the dimensional requirements needed for the desired chin augmentation effect and the patient’s emotional affinity for one vs the other. For men the key defining dimensional issue is often chin width. (and that is certainly true in your case as the horizontal need can be meet by both methods and you need no vertical lengthening) Does you want to keep the current chin width or make it wider or more square? Only a chin implant can make it wider/more square as a sliding genioplasty may even make it a bit more narrow.
As for the amount of horizontal augmentation that is determined by computer imaging as well as preoperative measurements which becomes most relevant when a surgery date is planned.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was wondering for the clavicle lengthening surgery does a patient need to have straight shoulders for this surgery to be possible? I notice clavicles are either straight or sloped. I was wondering if this effected anything and if it mattered. Thanks.
A: The shape of the clavicle does not matter as no clavicle is perfectly straight. All clavicles are s-shaped. The portion of the clavicle that is cut, bone grafted and plated, however, is straight.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m interested in a buttock reduction. I’ve always had large buttocks growing up and during bodybuilding squatting has attributed to that. I don’t work out anymore. If possible I’d like to have a much smaller and flat buttocks. I’ve read Vaser and skin removal is the process. However are there any dangers around the gluteus that would occur during this surgery as I know BBL surgeries have risk of fat embolism and if there’s muscle around my gluteus I assume this can not be removed?
Thank you
A: Thank you for your inquiry and detailing your buttock reductions goals. You are correct in that reduction of buttock subcutaneous fat and a lower buttock skin tuck are the only surgical techniques that can be of benefit. Buttock or gluteus muscle is never removed. Buttock liposuction has no medical concerns unlike BBL surgery in which fat is injected under high pressure into the muscle. (which is not done anymore) Liposuction is the reverse, it is removing fat. Its only concern is of an aesthetic nature which applies to liposuction anywhere…the risk of contour irregularities which may be more prone on the buttocks with aggressive fat reduction. The skin removal/tuck certainly helps mitigate to some degree that aesthetic concern.
Whether buttock reduction may be effective for you depends on what your buttocks looks like and how much fat there is at the subcutaneous level.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a slightly recessed jaw and chin. I might get jaw surgery in the future but I can’t afford it right now. I was wondering 1. Are chin implants and genioplasty the only surgeries for chin you offer? 2. Could I get a genioplasty and then get jaw surgery in the future? 3. I have just discovered chin fillers, and was wondering if they could make your chin wider or do they only increase project?
I could tell by comparing pictures and looking at other results online I would only need one syringe for a chin filler. What I am worried about is my chin looking too narrow after a filler, so I was wondering if they could increase width or do they only increase projection.
A: Thank you for your inquiry. In answer to your questions:
1) The available chin augmentation procedures include synthetic fillers, fat injections, implants and osteotomies. (sliding genioplasty)
2) A bony genioplasty deos not preclude jaw surgery in the future…although that depends on how much the chin is moved forward and how much the lower jaw needs to be moved later.
3) Injectable fillers can create any chin dimensional change…if you use enough filler volume. It is fair to say that both increased horizontal projection and chin width will likely require more than one syringe of filler.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I think I want thigh lift only whether it’s a mini thigh lift with some liposuction or full thigh lift. Please give me estimate price for both. Can’t wait to hear back from you. Thanks!
A: Thank you for your inquiry and sending your pictures. Thigh lifts in patients that look like you are very tough in my opinion in regards to the decision to trade into a scar given the amount of loose skin and skin quality that you have. Thigh lift scars in general do fairly poorly in most people because they are incisions closed under tension and are placed vertically which is perpendicular to the relaxed skin tension lines of the leg. (a recipe for poor scarring)
Like many types of extremity lifts (e.g., arm lifts, thighs lifts) the scarring does best in patients who have undergone large amounts of weight loss and the skin is very loose and stretched out. In people with much better skin quality who are not weight loss patients (you) the scarring will not be good as all. Thus I would be very cautious about considering this operation and I would certainly not dive right in. (full vertical thigh lifts) At best liposuction and a limited upper thigh lift would be the most you should consider. (and even that I cannot really endorse based on the pictures you have submitted)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I read an article you posted about ear surgery using metal inserts instead of rib grafts. Do you do this surgery? Please let me know. I am very interested in this surgery to bring my ears out about 5mm but I would rather not do a rib graft. Thank you!
A: Thank you for your inquiry. You are referring to a subtotal otoplasty reversal for over corrected ears. The key to the procedure is that the released cartilage must be held out by an interpositional piece. Initially I used a small bent metal plate. (which is the article to which you refer) That works fine but I have evolved to using tissue bank rib cartilage which I think works even better. No one wants to have their one rib harvested for the procedure.
Dr. Barry Eppley
Indianapolis, Indiana
Can A Custom Infraorbital-Malar Implant and Custom Jawline Implants Be Done During The Same Surgery?
Q: Dr. Eppley, Hi, I saw that you design Custom Infraorbital Malar Implants. It said it helps get rid of sclera show, but is this implant also part of Infraorbital rim implants?. Like does this implant also help with hollow and poor undereye support while at the same time giving the high cheekbone look?. And can this implant be inserted at the same time of a custom jawline implant?. What would be the approximate range of cost of a infraorbital malar implant+ custom jawline implant?
A: As the name implies, a custom infraorbital-malar implant provides augmentation of the infraorbital rim in both vertical and horizontal dimensions as well as can extend out onto the cheekbone and back along the zygomatic arch. This unique implant design simultaneously treats both undereye hollows as well as gives a high cheekbone look. It is common to place both custom infraorbital-malar and custom jawline implants during the same surgery. Such a combination is a well known male masculinization procedure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, One month ago I had a chin implant (submental approach) and I’m thinking of having a buccal fat pad removal procedure done. Is there any risk an infection related to the fat pad removal procedure could infect the chin implant? Basically, could an infection from the buccal fat pad removal spread to the chin implant, resulting in me having to remove the implant?
A: Thank you for your inquiry. I see no association between a buccal fat pad space infection (should that occur…but have never seen it yet) and infecting an indwelling chin implant. The buccal fat space is in a completely different anatomic tissue plane than a chin implant. Thus an infection of one can not infect the other.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a French Canadian adult and I suffer from plagiocephaly. My right side is relatively flat. The method of injecting bone cement by small incision really interests me. I wanted to know if you could help me find a specialist in Canada to perform this surgery.
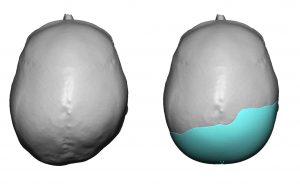 A: Thank you for your inquiry and describing your right occipital plagiocephaly concerns. While once done using bone cements placed through somewhat smaller scalp incisions, that technique has been replaced by custom made skull implants which are placed through similarly small scalp incisions. Custom implants produce far superior augmentation results that cover more of the flattened areas and assure a smooth convex surface with a very low risk of revisional surgery. (which is unlike bone cements) I can not speak for whom if anyone performs this type of skull reshaping surgery in Canada. (which I highly doubt)
A: Thank you for your inquiry and describing your right occipital plagiocephaly concerns. While once done using bone cements placed through somewhat smaller scalp incisions, that technique has been replaced by custom made skull implants which are placed through similarly small scalp incisions. Custom implants produce far superior augmentation results that cover more of the flattened areas and assure a smooth convex surface with a very low risk of revisional surgery. (which is unlike bone cements) I can not speak for whom if anyone performs this type of skull reshaping surgery in Canada. (which I highly doubt)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Glad to hear it’s something possible with iliac crest reduction and upper hip augmentation. Attached are current photos of my hip area as well as what my goal would be with the procedure. Looking forward to your thoughts.
A: Thank you for sending your pictures and the ideal goals. We understand these ideal images are the general idea which is really iliac crest/waistline reduction and upper hip augmentation. (that is bit more than just a hip dip augmentation. You appear to be correct in that the limiting factor in the lower waistline area is the iliac crest bone. Certainly the approach of aggressive liposuction of the waistline/iliac crest area to thin out the soft tissues, some iliac crest bone reduction and hip implant augmentation would be needed to try and affect some similar type of change which I have imaged. (attached)
There are two approaches to the above:
1) Do liposuction and fat transfer to the hips first and see what type of change you can affect by this standard approach. (it would be needed anyway so the effort is not lost) Then if needed the iliac crest bone reduction and hip implants can be done as stage two.
2) Do #1 with iliac crest bone reduction and hip implants.
Obviously #1 is the conservative approach (which is not always a bad thing) and #2 is the aggressive approach.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am planning of chin implant replacement and a submentoplasty procedure with you next month. I have some questions about the chin implant to be sure not will be better after the replacement as well as what changes in the neck that may occur.
A: Thank you for sending your side profile picture to which I can make the following comments:
1) If my memory is correct I have seen an MRI of current chin implant position which shows it hanging off of the end of the chin bone. Thus we know for certain that a new chin implant that is less bulky can be placed in the proper position on the bone which makes for an exclusive horizontal type of chin augmentation effect. Because of the existing chin implant and to ensure that it stays in the higher desired position, this is the role of double screw fixation of the implant.
2) Your neck is very typical for some middle-aged men who have thicker tissues creating a low hanging full neck with an indistinct cervicomental angle. While we know the best result possible comes from a full lower neck-jowl lift, most men are not prepared to go that far. (extent of surgery and ear scars) Thus the submentoplasty procedure has been chosen as it offers the most that can be achieved short of a full lower facelift. The result will not be the same but then the extent of surgery, recovery and risk factors will accordingly be lower. There is no question that the neck part will have the biggest aesthetic benefit but it is important to appreciate what the submentoplasty can and can not do.
3) I have attached an imaging prediction of what I think the likely outcome will be from these two combined procedures.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have facial asymmetry which has impacted on my self esteem for the most part of my life. I wondered if it was possible to treat and if so what procedures it may entail. I was researching v line surgery to have a more symmetrical, balanced and feminine face shape. On the pictures you can see one of my jaw bones is more square and the other more rounded. The rounded side is the side of my face that is wider. I prefer the square jaw on the side where my chin is over to.
Thank you for your time.
A: Thank you for your inquiry and sending your pictures. Your jawline asymmetry, by description and as illustrated in the pictures, has a left more square jaw angle, wider rounder right jaw angle and chin asymmetry. While a jawline reshaping procedure would be indicated, any form of traditional v line surgery would not be appropriate. I think you mentioned that approach with the intent of the result, not in how the surgery would be done. Since the one corner of your jaw is good (left square jaw angle), it is the other two corners of the jawline that need to be changed. The right jaw angle would be reduced in width by burring and a very small jaw angle implant ‘cap’ but one it to make it just more square. The chin bone would be moved to the right to put it into the midline. Before surgery a 3D CT scan of your jaw should be done to fully visualize the bony anatomy and plan the surgical changes.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m curious about a forehead implant. I am a young male and I look very young for my age, I have a round & sloped forehead and while I don’t dislike the slope I think the roundness gives me a childlike appearance. I’ve seen forehead implants that created a rounder less sloped head & i’m curious if it’s possible to create a custom implant that would create a flatter forehead. I still would prefer it to be somewhat slopped just flatter. Thanks
A: Thank you for your inquiry and describing your forehead reshaping objectives. One of the main advantages of any custom facial implant, including a custom forehead implant, is that they can be designed any way the patient wants. So having a forehead implant design that creates a flatter and less sloped forehead is certainly possible. As a general rule it is usually not a good idea to have a completely vertical forehead anyway for a variety of aesthetic reasons.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’ve ripped my tragus piercing, I think on the first or second night of getting it I must have slept on it and pulled it downwards. My piercer suggests switching the hoop to a bar but I can’t see the point if it has already been torn. I’m also concerned with how this hole will heal, whether the hole will heal itself and only be a lined scar or whether the hole will always be present.
A:I am confused between this picture and your description as to your tragus ear piercing concerns. By definition such piercings will always heal and end up as an epithelial-lined skin tract. Thus it will always be a hole through the cartilage. So a ‘lined scar’ and ‘the hole’ by your description are one and the same.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Here are some more rib removal questions after our consult from last week.. Could I get hurt physically from something injuring me in the future from wrestling etc from having rib removal? Do you think that rib removal has more or less complications than a butt augmentation? How painful is it compared to a butt augmentation? Do you think by taking the LD muscle out that it will cause better shape to my bodybuilding frame? And not take away from my lats? And not hurt my muscle when lifting? Can liposuction make my skin less tight? Is there anything that I can do during this procedure to tighten my skin in the abdomen and back region? Could removing my ribs hurt me when I am.older?
I also forgot to ask I have heard that removing the 10th rib can cause less balance coordination and exposure to the organs ect . Are my organs safe after this procedure? I apologize for all the questions
Thank you so much.
A: In answer to your rib removal questions:
1) I do not think wrestling exposes you to any increases risks of injury after rib removal surgery.
2) Rib removal has far fewer potential complications than any form of buttock augmentation, particularly that of implants. I have seen lots of complications from buttock implants but never one yet from rib removal surgery. Compared to intramuscular buttock implants rib removal surgery is less painful and with a quicker recovery.
3) Shaving of the lower outer border of the LD muscle improves the results from rib removal surgery but will not affect lifting thereafter in any way.
4) Liposuction will not make skin more loose…unless it is very loose initially.
5) There is nothing you can do to improve skin tightness after the surgery. Your skin is fairly taut and will naturally tighten on its own.
6) Removing ribs will not cause any problems as you age.
7) Removing part of the 10th rib will not cause any imbalances or expose the organs to any risk of injury afterwards.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am curious if I would be a good candidate for a chin implant or sliding genioplasty to improve my looks, especially my side profile.
I am in my early 20s, physically fit, and not at all overweight. It may be in my head, but I also feel that my side profile seems to be slightly worse from the right side. I’m not sure if you see this or might have insight as to why?
I have been insecure with my side profile for as long as I can remember, and I think I have mostly isolated the problem down to my chin. I would really appreciate your opinion on what throws my facial harmony off.
I would also appreciate if you could give any estimates for pricing of possible procedures. I am a college student, but this issue destroys my self esteem so I am willing to finance within reason. I do not want to go with a subpar surgeon and have done a fair amount of research and am really impressed with your work.
Thank you.
A: Thank you for your inquiry and sending your pictures. I have attached an image prediction from the side view which demonstrates the type of change that would occur in about the 8 to 10mm range of chin augmentation. Both a chin implant and a siding genioplasty can achieve the identical side profile changes. The differences between them lies in the changes they make from the front view (an implant can make it wider or more square whereas a sliding genioplasty either keeps it the same width or makes it slightly more narrow, the cost between the two and how one feels about an implant or whether one prefers moving their own bone.
The reason your side profile looks different between the two sides is that you have natural chin asymmetry which can be seen in the front view. (the right side is a bit more pronounced than the left side)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have been researching a whole lot online and I can not find anything on “midface shortening” procedures. I have a very long midface (pupils to beginning of vermilion border) that is really bothering me. Is there anything that can be done to significantly shorten it or am I just forced to have to live with it? My nose is long and my philtrum area is around 15mm long. Can rhino/lip lift decrease the length of my midface by at least 10mm or is that just impossible and if so than why?
Thank you in advance😊
A:Unlike the upper and lower facial thirds, the middle of the face can not undergo any substantial length shortening. It does not matter what you do to the bone the overlying soft tissues are not going to shorten. You have mentioned the only two procedures that can be helpful to create some appearance of midface shortening. (subnasal lip lift and tip rotational rhinoplasty) Whether that wouold be effective in your case would require computer imaging to determine.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m interested in Medpor implant removal. I’ve heard many horror stories about Medpor removals, such as nerve injury. But my understanding is that Medpor implant is placed under the periosteum — shouldn’t this separate the nerve/muscle and the implant. Or is that because they are adherent, so it requires a careful dissection to avoid tearing the nerve ending?
I was wondering if this “traumatic” removal will hurt the soft tissue, which leads to any functional problem or any indentation.
Also, many surgeons state that revision surgery is much harder because of more scar tissue and its contracture. It’s definitely harder for a nose job, but how about chin surgery? Will scar removal + fat grafting helps the revision surgery?
Thanks, and I’m looking forward to your reply.
A:cOn a comparative basis to solid silicone (which is the unspoken point of reference) Medpor implant removal is considerably more difficult and has some higher risks due to its robust tissue adherence. But that being said I have removed hundreds of Medpor implants and have not seen any adverse problems such as nerve injury or significant soft tissue issues. You do have to be careful, as you have alluded to, that the chin implant wing may be close to the mental nerve. The more relevant issue, like any chin implant removal regardless of its material, what is going to happen to the expanded overly soft tissues once the underlying implant support is removed.
Dr. Barry Eppley
Indianapolis, Indiana