Your Questions
Your Questions
Q: Dr. Eppley, Good morning. I have a question about trichophytic incisions. After a procedure, roughly how long does it take hair to grow back through a trichophytic incision back to it’s regular density?
I had surgery with a coronal incision 3 months ago, and although the hair is growing through it still is not back to its regular density. Will it probably take a little longer?
A: Time will tell but I would not expect it to grow back through the scar in the same density that existed in the scalp area before even if a trichophytic incision was used.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, The top back of my skull is depressed due to surgery as an infant. The depression is deep, wide and long so if plastic surgery was performed it would need to stretch skin or need a skin graft. I’m not sure of your capabilities but has your practice dealt with the issue described. Thanks.
A:What you are suggesting is the possibility of needing a first stage scalp expander procedure. (not a skin graft) That is a procedure I do regularly when more stretch of the scalp is needed for the amount of skull augmentation required.
Dr. Barry Eppley
Indianapolis, Indiana
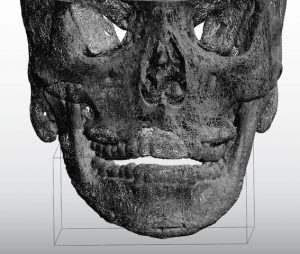
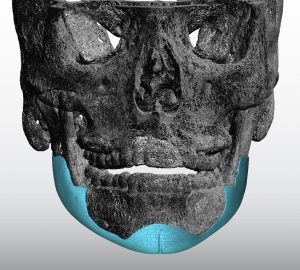
Q: Dr Eppley, Thank you so much for replying to my question about v line reversal implant surgery! May I ask how high the infection rate is for a custom silicone implant as that is a problem I am scared of having. Also since I had a sliding genioplasty. to make the new custom jawline implant that wraps around my whole lower jaw would I need to reverse the sliding genioplasty to put the implant in or would it be okay to leave at where it is at since my chin still does not have enough projection and it was moved foward 10mm. Thank you!
 A: In an
A: In an
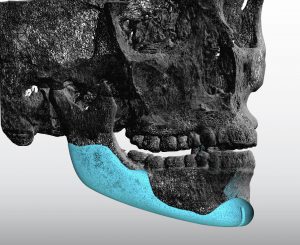 swer to your v line reversal surgery questions:
swer to your v line reversal surgery questions:
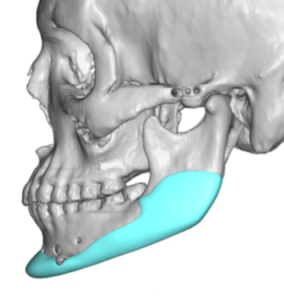
1) the infection rate in custom jawline implants is in the 3 to 4% range.
2) the sliding genioplasty stays in place and you build around it.
3) the attached images may be helpful in understanding how the implant works in v line surgery reversal.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had jaw reduction surgery along with a sliding genioplasty however, the surgeon over reduced my lower jaw and I developed step-off deformity from sliding genioplasty. The lower half of my face is over reduced and smaller than the upper part making my face look off-balanced. I would like to rebuild my entire lower jaw. Would I need jaw and chin implants or would I have to get a custom jawline implant? Would bone cement be okay for an implant or is silicone better? Would bone grafting work? What are the pros and cons of bone cement/silicon implants and bone grafting?
A: Over reduction from vline surgery is actually very common and is just the nature of how that surgery has to be done. When it comes to rebuilding the inferior border of the lower jaw (which is what is now missing and is what is the cause of the notch deformity from the sliding genioplasty) this can only be done with a custom implant approach. Bone cements, standard implants and bone grafts are not going to work and will just make matters worse. Besides the fact none of these can stick and create a new extended jawline border out into ‘space’ they will be associated with a very irregular/asymmetric jawline result…which will be worse aesthetic problem than what you have now.
 One can have debate about the use of silicone or Medpor custom jawline implants (PEEK is not commercially available in the US for jawline implants) but economics will end that debate for a custom silicone jawline implant in most cases.
One can have debate about the use of silicone or Medpor custom jawline implants (PEEK is not commercially available in the US for jawline implants) but economics will end that debate for a custom silicone jawline implant in most cases.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have mandible implants sized 11mm and chin implant sized 9mm ( all silicone) I am now3 months post op and am planning on getting them all removed. Will my face go back to the way it was? If not how close will it be? I’m 23 years old and I have thick skin according to my last surgeon.
A: The key question is if you knew your face would not go completely back to the way it was….would you still take out the chin and jaw angle implants?
The point being is that no one can predict precisely what will happen when they are removed. There are always going to be some aesthetic tradeoffs from removing them because of the stretched/expanded tissues. The only question is whether those aesthetic tradeoffs are better than living with the way you look now.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have done a CT of my face and my Dr left me know that my right side of face is around 5 millimeters more retruded so the other side is 5 mm more forward. I know there are implants for that purpose but I want to try with own materials
So do you think it is possible to move forward the midface more than 5 mm including: FRONT OF ZYGOMA, MALAR AND CHEEK BONE up to around the nose and infraorbital area. This is my concern how much can be forward midface on one side but no jaws not necessary pnly face: front of face : zygoma, infraorbital malar…( Augmentation)
How would you perform that please. Through osteotomy forwarding or in combine with bone grafts but remember please it is necessary for 5 or 6 milimeters augmentation for that i need to know how can be done this without implants.
And please dear sir what you think is it possible to gain a very good symmetry with both sides through osteotomy and using bone grafts.
You are very experienced surgeon and you may know how much symmetry can be achieved
Many thanks
A: The dimensions of the bony augmentations of the midface you seek are anterior and can not be done by any type of osteotomy. (bone movement) Your only autologous option is onlay bone grafts which will not provide a smooth contour and will likely undergo some resorption…and perhaps even complete resorption over time.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a young male in my 20s. My right shoulder is shorter than the left since I was born. It is genetic. My father has the same condition. No problems except cosmetic reason. My right clavicle is more curved than left.
I want my both shoulders equal and identical. Is it possible Sir?
A: Thank you for your inquiry and sending your pictures. It appears your right clavicle is shorter than the left one, perhaps by about 2.5 to 3 cms. Conceptually the right clavicle can be lengthened by the placement of an interpositional fibular bone graft of that length. The key question is where on the shaft of the clavicle should that be done. It appears that the inner third of the shaft would be the best location for the osteotomy and graft. Although a 3D CT scan of your shoulders would show the clavicle anatomy in detail and would be very helpful in making the decision for the best osteotomy location.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi, as you can see on the images in the file I look a LOT better on the right. They were both taken today, the only difference is that I bite together on the left picture which in my opinion looks horrible. On the right I jut the jaw forward and downward. (I think my whole lower jaw is too short as well)
I’m going to have double jaw CCW surgery in a while for health reasons, but when it comes to aesthetics I’m not sure it’ll do the trick.
As you may understand, my dream look is on the right, how do I achieve that in combination with double jaw in the best way? Hope you understand what I mean.
A: Thank you for your inquiry and sending your pictures. While such a facial change as you have illustrated is possible it can not be done at the same time as orthognathic surgery. You need first to get the skeletal foundation functionally corrected and then you can build off that to augment the remaining missing contours. Orthognathic surgery will provide some sagittal forward jaw movement but not any width or angular contours This is going to require a custom jawline implant AFTER your orthographic surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have very noticeable bumps behind both ears. I had a scan a few years ago and it is due to unusually large mastoid air cells. Can something be done about this? I’m 38 and get made fun of wherever I go.
A: Enlarged mastoid processes can be reduced. The key is knowing that these are air cells so in their reduction the mucosal lining needs to be removed and covered in hydroxyapatite cement to prevent postoperative infection.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, What I’m confused about is I also consulted with another surgeon. He suggested a 9 mm silicone off the shelf without wings. He’s not reshaping it, implant as is so yes the implant is round. I held it. While your imaging suggests a 4 to 6 mm size, at least the ones that are appealling me. So are you under projecting or is the other surgeon’s size is big?
I included the other surgeon’s imaging if that helps.
A: Based on your response to the larger imaging 9mms would be too big for you. That is my opinion as I would never place a 9mm chin implant in you or almost any female if they don’t like the predictive imaging.
The concept you have to grasp in that such implant selections are not an exact science and, even you the patient, don’t know how you will really respond to any size implant placed in you. Up to 1/3 of all facial implant patients ultimately change the size of their implants in a secondary procedure for a variety of reasons. That is the nature of facial reshaping surgery and the unpredictable psychological response of patients to changing the shape of their face they have looked at their entire life.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Could you ask Dr. Eppley how many millimeters is added to the chin on the first set of images and the second set of images? And how many millimeters you think is perfect in my case? I just want an idea. I feel better with the second set of images.
And whether the silicone he plans for me is the extended anatomical silicone that goes up my jaws or without wings.
During the consultation he said it’d be a v-shape silicone that he’d have to shave it into.. too much to ask but would he happen to have a picture of someone he did the same to?
I know you secure your chin implant onto the chin bone with a metal screw. If I ever need to do an MRI for whatever reasons, will that metal screw be a problem?
A: In answer to your chin implant questions;
1) Computer imaging is not really done by known millimeter increments. It is done by general ranges of changes. For example, the first set of imaging was probably in the 6 to 8mm range while the second imaging was in the 4 to 6mm range.
2) The perfect amount of advancement is the one that you like the best….which is why two different types were provided.
3) Most women do not like chin implants with extended wings because it makes their chin look wider from the front view. This is why for most women, unless they specifically request a wider chin, I use the anatomic style chin implants.
 4) All anatomic chin implants are a bit round by today’s female desires so I usually reshape that into more of a V-shape.
4) All anatomic chin implants are a bit round by today’s female desires so I usually reshape that into more of a V-shape.
5) Any screws used are made of titanium, a non-ferromagnetic metal. So it has no interference with MRI studies.
Dr. Eppley
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’ve got a quick question today (am planning to come back to you later for a thorough evaluation). Regarding the chin implant, you have written about how the submental incision scar usually heals up quite nicely. Will this remain true for darker skinned patients as well?
A: Skin color makes no difference in the submental incision scar healing in my experience. In fact the darker the skin pigmentation is the better the scar does from my observations.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, ‘m considering a jaw implant on my right jaw. My situation might be a little untypical compared to a typical jaw angle implant patient, so let me explain my situation.
Several years ago I had a cyst removal from my right jaw. This removal surgery changed the way my right jaw angle looks. I feel that before the cyst removal my right jaw was more angular, wider, better looking. The problem is worse the slimmer I am: the slimmer I am, the worse the right jaw looks.
I’m happy with the way my left jaw looks, it hasn’t changed at all.
One thing that I have to clarify: I want my right jaw to look more angular. It doesn’t have to look like it looked before the the cyst removal operation. I want it to look as good as possible. If it looks the same as before the cyst removal, good. If it looks different but better, that’s even better. The goal is to make my right jaw look as good as possible – the goal isn’t to make it look like it was before the operation.
So basically I want my right jaw to look better. Maybe later I can consider a left jaw implant, or it might be that I’m happy with my new right jaw and I don’t need a left jaw implant. I also realize that my jaws won’t be symmetrical, but it won’t bother me too much – and if it would bother me, I could get an implant to the left jaw.
1. Is it possible to insert a jaw angle implant only on the right jaw? If so, would it be off the shelf implant or a custom one?
2. If I decide that I want a jaw angle implant on my left jaw after the right jaw operation, is it possible?
A: Thank you for your inquiry and detailed explanation of your objectives. In answer to your questions:
1) There is no problem with just placing a right jaw angle implant only.
2) Whether that would be a standard or custom jaw angle implant depends on what the bony anatomy looks like. This requires a 3D CT scan to determine.
3) A left jaw angle implant can be placed secondarily.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Several years ago I had a sliding genioplasty and my jaw augmented with hydroxyapatite paste. I was unhappy with both as I still lacked horizontal and vertical chin projection and the HA paste on the jaw area was uneven. I tried to have it removed later but he was unable to remove the HA as he said it had integrated too much with my bone and tissue and was at risk of damaging nerves etc if removed. Instead he added pieces of Medpor under my chin to increase height and also placed Medpor pieces either side of my chin to fill gaps left from the genioplasty.
My question is, as someone who is more familiar with HA paste would you be able to remove the HA and Medpor and replace it all with a custom wraparound jaw implant?
A: Between the HA paste and the Medpor pieces added to your jawline the situation has become very difficult for successful efforts at complete removal of both. Quite frankly, on the surface, it is not very appealing surgery with increased risks of marginal mandibular facial nerve branch injury due to the location of the Medpor pieces. Removal of HA on the jaw angles is more of an issue with access, not a risk of any nerve injuries. When HA paste gets jammed back onto the jaw angles that is a convenient placement technique but not a removal one.
A more qualified opinion, however, would require a 3D CT scan of your lower jaw to really see what the internal bone structure now looks like.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am looking for v line reversal surgery. V line results are not good. I didn’t ask to shave my jaw like that. My face looks shorter and narrow and uneven jawbone cut.
I had fuller face. I want to get my face back. Please let me know if this is something you can do for me.
Thank you
A: Thank you for your inquiry and sending your pictures. V-line reversal surgery is a procedure of which I have great familiarity having seen many such requests. Traditional v line surgery amputates off the vertical length of the jaw angles (ramus) and body with some form of bony chin reshaping. When people seek its partial or complete reversal they are seeking restoration of the missing vertical length of the jawline in most cases. This can only be done with a custom jawline implant design made from the patient’s 3D CT scan. While the actual bone shape before the surgery may never be known completely (unless you have a preop 3D CT scan or panorex…which many patient’s do) good estimates can usually be made.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My jaw stopped growing at a young age due to Juvenile Rheumatoid arthritis. I would really like to get my chin and jaw to look more normal. I am not sure what procedure or procedures I will need. Thank you for answering back with the cost of the custom jaw wrap implant. I was on the website and saw pictures of patients that had genioplasty and chin implants. I’d like to know which would be best. If genioplasty and implant would be best, I’d like an approximate cost for everything. Thank you!
A: Thank you for your inquiry and sending your profile picture. When you have a skeletal jaw foundation that is so short from a congenital/medical basis the first question is whether you are a candidate for orthognathic surgery. (double jaw surgery with lower jaw advancement) That is not a question that can be fully answered by looking at a picture. This requires a full orthodontic evaluation/workup which you may or may not have had. In an ideal world this is likely the best approach for your severe lower jaw deficiency.
Any ongoing comments are based on the premise that orthognathic surgery is not option you are going to pursue and a ‘camouflage’ approach to the problem is being taken. (and one accepts their bite the way it is now) Thus a sliding genioplasty is the chin procedure you should have and it would like be of the jumping man variety. This is certainly the one basic procedure that would be of greatest benefit. An implant alone is not a good option for your chin as it is simply too deficient. There could be an option for an implant on top of the sliding genioplasty but never an implant alone.
The rest of the jawline, while having to be done with an implant approach (as there is no other way to do it), is going to likely require a custom jawline technique as the anatomy of your ramus and body of the mandible is undoubtably not normal and is most likely asymmetric as well.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a sliding genioplasty surgery about 4 weeks ago, advancing my chin 8mm and 4mm vertically. However, I’m really unhappy about the result as my face is too long and my chin looks pointy whevever I open my mouth. I am 19 years old (male) and would like to know if the procedure can be revised to decrease the vertical height by 2-3mm and the horizontal height by 2-3mm. Please could you advise if this is possible and what the risks are. Attached are photos where it looks too pointy and long.
Kind regards
A: Certainly your sliding genioplasty can be revised/positionally adjusted. I suspect it is largely the vertical lengthening that is at fault but moving it back a 1mm or 2mm would not hurt either. I would say the most significant risks of the procedure have already passed (permanent nerve injury) so a secondary early genioplasty does not increase that risk since the bone cut has been already made. You just need a new plate (6mm one) and some allogeneic bone chips to ensure good bone healing.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question about my eye area. My eyes look quite feminine and weak despite good palpebral fissure length. My lower eyelid look quite round. I noticed that I have bad upper eyelid hooding and my upper eyelid looks round. I show examples of masculine,alert eyes I wish I could achieve. First example is my eye area.
Another question is if its possible to lowering entire brow bone and push eyebrows lower. Also is it possible to change orbital rims shape? I asked one surgeon before and he told me for infraorbitals is possible to get 2.5-4mm of vertical augmentation and up to 6mm of horizontal augmentation and for supraorbitals is it possible to move horizontally up to 4mm and there is a problem for lowering cause you have to release some skin from forehead or use expander to make place for implant and in that case even 7mm of vertical augmentation can be achieved.
Thank you.
A: I would generally agree using custom implant designs with the following statement ‘ for infraorbitals it is possible to get 2.5-4mm of vertical augmentation and up to 6mm of horizontal augmentation and for supraorbitals is it possible to move horizontally up to 4mm.’…..with the exception I have seen brow bone augmentations that are much greater.
I would also agree with the statement that ‘there is a problem for leyebrow lowering cause you have to release some skin from forehead or use expander to make place for implant and in that case even 7mm of vertical augmentation can be achieved’ ….with the exception that I have seen eyebrow lowering of a few millimeters just with brow bone implant augmentations alone that have a vertical inferior lowering design.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have linear scleroderma of the chin. I have been seen by rheumatologists and dermatologists who recommended methotrexate or a biopsy; neither of which I was keen on. I believe I’ve had this since I was about 15, perhaps younger. I’m currently 19 years old. I was wondering what you would recommend for me? HLA fillers (temporary or permanent) or something else? I would love to be in a case study receiving treatment.
A: Thank you for your inquiry and sending your pictures. Assuming your linear scleroderma deformity is stable there would be no indication for pharmacologic intervention or for a biopsy. While there is certainly nothing wrong with the use of synthetic injectable fillers, they would not be a cost-effective long term solution. I would recommend the following two options of either external fat injections or the intraoral placement of a dermal-fat graft for contour restoration of your chin.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, with a sliding genioplasty and a chin implant, what’s the most amount of vertical length you could reasonably add to someone’s face?
A: My experience has been that 10 to 12mms per vertical opening wedge bony genioplasty can be achieved in a single surgery. This leads to uncomplicated bone healing. I have done a second stage opening bony genioplasty for one patient to ultimately achieve a 20mm total vertical chin lengthening. An implant can not be used with a vertical lengthening bony genioplasty.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Four years ago I had a soft tissue reduction performed on my soft tissue chin pad. It was an intraoral thinning reduction. I was unaware at the time and the doctor did not communicate to me the level of potential for soft tissue contour deformities. The soft tissue took a long time to heal with edema in the excision site for months. Unfortunately, the soft tissue pad is now quite uncontoured and has an irregular shape from the surgery, and it seems as though the chin pad is not attached very well to the bone as it is hyper mobile and bags at the middle section of the chin. It is possible that some mentalis muscle was removed in the excision, I am unsure. I now have soft tissue chin balling to some extent. I have shown in the photos how the soft tissue lifts off the bone if I tilt my head or push the tissue up.
I have been to multiple surgeons since in pursuit of soft tissue contouring or tightening and or chin reduction. From the x-rays, it is obvious that the bone is not the primary contributor to the horizontal projection, but I have a significant soft tissue excess. In the photos, I have tried to show how the bottom point of the chin is very steep and meets the mid point of the chin (most prominent area) at a very steep angle. It is more pronounced on the right side than the left as the right side seems to have a slight deficit of tissue or is just irregularly shaped now. When i grow out my beard the tissue on the top / middle projects significantly and is a constant nightmare.
I fear that it may be hard to perform a submental tuck up with the bone as the bone still sticks out and due to the steep angle at the bottom. Maybe somehow with bone repositioning or something the tissue could be draped over it and tightened to create a more contoured appearance. I imagine there would have to be some kind of muscle resuspension too to get the chin to stick down. I have tried to show you all the angles in the photos and have demonstrated pulling down from underneath. The tissue will not come down over the bone perfectly as it is. I also have a little bit of submental fullness or skin excess which may make a submental tuck hard to perform. I have been turned away by other surgeons obviously because any procedure to the bone will result in a horrible soft tissue outcome. I am quite unsure about it and whether anything can be done. It is obviously a highly risky and difficult surgery. The photos do not completely demonstrate how the tissue is mis-shaped.
A: Thank you for your inquiry and sending your pictures to which I can say the following:
1) Intraoral soft tissue excision is never a good approach for the exact reasons you have observed. But that is past history.
2) The only new piece of information I can provide you is that you have a very flat mandibular plane angle. (chin and jaw angles on same horizontal plane) People that have such flat plane angles often have a soft tissue chin pad protrusion because the chin is actually vertically short. From my perspective the better approach initially and even now is vertical bony chin lengthening. That will do more for the soft tissue chin pad by stretching it out (unfurling it) than any further attempts at soft tissue reduction/manipulation on its own.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I attached photos some of myself from different angles, a morph of myself in the profile view with a possible rhinoplasty and a few “desired aesthetic” photos. Thank you!
Background:
•I believe I have a weak chin from the profile view and I am unsure if my chin is too short from the front view
•I did breathe through my mouth as a child. As an adult I do not typically breathe through my mouth, only occasionally when I sleep I believe I do
•I had braces when I was around 11years old and it was done by my dentist.
•The middle split in my front tooth seems to be off center with respect to the center of my lip
•One side of teeth seem to be higher than the other side
•I plan on doing rhinoplasty prior to a genioplasty or jaw surgery
•I am looking to get a more defined jawline and a stronger chin that is still feminine
Questions:
1.Out of curiosity, why was genioplasty recommended over a chin implant?
2. Based on my history and photos, is jaw surgery recommended, or would a genioplasty and shaving down one front tooth suffice?
3.Is the morph I created possible/recommended?
4.Would genioplasty be able to give me a more defined jawline?
5.Is it recommended to get rhinoplasty or genioplasty first?
6.How much improvement should I expect for my lip incompetence and mentalis muscle strain with the genioplasty? Is there a way to completely or mostly remove these issues?
A: Thank.you for sending your pictures. In answer to your questions:
1) Give the shortness of your chin and to prevent it from becoming too wide, if you were only doing chin augmentation a sliding genioplasty would be the preferred method. Your chin deficiency is at least or close to 10mms which is beyond what most chin implants can do. It is also important in a female to keep your chin narrow. A sliding genioplasty will improve symptoms such as lip incompetence and mentalis strain far better than an implant.
2) You can not make the determination about whether orthognathic surgery (lower jaw advancement) would be indicated based on facial pictures alone. This requires x-rays and an occlusal assessment.
3) To do computer imaging I need all three facial views particularly the side view of you…which is not in the pictures sent.
4) Genioplasty improves the chin…not the jawline behind it. No form of chin surgery makes a better ‘jawline’. Most people when they refer to jawline mean the back part of the jaw or jaw angles. That requires a different procedure than any form of chin augmentation.
5) The order between rhinoplasty and genioplasty is a personal one. There is no right or wrong order. It is all about what you value first.
6) While a sliding genioplasty will help with lower lip incompetence and mentalis strain there is no predicting beforehand how much it will improve.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had lower jaw surgery at 17 to correct my overbite. My orthodontist said since I grew up with an overbite it cause the deep labiomental crease. It makes me very insecure and I am interested in solutions to fix it, without making my chin bigger since I am scared of it appearing more masculine. I’ve heard fillers and fat grafting sometimes don’t last or have much of a difference. I am interested in what you have to say in what would be appropriate for me. Thank you
A: While your labiomental fold is deep I do not see any need for chin augmentation. Your chin has adequate projection for a female and any more, as you have rightly stated, runs the risk of making it look too masculine. Your focus should be on treating the deep labiomental fold. The first place to start is to have injectable fillers done and see if you like the change. If so then you can graduate to a more permanent method such as release with interpositional composite fat grafting.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’ve always found my forehead to be very irregular, and last month I visited a maxillofacial surgeon in Brazil. He diagnosed me with non-treated Trigonocephaly (although a very soft one).
My forehead is indeed a bit triangular, and I have a ridge on the very top of the forehead, in the hairline, although I never experienced any neurological disorder. I’ve attached some pictures.
He suggested two different treatments:
1) Customized facial implant, made with a 3D CT Scan
2) Non customized implant (made of bone cement by the surgeon)
He advised the Customized facial implant (made of soft material), as the incision is smaller and results are more predictable. I found you on the internet as a reference for customized implants.
What type of material do you use? I saw many possibilities, such as PTFE, POREX, PEEK, Titanium, Silicone. I worry about the size of the incision, as my father and grandfathers are bald, but the doctor said he would need to cut across the entire head to open and cut (reduce) the ridge on the top anyway.
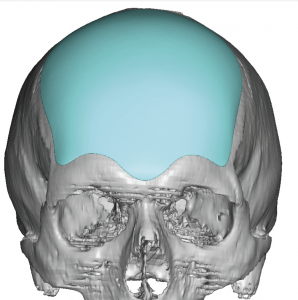
 A: Thank you for your inquiry and sending your pictures. I don’t think there is any question that the superior method for your forehead augmentation is with a custom implant for two compelling reasons: 1) the incision needed to place it would be very small (unlike bone cements which would require a full coronal scalp incision) and 2) the shape precision need for any forehead augmentation shape is very high and unforgiving. Trying to get the proper shape by hand (even if one could accept the coronal incision) is very difficult to do. It is far superior to spend the needed preoperative time in a computer design where the effects of the changes can be better appreciated. This results in a far lower risk of revisional surgery due to shape/contour issues.
A: Thank you for your inquiry and sending your pictures. I don’t think there is any question that the superior method for your forehead augmentation is with a custom implant for two compelling reasons: 1) the incision needed to place it would be very small (unlike bone cements which would require a full coronal scalp incision) and 2) the shape precision need for any forehead augmentation shape is very high and unforgiving. Trying to get the proper shape by hand (even if one could accept the coronal incision) is very difficult to do. It is far superior to spend the needed preoperative time in a computer design where the effects of the changes can be better appreciated. This results in a far lower risk of revisional surgery due to shape/contour issues.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I also have a really slanted forehead so the top of my head looks very Neanderthal-like. Throughout my high school I’d get called a Neanderthal or homosapien and I’m looking at pictures of me from when I barely started high school and I didn’t have that huge brow bone and my forehead was slanted at a right angle, but I understand that genes play a big role too. I saw a post of a patient you had and my head shape is very similar to that and the after results were fantastic! I want my forehead to look slanted but not too slanted. I would like to know how risky this procedure is and well, you’re the doctor so I’d like more information on this.
I’ve even edited before and after photos of my side profile to show how I want my brow bone to be and I really want you guys to be honest with me and let me know if my look is possible 🙂 another question I have is after my brow bone gets shaved will it make my eyebrows be shaped differently? Cause I like how my eyebrows are shaped and all and does this procedure require the big incision that goes all around my scalp or do you guys also do the small incision at the top of the scalp?
A: Thank you for sending morphed images. What you are showing is a combined brow bone reduction with upper forehead augmentation. Such a result is very possible and this is a common procedure in my practice. This is not a risky procedure and is done through a scalp incision but not one that goes from ear to ear. (coronal scalp incision) Reduction of the prominent brow bones does not change the shape of the eyebrows.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I gather from the website that you do testicular enhancement surgery.
What is the implant made of? I read the details of the configuration (like a clam shell, fixed in place around the existing testicle). Does it have a natural feel? Is it detectable by airport security.
How many days would I need to be in Indianapolis? I assume it’s an outpatient procedure.
Typically, how quickly can one expect to book an appointment?
Thanks in advance for your response.
A: Thank you for your inquiry for testicular enhancement surgery. I would first direct you to my website, www.exploreplasticsurgery.com and search under Testicle Implants where much has been written on this topic in great detail. To answer your specific questions:
1) All testicle implants are made of an ultrasoft solid silicone material.
2) Such materials have a natural feel which is why they are used.
3) Silicone is not a detectable material by x-ray metal scanners.
4) You would go home the day after surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi! I’m pretty sure I have Vertical Orbital Dystopia as you can see in the picture. Saying this bothers me would be a huge understatement, I’m 20 years old (no health issues), haven’t been in a picture for at least 8 years and can’t look at someone in the eyes because I’m ashamed. I’m desperate to fix this. Obviously I’m not looking for perfect symmetry, but I want to have “normal” asymmetric eye. Seeing all the pictures on your website, I’m really interested and would like to know how much this could cost me and if this is a dangerous procedure. Thank you!
A:Thank you for your inquiry and sending your picture. Your diagnosis is correct (vertical orbital dystopia, VOD) and its magnitude is aesthetically significant. (probably 5mms) The entire right orbital box is lower. This means the brow bone and cheek around the eye are part of the skeletal asymmetry and must be included in the treatment approach. While a preoperative 3D CT scan is needed for proper treatment planning, the concept besides raising up the floor of the eye is that the brow bone above needs to be vertically reduced and the infraorbital rim and cheek below need to be raised as well. In addition you can’t just raise the eye and adjust the bone around it without factoring in adjusting the upper and lower eyelids as well. (if you move the position of the window the overlying shade must similarly be adjusted or the window will look unusual/distorted)
While this sounds like a major undertaking, and it is, but this is the normal collection of procedures that are needed in significant VOD surgery. This is not a dangerous procedure, it is more a question of the magnitude of the asymmetry that can be achieved. It would take looking at the scan to provide a more qualified opinion in that regard.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m thinking of mandibular implant and maybe buccal fat removal. When you see my pics what do you say? In the pictures from 2015 I was working out very heavily and biting my teeth so that the “mandibular” grew bigger. You can see it gave results and my jaw appeared wider. If you look at the picture from 2016, on that picture im’ biting my teeth together and doing a “zoolander pull” with my cheeks and lips. (cant find the correct word in english). That look in the 2016 picture is a look I think look very good on me, do you think that look is possible to achieve?
I think unfortunately that I have aged a little bit since 2015 and I feel that my cheeks has fallen down a little bit, do you see that too? Maybe I need some kind of face lift? Especially my right cheek I feel has gone down. Little to early maybe with facelift, I’m only 33 years old.
My fat percentage is right now at 12%, it was the same in 2015.
A:Thank you for your inquiry and sending your pictures. In the spirit of trying to achieve the 2015 ‘sucked in cheek, biting down jaw angle look’, which is commonly requested I would not disagree that midfacial defatting and jaw angle/jawline implant would be the only way to try and achieve it in a non-induced/artificial manner. In regards to your cheeks you are too young and do not have enough loose tissue to justify a cheek/midface lift and the scars to do so. It would be more effective and scar free to do high cheekbone implants which provide their own cheeklifting effect.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, If you are an active person and are into contact sports like mma or football, are the implants still safe to have? For example, I am really into CrossFit and we do a lot of handstand push-ups where my head hits the floor each rep. Can this cause complications long term in a skull implant? Provided that I take the proper post op rest and recovery precautions getting back to training.
A: This is a common and understandable question. Once healed I do not see any contraindications to contact sports with either skull or jawline implants. They are very much like placing ‘bumpers’ on the bone which provides some added protection. It would take an incredible amount of force to ever displace them. That being said, repetitive and avoidable trauma to an implanted skull or facial area should be avoided as no one can predict every adverse effect that could occur.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m looking at sliding genioplasty or chin wing osteotomy. I originally was most interesting in jaw surgery bc I have a slight lisp when I speak along with a recessed maxilla. …..but it depends on how long braces would be on. I just finished smile direct and my teeth are straight and my bite seems to be normal. Would love to get in contact! … I currently have jawline and chin filler in my pics which I’m dissolving soon.
A: Thank you for your inquiry and sending your pictures to which I can say:
1) You are not a candidate for orthognathic surgery as your bite is fine and you have normal facial bone balance. You have an aesthetic jawline deficiency.
2) You are not a candidate for chin wing osteotomy as that procedure does nothing for the jaw angle area and you do not have a vertical jawline deficiency.
3) Your options for total jawline enhancement are either a sliding genioplasty combined with vertical jaw angle implants or a custom jawline implant, each of which has their own advantages and disadvantages.
Dr. Barry Eppley
Indianapolis, Indiana