Your Questions
Your Questions
Q: Dr. Eppley, I am interested in making my forehead wider and more squarer to balance out the width of my new custom jaw implants that will be placed in about a months time. I have booked in for temporal implants at this stage but not forehead as I don’t think my doctor or any doctors here are quite familiar with the procedure. I wanted to know if it is ok to request to my doctor to use Medpor temporal implants? This is because I had a look at the Medpor catalogue and have found that the Medpor brand offered a significantly BIGGER size compared to the silicone ones offered my Implantech (which my doctor will use). Medpor ones go up to 20mm in augmentation. I’ve read your resource millions of times (very helpful) and want to know do temple implants sit only on top of the soft tissue or can the implant itself be placed higher if the implant overlaps onto the bone? Or is that something a custom made forehead implant would fix? If so are there any off the shelf forehead implants available on the market to widen the forehead?
I also wanted to know if I was certain that I need a forehead augmentation in future are temporal implants necessary? Or are they needed along WITH forehead augmentation. I just don’t want to waste my money on temple implants if a custom made forehead implant will fix both areas.
A: I would never use Medpor temporal implants myself. They are too big, are very difficult to modify and are very difficult to remove should that ever be desired. (and there should be a high probability that they would) No one ever needs a temporal augmentation that requires a 20mm thick implant. They are simply too big for most cases and were initially designed for patients that suffered significant temporal muscle atrophy from neurosurgical procedures not for patients that want a pure aesthetic augmentation with a normal tenporalis muscle.
If you are seeking a temporal augmentation that reaches the high temporal region to make the forehead wider as well, only a custom designed temporal-forehead implant can achieve that aesthetic change. No current implant style, Medpor or silicone, are made to create that look as a ‘catalog’ item.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I know that the two most common surgeries in cosmetic ear plastic surgery are to 1) remove cartilage from behind the ear and move the concha closer to the head and 2) reform the antihelix. In my case, the size of my concha and antihelical fold are OK. In my opinion my main problem is that the outer helical rim is short and dipped in. What I am asking is whether you have the ability and experience of building up the helical rim? In my self diagnosis, I think that we don’t have to fix the helical rim all over the ear, we can just fix something like a one centimeter area at the top of the ear. In my self diagnosis it gives me my ideal result. Thank you very much.
A: What you are suggesting by self-diagnosis for your ear helical rim reconstruction makes sense and is possible. The helix exists as an outward curl of cartilage distinctly different than that of the anti helical fold. How to build out the helix at the top of the ear comes from knowledge of performing microtia, cryptotia and other congenital ear deformities. Based on the attached pictures of your ears, this is going to require the placement of a cartilage graft which could be harvested from the backside of the concha with no change in its appearance. The only question is whether this is best done by placing the graft on top of the existing helical rim or by placing it into a cut below the helical rim as an interpositional space to push the height of the helical rim higher. In my opinion this would best be done with the latter technique to prevent graft show through the very thin overlying helical rim skin.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Is the V-Y plasty the same thing as a lip advancement? If so, is that a procedure that can raise the height of the lower lip to have less tooth show? That is an option that I am exploring.
A: A lip advancement and a V-Y advancement are two completely different operations with varying effects on the lower lip. A lower lip advancement removes a horizontal strip of skin on the outside so the vermilion can be rolled outward making the lower lip look bigger. It will not raise up the lower lip but is done to make the lip look fuller. (have more vermilion show) A V-Y advancement is a internal vertical mucosal procedure done on the inside of the lower lip. It is designed to try and lengthen the height of the lower lip and/or release any contracture or shortening of the anterior mandibular vestibule.
Raising the height of the lower lip is challenging and there is no one single procedure that can consistently do so. It usually require a combination of procedures through mucosal lengthening and vermilion augmentation to create such an effect.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, These are a few pictures of my crown and a short video of my head. The hair on the ridges is sparse but in the furrows there is some. I’m not sure if I’m losing hair in this area due to mail pattern baldness or the cutis verticis gyrata. I just want to know my options for conceiving this. Wether it be a hair transplant over it or cutting it out.
A: Thank you for sending your pictures and the video. What you should do is based on how large of an area is involved in your scalp and how progressive or stable the cutis vertices gyrate is. If the area is small and stable and is not causing any other symptoms, it be left alone. I do not think it necessarily is causing hair loss but may just be spreading the follicles out further as it expands. (although I can not say for sure whether it is) The involved scalp area should only be excised if it can all be removed and should first have tissue expansion. The scalp is not very flexible and will leave a wide scar if it is all removed at once. If the scalp area is larger and it seems to be growing, then excision would not be advised. You may consider fat injections or PRP injections in an effort to treat it although such treatment is theoretically beneficial but not yet proven.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m wanting to find out more about the different options available for forehead reshaping. Are there alternative procedures to the shaving technique? For example are there any kinds of forehead implants, fat injections that can be used to smoothen the forehead. I will also be sending pictures within the next week or two for a more accurate price range, but can you tell me the average price range for these kinds of procedures? Thank you very kindly.
A: There are numerous different options for forehead reshaping including bone cements, custom implants and even fat injections. (not my preference but an option) When it comes to brow bone reduction, bone removal and reshaping usually works much better than shaving/burring for any significant reduction. As you can see between manipulation of the brow bone and the forehead above it, there are a variety of techniques. Which one may work best for you and what trade-offs you are willing to accept in doing them are issues to yet be discussed. It is better to determine first what methods you would choose and then an accurate cost for the surgery can be given. There are no ‘average’ costs for possible combination forehead procedures that we yet don’t even know what they would be.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have been reconsidering a sliding genioplasty procedure recently due to the great deficiency my chin has. As I stated in my last email, I am on Remicade and there is a good chance I will still be on that medication when then time comes for the procedure. Does it concern you doing a sliding genioplasty procedure while I am on this medicine? I assume healing may take longer. You have also mentioned that a sliding genioplasty with a chin implant overlay may be necessary. Will this have any negative effect on healing or increase the risk of infection?
A: I have operated on numerous patients who have been on Remicade for Crohn’s disease and I have not seen any healing problems. Such surgeries have been much bigger in surface area trauma and operative times than a sliding genioplasty. The face is uniquely well vascularized and unless there is direct impairment of the blood supply through prior radiation it will not inhibit healing difficulties. The orthopedic literature supports that major bone surgery and joint replacements can heal uneventfully with patients on this medication.
That being said, it is important to work around the dosing of the medication to reduce any risk of adverse healing. Given that Remicade is a TNF blocker and is done by infusion, it would be important to do the surgery about 3 to 4 weeks after the last infusion. This is will than allow a few weeks before the next infusion. With such an approach for a sliding genioplasty I do not envision any difficulty with healing or a prolonged recovery time.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 40 year old male who had my buccal fat pads removed about 10 years ago. My issue went unresolved however as the puffiness was closer to my mouth. There was no information online at the time and I have just lived with it. Recently, I came across the term ‘periorial mounds’. I went to see a local plastic surgeon about it and he admitted that he had never heard of such a procedure, that it would be much too risky and that there is no fat there regardless. I came across your name when further researching it. You seem to be alone in addressing the needs of people with this issue. I have attached photos of my condition and would love to get your feedback. I should mention, it is not only the visual aspect I am hoping to change, but also the constant weight I feel around my mouth. My questions are:
1. do I qualify for perioral mound reduction?
2. do I risk damaging nerves?
3. will the amount you are able to reduce have a noticeable effect physically?
4. will a reduction aid in reducing the fat on my jawline?
Thank you so much in advance for any further knowledge you can bring me, I really appreciate it.
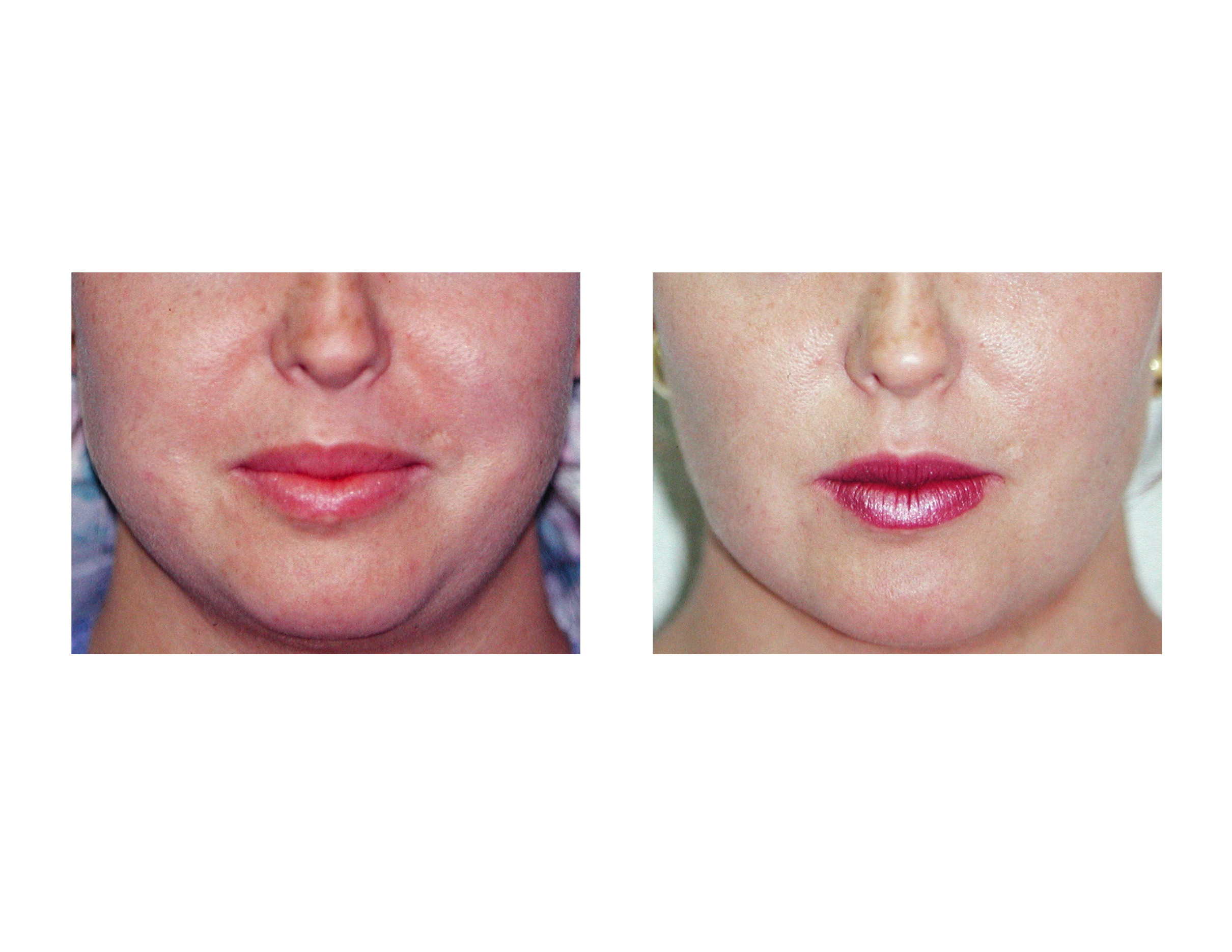 A: The perioral mounds are a well known collection of subcutaneous fat that exists at the level of the corner of the mouth that is distinctly different than that of the buccal fat pads. It can be reduced by very small cannula liposuction and even a 1cc to 2cc fat reduction can make a noticeable difference. Although some plastic surgeons make not be familiar with its treatment, that does not mean it does not exist nor is it risky to do. In answer to your questions:
A: The perioral mounds are a well known collection of subcutaneous fat that exists at the level of the corner of the mouth that is distinctly different than that of the buccal fat pads. It can be reduced by very small cannula liposuction and even a 1cc to 2cc fat reduction can make a noticeable difference. Although some plastic surgeons make not be familiar with its treatment, that does not mean it does not exist nor is it risky to do. In answer to your questions:
- You do have a fullness in the perioral mound area with an overlying skin fold which presumably is due to aging. (descent of the midfacial tissues) It is impossible to know beforehand how much the skin excess or subcutaneous fat is contributing to that appearance. But in my experience removing the subcutaneous fat through perioral mound liposuction can make that skin fold ‘lay down’ so to speak.
- This is a very safe facial area to do liposuction in. The buccal facial nerves run above it and the marginal mandibular nerve lies below it. This is a safe facial triangle for subcutaneous fat removal.
- There is no way to absolutely predict the change but I have yet to see a patient who did not get some improvement in their perioral fullness.
- The liposuction can and should be carried down to the jawline to maximize the procedure’s effectiveness.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have low set tilted back ears. I want to know if it is possible to bring the ears forward, thus raising the top vertically? In other words, is it possible to rotate the right ear clockwise, the left ear counterclockwise; thus, rotating the top of the ear forward. I obviously do not know anything about this, but it would seem that the rotation would result in the top of the ear being ‘higher up’ five millimeters or more depending on what is possible. I understand the canal cannot move upwards. If this is possible, how much vertical increase in the top of the ear would result from the forward rotation? Is it possible to rotate them forward so that the top of the ear is the eyebrow level without relapse?
I also desire the lobes to be shortened and the ears pinned so they do not stick out so much. Attached at the bottom are pictures. Lastly, if this is possible, is this an otoplasty procedure that you perform? Thank you for your time and consideration.
 A: I have done numerous ear lifting type otoplasty procedures, some with moderate success and some with little vertical change at all. You are correct in your assessment that the fixed point of the cartilaginous ear is the canal which prevents any significant cartilage relocation. Whether the upper half of the ear can be moved upward at all this depends on the flexibility of the superior helix. Any lifting effect at all comes from relocating the area behind the anterior crus of the helix upward. By suturing this cartilage area up higher on the temporal bone with microscrew fixation, some vertical lengthening of the upper ear can be achieved. That effect can be maximized with setback of the upper helix since this also can cause a rotation effect if desired and appropriately sutured. Putting the two together can help raise the vertical height of the ear but not to the level of the eyebrow however. A vertical reduction of the earlobe will also help not only shortening the vertical length of the ear but may also help create the illusion that is actually higher.
A: I have done numerous ear lifting type otoplasty procedures, some with moderate success and some with little vertical change at all. You are correct in your assessment that the fixed point of the cartilaginous ear is the canal which prevents any significant cartilage relocation. Whether the upper half of the ear can be moved upward at all this depends on the flexibility of the superior helix. Any lifting effect at all comes from relocating the area behind the anterior crus of the helix upward. By suturing this cartilage area up higher on the temporal bone with microscrew fixation, some vertical lengthening of the upper ear can be achieved. That effect can be maximized with setback of the upper helix since this also can cause a rotation effect if desired and appropriately sutured. Putting the two together can help raise the vertical height of the ear but not to the level of the eyebrow however. A vertical reduction of the earlobe will also help not only shortening the vertical length of the ear but may also help create the illusion that is actually higher.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am asking an identical array of questions of different surgeons both to become more knowledgeable on the topic as well as making a decision on choosing a surgeon. If you were to undergo sliding genioplasty, which five top surgeons would you choose based on experience and reputation.
A: This is an excellent question and I wish I had a similarly good answer for you. There are many surgeons of different specialities that perform sliding genioplasty but who would be ‘top five’ would escape me. Since I have never seen another surgeon actually perform this procedure other than myself (and that was decades ago in my training), all that I have to go on is whom writes clinically and scientifically about the procedure. And because it is an historic maxillofacial procedure of which there is little new, few surgeons today publish on this procedure. Thus creditable knowledge of who performs a sliding genioplasty technically well I do not know. That does not mean they do not exist, as obviously they do, but I could not honestly give you a list based on useful knowledge of them.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was interested in getting a consult for myself for the Vanquish vs. Exilis for several areas. I was also going to potentially buy a gift for my significant other as he is very concerned about abdominal fat. He also is considering Liposuction, so I looked that up. In your article about Liposuction you indicated that non-surgical, non-invasive fat removal methods are often not realistic and over hyped. Now, I am not sure whether to pursue the consult for the Exilis and/or Vanquish.
 A: Any non-invasive body contouring procedures can not be compared in results as to what surgery can do. (e.g., liposuction) They rarely are even close. In general, there is a often a disconnect between patient expectations and what these types of treatments can do. Between a patient’s hopefulness and device marketing (by both manufacturer and practitioner), there is ample opportunity for patients to be disappointed. This does not mean that these devices are not beneficial and can not create moderate body contouring results, but each patient needs to be assessed individually to determine how non-surgical vs. surgical ROI (return on investment) compares. That requires a thoughtful and honest discussion which I regularly do for many potential patients seeking such treatments. I own both Vanquish and Exilis, so I have great insight into their potential value, but I also have no interest in patients making a ‘poor investment’ either if they are not good candidates for them. I would recommend that you and your husband come in and talk to me about it.
A: Any non-invasive body contouring procedures can not be compared in results as to what surgery can do. (e.g., liposuction) They rarely are even close. In general, there is a often a disconnect between patient expectations and what these types of treatments can do. Between a patient’s hopefulness and device marketing (by both manufacturer and practitioner), there is ample opportunity for patients to be disappointed. This does not mean that these devices are not beneficial and can not create moderate body contouring results, but each patient needs to be assessed individually to determine how non-surgical vs. surgical ROI (return on investment) compares. That requires a thoughtful and honest discussion which I regularly do for many potential patients seeking such treatments. I own both Vanquish and Exilis, so I have great insight into their potential value, but I also have no interest in patients making a ‘poor investment’ either if they are not good candidates for them. I would recommend that you and your husband come in and talk to me about it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have breast implants and I want them removed. I do not want another implant and instead want fat transferred to my breasts.
A: . Fat grafting to the breast can be done when implants are removed. But the advisability and success of the procedure is predicated on several important issues. First, do you have enough fat to harvest to make the procedure worthwhile? Since only concentrated fat is injected, it takes a greater fat harvest than most patients think to have enough injectate to produce any significant breast volume. Secondly, it is important to know how much actual breast tissue you have between the breast skin and implant capsule as this is the layer that is injected. Fat can not be injected directly into an empty implant capsule. There must be enough tissue between the skin and the capsule to serve as a recipient site. Lastly, what are your size expectations and can fat serve as an adequate substitute in volume for your existing implants. Unlike implants which have stable volume, injected fat has a variable take which will always be less than what was initially injected. Therefore patient expectations should be tempered with what fat can actually achieve in terms of final volume retained.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I exchanged my saline implants for silicone about 3 years ago and my new scars never healed as nicely as my original (invisible) scars. Immediately after replacement surgery I could tell these were wider, longer and more irritated looking than my originals (particularly my left). I have had a few different Fraxel and V-beam treatments to see if that would make me happier but I wasn’t too impressed. While these are not horrific scars, I am definitely self conscious of them compared to my originals..Do you think it would be possible to improve these scars with a revision, ultimately aiming for thin, non-pigmented scars like my originals? Thanks!
A: Breast implant scar revision usually produces a better result than any type of more superficial treatments like laser or light treatments. The only improvement that can come for your breast implant scars would be through this type of scar revision. This means actually cutting out the existing inframammary scars and re-creating new scar lines. I believe this will provide an improvement in their appearance but whether they will every return to what the scars initially looked like can not be guaranteed. It is difficult to ever go back to the scar result that occurred from cutting into new unscarred skin.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Wondering if you do maxillomandibular advancements surgery for sleep apnea or know of any other plastic surgeons that are also dentists/oral surgeons that might do this procedure. Would prefer to have a oral surgeon that is also skilled as a plastic surgeon in hopes of having not only a successful surgery, but also a better cosmetic outcome. Thank you.
A: I do perform bimaxillary (maxillomandibular) advancements for obstructive sleep apnea. You are correct in that there can be a delicate balance between how much to move the face below the eyes forward and not so much that it creates facial disharmony. (resultant infraorbital-malar hypoplasia) As a general rule it is recommended to move the maxilla and mandible as far forward as possible. (usually about 10mms) But in some patients that may well create a ‘protruding lower face’ that is disproportionate to the natural facial appearance above it. This requires insightful planning beforehand based on the patient’s facial shape. Using computer imaging and VSP (virtual surgery planning) for the facial bones from the patient’s 3D CT scan, more thoughtful surgical planning can be done that takes into account both the functional and aesthetic needs of the patient.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was inquiring to see if masseter muscle reduction surgery is something you can do? So rather than a jaw reduction of the bone, just reduce the muscle in the jaw. I’d be coming in from Arizona for surgery so approximately how much would something like that cost me? And what would the recovery time be? Thank you.
A: Masseter reduction surgery can be done but it does slightly different than one would think. You do not go in and cut a portion of the muscle out as that would be very bloody and would likely leave the outer facial contour irregular when it heals. Rather the muscle is lift off the bone from the inside of the mouth and its inner surface treated by electrocautery. This will cause some muscle fibers to die and a portion of the muscle to atrophy obver time. Also Botox is injected into the muscle at the same time to help the atrophy process. I assume you are aware that you can treat masseter muscle hypertrophy with repeated Botox injections to help it shrink without surgery.
Other than some swelling there really is not much recovery or limitations after surgery. The jaw will feel stiff for a few weeks from the muscle treatment.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a mild chin cleft that I would like corrected. I have attached a picture so you can have a better understanding. It drives me nuts when I smile as it is so visible particularly in pictures.
A: By your picture what you have is a chin dimple not a chin cleft. That may seem like a semantic difference but anatomically there are somewhat different entities and are treated a little differently. A chin dimple that presents itself when you animate (smile) represents a defect in the mentalis muscle that covers the chin. Lacking fat underneath it and a defect in the muscle, the skin is pulled inward acting like an adhesion to the underlying tissues. Conceptually, volume needs to be added under to dimple to push it outward. This can be done by a number of ways but the simplest method is to place some injectable fillers (e.g., Juvederm) underneath the chin dimple. While this simple office treatment will not be permanent it will last 6 to 9 months and will answer the question whether the ultimate placement of fat injections would be the best long-term treatment of your chin dimple correction.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am very interested in your custom one-piece wrap-around jawline implant but have a few questions.
1. I saw an example of your custom wrap-around implant in an article you published on August 24, 2014 on your website. It was very impressive and exactly what I’m looking for. How difficult is that procedure compared to the standard 3-piece chin/mandible implant?
2. Is the recovery time and swelling reduced in the one-piece wrap-around implant compared to the 3-piece (because it is inserted only under the chin and not inside the mouth as in the 3-piece)?
3. Is the incision under the chin larger in a wrap-around implant compared to just a standard chin implant incision?
4. Apart from cost, what disadvantages do custom wrap-around implants have against an off the shelf 3-piece? (In other words, if cost wasn’t a factor, why would I or anyone ever consider a 3-piece implant?
 A: In answer to your questions about a custom wrap around jawline implant:
A: In answer to your questions about a custom wrap around jawline implant:
- If your questions about difficult relates to its surgical placement, it is not more difficult than placing standard chin and jaw angle implants…if one had done it a fair number of times.
- Usually three incisions are still used for a custom wrap around jawline implant because it is critically important to check and ensure that the posterior jaw angle portions are properly positioned on the bone. But the overall swelling and recovery are no different than placing three separate chin and jaw angle implants.
- The incision under the chin is the same for either standard chin implants or a custom jawline implant.
- Good question! They are so superior that cost would be the only reason not to use them…and when the costs are considered for either a standard or custom jawline implant approach the custom implant is not significantly more costly.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 32 year old male. I have a very flat brow bone and have been looking at getting something done as I believe it detracts from my overall appearance. My biggest concern has always been about the severity of the surgery to do something about it. It seems to me that you have multiple solutions which offer a more minimally invasive procedure. My question is about the cost of Endoscopic Placement of Custom Brow Bone Implants and the lifetime of those implants. Do they need to be replaced? And what are the complications with the procedure. If you could please let me know that would be greatly appreciated. Thank you.
A: Custom brow bone implants, like all custom facial implants, are made of a solid silicone elastomer material. They are permanent implants, will never degrade or breakdown and will never have to be replaced. They are placed through an endoscopic technique using two small incision either in the scalp or at the edge of the hairline. While there are potential complications with any facial implant procedure (e.g., infection, malposition), I have yet to see any with that of the brow bone. The one huge advantage to a custom approach is that the implants will have a precision fit and the their size and shape will have been designed in advance to the aesthetic desires of the patient.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a consult scheduled with you in the next few weeks for a breast lift and removal/replacement implants. I was also wondering if you could answer some questions about the differences between Exilis, Vanquish, Venus Freeze, Cool Sculpting and I-lipo. A friend of mine has tried the I-lipo. I have read about all of them online. Hard to tell what the “best” option for a little targeted fat loss and skin tightening would be. Maybe they are all good options.
A: In today’s world of non-invasive/non-surgical body contouring, there are a number of devices that are currently available for some degree of fat loss and a little bit of skin tightening. (and I want to emphasize the phrase ‘a little’) All available devices are based on some form of penetrating energy from ultrasound, infrared, radiofrequency and thermal sources. They all claim effectiveness but whether one is better than the other can never be proven since there are no comparative clinical studies of them. I have used most of these devices and, in the properly selected patient, can offer some reasonable results. Currently we use Vanquish and Exilis for the best non-invadive body contouring results, They are best used in those patients who are never going to have surgery to those that want to give it a try with actual surgery as a final treatment if needed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am unhappy with my nose and I have been considering rhinoplasty for a while as well as jaw augmentation. For my nose, my first main concern is that I don’t like the bulbous tip it has. I’d like the tip to look pointier and to project a bit more. Second, I think my nose is too wide. I would like my nostrils to be narrower from the front view. I have attached a few photos of my face, as well as a couple models whose noses I like.
For the jaw, I have been considering some combination of chin and especially jaw angle implants. Perhaps even sliding genioplasty, the latter I understand is the only way to add vertical chin height. I basically want to create a stronger looking profile that balances my face.
I also have a few secondary procedures I am considering but not sure about. A reduction of my lower lip reduction (I think it is too big compared to the upper, and might make my chin appear larger if it were reduced). And also forehead augmentation (to reduce the appearance of my sloping forehead/prominent brow bone)
I am trying to figure out which procedure/s would produce be the best result in my case.Would it even be possible to do all of them at once?
A: Briefly, all the facial procedures you have discussed can be done as the same time and it would not be rare in my experience to do so. But first we must go through each procedure and determine what is the best approach for each change and how much change you desire for each area. Options in rhinoplasty and jawline enhancement are best done through initial computer imaging. I will do some computer imaging using your pictures of these changes and this will be a good starting point for our treatment planning discussion.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, the right side of my face looks bigger and more elevated than the other side, and the position of my right eye socket is higher than that of my left one. My jaw is also asymmetrical. When I bite, I can feel that the left side of my upper jaw and lower jaw is higher than the right side. I can also feel that the bone between my right eye socket and.my upper jaw is bigger than that on the left side when I touch. Is it possible to make my right side identical to the other side? If so, could you advise me on what procedures I should take and their costs? Thank you.
A: For your facial asymmetry correction, there are some structures that can and can not be changed. It is not possible to lower a higher eye socket. (orbital box) A lower eye can be raised somewhat but a higher eye can be lowered. Your maxillomandibular cant (jaw asymmetry) can be corrected by a LeFort I osteotomy to shorten the longer side. (vertical maxillary reduction) To keep your current occlusion (bite) a sagittal split ramus osteotomy is needed to rotate the lower jaw back into occlusion as well as complete the vertical shortening of the right lower face.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in getting a chin implant but had radiation for a sarcoma on my chin as a teenager which was over thirty years ago. I have read that you like to inject fat prior to placing an implant in an area that has previously received radiation. But doesn’t the fat just go away?
A: The purpose of the fat injections is not to create the augmentation effect, although it may have some mild benefit in that regard. Their purpose is to improve the blood supply and healing potential of your chin to eventually withstand the effects of placement of a chin implant. Fat injections are well known to help reverse the effects of irradiated damaged tissues through a process known as neovascularization. The fat may indeed partially or completely resorb but it will have improved the blood supply of the tissues through various stem cell and growth factor effects. With your history of facial radiation treatments with the chin as the direct recipient of them, placing a chin implant into these damaged tissues could be fraught with wound healing and infectious problems afterward. At the least, fat injections will help soften the chin tissues in preparation for the stretch effects of what an underlying chin implant will create.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m currently in the midst of orthodontic treatment and I’m scheduled for some surgical palatal expansion and double jaw surgery later on (Lefort I). I have recessed maxilla and mandible bones, so they will both be advanced (after my palatal expansion is complete).
I also have a midface deficiency. I have a tear trough deformity and scleral show. I believe that a LeFort III would work for me, but I have to be realistic because it’s very invasive. I don’t suppose I’ll be able to find a surgeon to perform such an invasive operation on me – which is why I would like to ask if a malar osteotomy and some kind of orbital rim procedure after my jaw surgery would produce the same results as a Lefort III – filling out my midface, making my cheekbones more prominent, and correcting scleral show. Do you offer those procedures?
A: There is no question that a simpler and more effective treatment to your upper midface concerns is NOT a LeFort III but custom orbito-malar facial implants. They would provide a much better result than trying to move the bone and are made from a 3D CT scan and could be done after your orthognathic surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am inquiring about abdominal implants to create a 6 or 8 pack look to the abdomen. I think they called are ‘blocks’ and up to 8 implants would be needed. Can you tell me anything about this procedure?
A: In the fast track way to six-pack abs, abdominal implants are different than abdominal etching by linear liposuction. While linear liposuction looks to make the six-pack look by accentuating the muscular inscriptions through fat reduction under the skin along their lines, implants do exactly the opposite. They are placed between the inscriptions under the fascia like a muscle implant to accentuate the bulging between the inscriptions. Thus they are like ‘blocks’ so to speak. Other body implants, like buttock or pectoral implants, are carved down to make the soft supple implant shapes that go between the inscriptions under the abdominal fascia. There are not true abdominal implants, just other body implants that are modified. But shaping the implants is not real the hardest part, it is the placement of them that is the challenge. If one was having an open tummy tuck, then their placement would be easy and this is why it is frequently recommended to do them at that time. But the vast majority of patients that want six-pack abs don’t need a tummy tuck. Thus they must be placed through a belly button incision and with this limited access it can be a 2 to 3 hour surgery to do so.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a chin implant revision. I wrote to you awhile back about getting a button style chin implant after a chin reduction by sliding genioplasty. My chin was reduced about 4mm. I then got a 3mm button chin implant placed, hoping to reverse the outcome of the chin reduction. Thankfully I’ve had no complications but I know have the look of slight jowls of both sides of the implant, especially on the left side. I’ve tried fillers but I really can’t afford to get fillers placed every year. Have you ever placed an extended anatomical implant with wings that measure 1mm in thickness? Have you ever placed an extended anatomical that has one wing thicker than the other to fix asymmetry? Thanks for your time.
A: Most chin implant wings, if they are made of silicone, are very thin often being only 1 to 2mms in thickness as they taper back along the jawline. The chin implant wings can be adjusted in length and thickness to compensate for asymmetry between the two sides. That is not an uncommon modification done in some chin augmentation patients whether it is a primary surgery or a chin implant revision.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I recently posted a question on Real Self regarding my cupid’s bow and if/how it could be changed in shape. (upper lip reshaping) I got a response from you and was wondering if you could possibly explain it further. You said you can change the distance between the height of the cupid’s bow slightly through small skin excisions on each side of the existing cupid’s bow. Forgive my ignorance here but does this mean that the height between the cupid’s bow can be lowered? I was also wondering if a dermal filler on the outer portion of the upper lip would even out my lips and make the cupid’s bow less prominent. Thanks in advance for your response.
A: My remembrance of your question was that the height or peaks of the cupid’s bow was too vertically high. By removing the peak of the cupid’s bow through small vermilion excisions, their height could be reduced by a few millimeters. That would smooth out the cupid’s bow to some degree. The trade-off is that there would be a very tiny scar between the vermilion and the skin. You could also go in the opposite direction and lift up the sides of the vermilion outside of the cupid’s bow to reduce their appearance. (lateral vermilion advancements) Injectable fillers may help in that regard but do not have the same vermilion lifting capabilities and would have to be repeated. But it is certainly a non-surgical lip reshaping test of that approach and there is no harm in doing so.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, It was good to meet you today to discuss my wife’s breast augmentation incisions options. We had a follow-up question for Dr. Eppley regarding one aspect of the proposed augmentation that we were hoping he could comment on.
We visited with another plastic surgeon later today,who suggested that because of her ever-so-slightly nipples facing outward and to the sides and not completely to the front, he would most likely insert the implants somewhat to the outside edge of her breasts so as to promote a more inward-facing profile of her breasts post-surgery. In effect, the surgeon expressed an interest in being able to have the greatest amount of control possible in the placement of the implant during surgery. To achieve this greater control, however, the surgeon advocated for inserting the implants through the areola instead of through the armpit.
While she definitely likes the idea of a transaxillary implant so as to avoid the presence of scars on her breasts, we would like to understand whether in fact it’s true that this approach might not give as much control around the implant placement, especially given her particular physical circumstances. Could you give us some perspective on this issue and whether indeed there’s a tradeoff here between the two insertion approaches that we should more carefully consider?
A: It is important to understand that the location of the incision in breast augmentation is largely about access to the submuscular and subfascial breast planes..once you are in there what is done is the same…the development of the implant pocket. Considerable experience and skill allows a plastic surgeon to use any of the incisions will equal ability to make whatever pocket one wants. Plastic surgeons frequently use only one incisional approach because that is what they are most comfortable doing so it eventually becomes the ‘best’ way to do the operation…and if that is what their comfort zone is then it is in fact the best way for them to do it. But the areolar incisional approach offers no advantages in terms of visibility or pocket creation than either the transaxillary or inframammary approach breast augmentation incisions.
One of the keys to breast implant placement is to get it centered on the existing breast mound. Trying to place it more to the side so the nipple might be ‘pushed inward’ is not going to create that effect and tuns the risk of having an implant becoming lateralized or ending up too far to the side of the chest wall. This is one implant location to avoid as it is a difficult problem to fix later. It is far better to accept some minor nipple location flaws than to create what may turn out to be a bigger aesthetic problem later.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in the customized one-piece jawline enhancement. I live in Sweden and have been talking to a doctor in NY who is using implants made of Medpor instead of silicone for the mandibular angles. Medpor is a material that your body grows into therefore the risk of misplacement or jawline breakdown is reduced.
1. Is it possible to have the custom implants to be made in Medpor instead?
2. Could you send me at least 10 before and after pictures of patients who have had jawline enhancement with the custom implants?
3. I know the custom implants varies in price but could you give an approximate price so that I know how much money that I need to save?
4. Can I pay 1000 dollars/month?
5. How soon can I have the surgery done? I would prefer to have it done this month or the next since I have my vacation now.
6. How long do I need to stay if I want the custom implants? I read from the Q&A that it takes 3 weeks to get the custom implants from the 3D-scan. After surgery I need to stay probably another 2 weeks right?
7). As I fly in from Sweden, where can I live during my stay and how much will it cost for 5-6 weeks?
A: In answer to your questions about a custom one-piece wrap around jawline implant:
- A custom one-piece jaw implant can only be made of silicone not Medpor. Even if it could be made of Medpor, it could never be placed as a single piece. That material is too stiff and would need to be sectioned into three pieces to place it…but even that would not be easy. The ingrowth of tissues into Medpor often poses more problems than it ever solves, particularly if you have to revise, replace or try to remove them. A custom implant does not shift because of its precision fit.
- Due to patient confidentiality, we do not distribute patient photos randomly across the internet.
- I will have my assistant Camille pass along the cost of custom jawline implants to you tomorrow.
- Surgery fess must be all paid in advance not in partial payments after the procedure.
- It would take a minimum of three weeks just to have a custom implant fabricated. Thus unless one wants to use a three-piece implant approach with standard implants it can not be done this month.
- The 3D CT scan is done in your country and send here to make the implants. You come here one day before the surgery and return home 48 to 72 hours after the procedure.
- You only need to be here a few days to have the actual procedure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I asked you about my skull shape problem before but I don’t think I’ve describe it accurately.The problem with my “big head” has been troubling for years and I hope to resolve it once and for all.
Here is my problem:
My head looks normal when viewed from the front or back. But when viewed sideways, it looks big. Specifically, the distance between the forehead to the back (the occipital region) is too large.
If one would to look at the top of my head from a bird’s eye view, the back region is sort of a “trapezoidal” shape, in that the middle portion protrudes too much out. I wonder if it’s possible to “push back” on the middle portion and fill up the side, so that the head will be a more flat or rounded shape rather than trapezoidal.
I think the only way this can be done is via a partial removel of the skull, and putting it back like a jigsaw, or maybe even replacing that portion with an artificial skull. I wonder if this is within your specialty. I heard the risk of death or disablement from this might be as high as 50% so I might not do it if that’s the case.
My goal is to reduce the said distance between the forehead to the back by 20mm. On your website, most of the skull reduction procedure I’ve read about deals with mechanically removing a portion of the skull and making it thinner. I’m not sure if that would be enough in my case. I’ve read that the human skull thicknes is only about 10cm thick at most.
A: Realistically what you are asking can not be done. The outer portion of the skull can be shaved down by removing the outer cortex. When done in the forehead and occiput, the anteroposterior (front to back) distance can be reduced probably 10 to 12mms at best. You can not remove skull pieces and put them back together any way you want because of the space occupied by the brain. This space can not be reduced or intruded upon, only the outer portions of the skull can be reduced which protects and maintains the intracranial space for the brain.
Dr. Barry Eppley
Indianapolis, Indiana
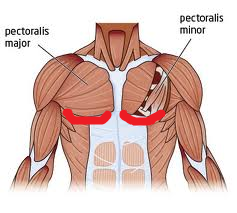 Q: Dr. Eppley, I am wanting to know how much the costs would be for fractional laser resurfacing underneath the bottom outline of my pectoral muscles would be. There are some small, fine wrinkles that I am wanting to treat. I highlighted in red the approximate area in the photo.
Q: Dr. Eppley, I am wanting to know how much the costs would be for fractional laser resurfacing underneath the bottom outline of my pectoral muscles would be. There are some small, fine wrinkles that I am wanting to treat. I highlighted in red the approximate area in the photo.
A: Fractional laser resurfacing is most commonly done on the face which responds very favorably due to its excellent blood supply and quick re-epithelization properties of the skin. As you move below the jawline, and particularly below the neck, greater caution must be exercised as the skin healing properties as not as great as that on the face. This does not mean that laser resurfacing on the chest can not be done…just that it must be done less deep and in stages to avoid creating scarring and hypopigmentation.
I would recommend that you first have a test patch of a certain laser resurfacing depth done to make sure this body area can heal without any adverse effects.
As general cost information, I will have my nurse send to you tomorrow a fractional laser resurfacing series cost.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have some questions about implants for skull reshaping. These are the questions that I would like for you to answer. Thank you for taking the time to answer them.
1) My main concern is to eliminate the cone shape at the top of my head. It appears that using implants would give me better results than just burring the scalp. Which one of the two do you believe would give me the best possible aesthetic look? Meaning the most proportional/normal looking head? If I can achieve a normal shaped head, “with implants only” I do not see the need for you to burr the scalp. However, if you believe that implants “alone” cannot give me the best possible shaped head, I would go with the option where you burr and insert implants. I don’t think I would have a problem with the height of my sagittal crest if the sides of my head would not be so slanted.
2) If you only use implants and do not burr the skull down, would this create too much tension on the top of my head? Will the skin on my head once pulled over the implants create too much tension that would then lead to pain in my head?
3) Am I going to be limited in the kinds activities I could take part in? For example, would an activity like diving head first into water be considered unacceptable for fear that the implant will move out of place?
4) Does this procedure require maintenance? Will I have to replace the implants after time goes by? Or can I can I live out my life without having to worry about it again?
5) What kind of material are the implants made from?
6) How long until the scar is completely healed, or the time frame when I will know the scar will look as good as it’s going to look?
A: 1) That is why I do computer imaging to look at all options available for skull reshaping. By looking at the head shape outcomes from all three methods, YOU can make that determination. This is a purely aesthetic judgment of what you think looks the best.
2) No, The skull implants are not that big.
3) No, you would have no physical restrictions and they will not become displaced no matter what you do.
4) The skull implants are permanent and will never need to be replaced.
5) They will be custom implants made of solid silicone elastomer and will feel just like bone.
6) Scars take put up to six months to fully mature. Although many scalp scars do well and mature before that time period.
Dr. Barry Eppley
Indianapolis, Indiana