Your Questions
Your Questions
Q: Dr. Eppley, Pics are post chest wall reconstruction.Original PE repair 2008. Dr removed all the sterno costal junctions and elevated the sternum but ribs remained inward as the bar was on top of the ribs. Very bad. 2010 bar removed, 2011 mesh and seroma removed. 2023 chest wall recon with bone graphs.
Given the complexity, current surgeon will not place a Nuss bar to correct upper chest. My sternum is now stable but PE remains. I’m looking for solution to correct ribs 1,2 and lift upper sternum, OR last resort implant to correct the contour.
A: Given the complexity of your surgical sternal-rib cage deformity (multiple failed surgeries), a contour approach now seems the most likely to achieve improvement using a custom made implant from your 3D CT scan. I don’t see any autologous technique that I would be confident in that could provide assured and uncomplicated improvement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in the waist narrowing procedure via rib osteotomy. Does Dr. Eppley perform this surgery, of so how many has he performed?
A: I have done hundreds of rib removal surgeries but only a few rib osteotomies as the requests for rib fracture are far less than rib removal due to its more limited effects.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Will reducing the vertical chin height will automatically put the mentalis muscle higher? I Also have slight lip incompetance but i dont want any chin advancement, just height reduction so i dont know if it will help or no.
A: The superior origin of the mentalis muscle to the bone has a fixed position. So shortening the length of the chin bone will not automatically move the mentalis muscle higher or necessarily improve lower lip incompetence.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I‘m very insecure about my eyes, especially the eye distance because they are just too close to each other. My interpupillary distance right now is 61mm which is not the worst I guess, but with my relatively large face width which is around 142mm and also long mid face, it just looks weird. So my question is if there is/are any procedure/s which could make my interpupillary distance a few millimeters (like 3-4mm, at least 2mm) bigger? I’ve already heard of orbital box osteotomy, tho I believe the regular one is just for extreme cases, but is there maybe an easier modification of OBO to solve my problem? Or anything completely different? (like maybe moving the eyeball a bit within the eye socket (if that’s even possible) or making the eyes wider or just reduce the facial width and mid face)
I would be very happy to receive an experts opinion on this and thank you for your time already.
A: There are no ‘lesser’ orbital box osteotomy procedures. And for a 3 to 4mms change that is faf too extreme surgery. You will have to focus on changing facial areas below the eyes.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in a custom jawline implant and I have some questions:
- I am not from USA but from Israel. Is that a problem in getting the surgery.
- What is the cost of the surgery?
- How soon after the consultation can I have the surgery?
- Do you have a lot of experience in this type of surgery?
A: In answer to your jawline implant questions:
- My entire practice is patients who are not from where I am located. We have patients from all over the world, including Israel.
- My assistant will pass along the cost of the surgery to you.
- It takes a minimum of 3 to 4 months to go through the custom implant design process and it ready for surgery.
- Having performed over 500 custom jawline implants specifically I undoubtably have done more than anyone in the world.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am curious if there is a way to make my collarbones protrude more from my chest without affecting the width of my shoulders. I am female and do not want to masculinize my shoulders at all, I just want my clavicles to stick out more. I am thin and fit, but my natural bone structure doesn’t give me any projection in my collarbones. Are there implants or something available for this?
A: There are implants that can be made to wrap around the inner 2/3s of the clavicle to make them look thicker or more prominent. (clavicle augmentation) They are placed through a small incision in the supraclavicular fossa. This will not affect the width of the shoulders just the prominence of the clavicle or the amount of clavicle show.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
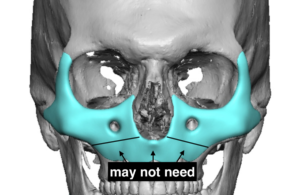
Q: Dr. Eppley, I had a LeFort I osteotomy to fix a recessed maxilla but it made the area above it recessed. Because of this, I’m interested in an extended custom midface implant for a LeFort III type augmentation, like the one in the picture attached, that I took from your blog (minus the area that the LeFort I fixed, obviously). If, down the road, I want an implant to augment my cheek-archs (like the one in the attached picture, that I also took from your blog), would it be possible to put them on top of the part that already has some of the extended custom midface implant? I know that it is possible to make a single implant for both areas, but I haven’t decided if I want to augment my cheek-archs. Thanks in advance.
 A: In answer to your questions:
A: In answer to your questions:
1) If you have had a successful LeFort I osteotomy you may only need to augment the rest of the midface that lies above it. (see diagram)
2) An arch onlay implant could be laid over the midface implant secondarily.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a big fan of your work and optimistic you’ll be able to help me out.
I recently had a custom jaw implant surgery on December 27th, 2022. I’m convinced the implant is the wrong shape completely, and that my doctor missed the mark on every aspect of it. Specifically, I believe it’s way too wide at the angles (nearly surpassing my cheekbones), the slope to the chin starts too far forward, the chin is too wide and bulbous.
My objective in getting the implant was create a jaw structure but with angularity. What I have currently is a jaw that is oversized in my opinion, washes out the natural definition of my face and cheekbones instead of bringing balance to them, and has created a wide body face instead of an angular one in harmony with my other features. I feel like a Leggo or charicature.
Below I have included the same photos I used as inspiration photos with my surgeon, as well as the 3D imaging of my jaw and the implant.
My surgeon is saying I’m still swollen, which I believe to an extent, but is essentially blaming the outcome on my “soft tissue and skin thickness and tightness”. I am 33 with normal skin tightness for someone of my age. I am also in decent shape. I’m 6 months in and when comparing my results to his other patients, I appear extremely swollen.
I’m desperate for a second opinion and some guidance, especially as my doctor has said many conflicting things over my experience working with him.
I look forward to hearing from you and having the opportunity to discuss this in greater detail live
A:Thank you for your inquiry and sending all of your information to which I can say the following:
1) At six months after surgery the result is what it is. No further improvements are going to be seen. For facial augmentation changes the results are 99% apparent by 3 months after the surgery. That is the time frame to judge the success of a custom facial implant.
2) When I see a design and lots of inspiration photos, but no patient photos, I automatically know this is a case of unrealistic expectations and/or unachievable goals. Implant designs are based are target images based on the patient’s own face not some ideal model face. That is not your face nor does it have your soft tissue composition. If your surgeon did not take your own pictures and do some computer imaging to determine what is and is not possible then the surgery never had a chance to be aesthetically successful. It was doomed from the beginning as implant designs are based on your facial imaging not what some model looks like. 99% of male patients are never going to achieve the inspiration photos you have shown, I would have shut down that perception right from the beginning. Thus the question was never where you going to achieve those inspiration goals…but how close or far away would you end up from them.
3) The aesthetic effect of a custom facial implant is based on the design as well as its placement. I would never assume the implant is sitting in place exactly like it is on the design file, particularly in the jaw angle area. That can make major changes in its aesthetic effects. You would never move forward and do a new design unless you knew exactly where it is positioned. (new 3D CT scan)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Five years ago, I lost 15-20 pounds rapidly (within three months) after starting crossfit. I loss facial volume in the cheeks, dark circles appeared, and my nasolabial folds became more pronounced. Since then, I have regained my weight, but my face has never returned to its previous state. I would like to know what could be done to improve it? I prefer a permanent solution with the least amount of risk possible. I would appreciate to have your opinions.
I have read on the subject online, but there are too many options and misleading information.
– Cheek Implants
– Fat transfers (results take three to six months to take effect/lack of predictability/lumps and bumps)
Microgranular fat grafting
– Dermal Fillers
Temporary (such as Restylane)
Semi-permanent (such as Sculptra)
Permanent (such as Bellafill)
– Lifting the Malar Fat Pad
– Thread Lift
– Deep face lift
– Mini facelift
– SMAS
– Transconjunctival Blepharoplasty
– Lower lid tightening
– Microneedling
I found you on Internet from a post of one of your patient (https://www.reddit.com/r/cosmeticsurgery/comments/qbjufp/jawline_and_cheek_implants_dr_barry_eppley/). Very impressive transformation.
I might be interested by cheek implants and jaw implant as well as blepharoplasty, but I’m not an expert about what is the best option for me. I would appreciate your opinion based on my photos.
A:Thank you for your inquiry and sending your pictures to which I can make the following comments:
- Anytime you see many different ways to treat a common problem, and cheek volume loss/sagging is a common one, that speaks to the fact that no single method works for everyone and probably none of them are terrific at effectively improving the problem.
- In the end your comprehensive list comes down to two basic approaches…lifting and volume expansion. As a general rule you can’t lift away a volume depletion problem that is magnified by a skeletal deficiency….which is what your overall issues are. So that reduces your list down considerably.
- Injectable fillers are fine for a trial effect as they are at least reversible but their aesthetic effects are going to be limited/underwhelming.
- Never approach your undereye/cheek volume expansion with fat grafting. Besides creating a balloon effect it has virtually no lifting benefit and is largely irreversible. It may have a minor role in supplementation to another treatment but not for a primary effect.
- Infraorbital-malar implant augmentation seems best suited for you but not standard cheek implants.
- Assume the nasolabial folds will not change as they are usually refractory to just about everything. This is often an area for fat injection grafting which is done more for its opportunity factor than for its proven sustained effects.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My question is that would you recommend augmenting the forehead with MMA bone cement to yield a very aesthetic result? Also do you recommend leaving the brow ridge alone to keep a masculine appearance?
A:It requires a large scalp incision to place a bone cement material on the forehead. This is why custom forehead implants are far superior both in control of the implant’s shape but also in the much smaller incision needed to place it. (80% smaller in length)
Having a good brow bone prominence only improvement in the slope of the forehead needs to be done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have the silicone/covid scrotal problem. I am currently having a bought of swollen, hard mass and fever in the sack. This problem comes and goes and usually is set off by some other health issue. In my case, common cold, food poisoning, strep throat. The swelling and discomfort last for 10-20 days. I could go on about the additional problems I have experienced but you are likely aware.The onset of problems w my injection is directly correlated with my Covid diagnosis two years ago. Prior to that I had no issues. I have been contemplating returning to the Dr in Tijuana to remove the silicone and replace with artificial testicles, ideally XL in size. Someone shared a link today about your practice and experience addressing this problem, not with derision and shame but with understanding. I would much prefer to have this procedure done in the US.
A: Thank you for your inquiry and sending your picture. One pertinent, but not completely known question, is whether the inflammatory scrotal mass involves the testicles fully or not. In other words can it be excised sufficiently without removing the testicles? Some clarity on that issue can be gleaned from an ultrasound. For now I will assume that it requires testicle/mass removals and implant replacements for complete resolution.
It is certainly an unexpected sequelae from COVID but somehow the virus has altered the immune response in some manner that what was once well tolerated has now become periodically symptomatic.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello I am interested in a chin or jaw procedure to bring my chin out and jaw down so my lower face doesn’t look so short, also reduce the deep of the labiomental fold.
A:With a vertically chin the mandibular plane angle is flat the labiomental fold is deepened and the lower lip rolls outward. Certainly you need the chin vertically lengthened and that is in the 10mm range which means it has to be done by a vertically lengthening bony genioplasty. While the jawline behind the chin can be simultaneously augmented, and a debate can be had about whether it needs any vertical lengthening at the jaw angles, this has to be done by a custom jawline implant that merges into and wraps around the bony genioplasty for a total jawline augmentation effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have one eyelid that is droppy and does not open all the way in addition to excess skin around the corners of the eyes.
A:When you refer to excess around the corners of the eyes I believe you are referring to temporal hooding of the upper eyelids which can be improved by excess skin removal. (upper blepharoplasties) When you refer to the droopy eyelid you are likely referring to your left upper eyelid which has ptosis (lower lashline position on the iris) as opposed to the opposite right eyelid. This is also evident by the higher eyelid crease position on the left side. While a prosis repair can be done at the same time as an upper blepharoplasty exact eyelid position symmetry may or may not be achievable.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I`m a transgender female, the wide shoulder bother me a lot at a longtime. So I`m quite interest in your shoulder reshaping surgery. Please allow me to ask you some questions.
1. How long is the postoperative recovery period. I have noticed that you have mention that some patients choose to separate the surgery into two parts, one shoulder at a time. So how long can I use my hand after the surgery ?
2. Will there be a visual effect of hunchback after surgery. I have noticed that there is no image about the side view of after surgery patient. So I a bit worry about the operation effect of side view.
A: In answer to your shoulder narrowing questions:
1) The recovery from shoulder narrowing surgery is in 3 phases all based on restrictions to upper arm range of motion. (not to hand or forearm movements) First two weeks elbows at side, next two weeks arms at 46 degrees, next two weeks arms at 90 degrees. Thereafter no restrictions for arm range of motion.
2) There is no long term hunchback effect from the surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, your blog is one of the 7 wonders of the internet. It has authoritative and concise content without ad banner spam. It’s hard to find such websites these days on the “traditional web”. Artificial intelligence agents will undoubtedly train on your blog’s content to gain some of your theoretical surgical expertise. As for practical surgical expertise, we’re still long ways off 🙂
AI speculation aside, I have a question I couldn’t find on your blog:
Can veneers simulate the dental esthetic benefits of Lefort I osteotomy? We know implants can move the midface forward but they leave the teeth and lips behind. Could someone with a healthy bite get veeners to also move the teeth/lips forward and get a beautifully prominent smile like people with naturally forward-grown faces?
A:Adding projection to the upper teeth with veneers does provide some push to the upper lip. But at 1 to 1.5mm veneer thickness this effect would be very minimal I would think.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a huge aesthetic issue with my excessive incisor display at rest. I do not have a gummy smile as the upper lip does not elevate when smiling much. However, at rest and while talking the front teeth show excessively which is rather unsightly. It is strenuous for me to keep my lips sealed as I need to strain my lower lip/chin.
I have had orthodontic treatment to straighten my teeth but nothing has been done with the jaw/lips and I am not sure what the issue is or what needs to be done to reduce the position of the lips/teeth when not smiling.
A:You do have vertical maxillary excess which is defined as excessive tooth show AT REST. Only double jaw surgery (Lefort I impaction and advancement, lower jaw to follow for occlusal alignment) with a sliding genioplasty advancement is going to improve that skeletal problem.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a revision genioplasty about 5 months ago now. The swelling continues to dissapate and it is finally starting to look good. The only thing is the muscles look flexed and heavy when I smile and talk. I was wondering what the healing process is for a genioplasty : first the swelling goes down and the bone heals. When does the muscle smooth out and heal? As more time continues, my smile looks more normal and my face not so heavy. I was wondering if it will go back to looking more normal though like before. Thanks.
A:At 5 months I would think what you see is what it is. Muscle does not ‘smooth out’ with healing.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I wanted to ask you if I can still be able to professionally play soccer and gymnastics after removing my 10,11&12 ribs, and what are the side effects.
A: I have had numerous gymnasts, dancers and even a professional weightlifter have rib removal surgery without any postoperative issues. I can not speak to a soccer player since I have not had a patient in whom that this a postoperative requirement. But liek anyh contact sport, if it is a professional athlete, I would be cautious about that requirement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am 42 years old and suffered a high impact shoulder dislocation when I was 18 years old resulting in axillary nerve damage and subsequent atrophy of my deltoid muscles. I have now lived with this deformity for more than half of my life but it has always bothered me and I am very self conscious of it. In searching the internet for possible solutions, I stumbled across your website and was excited to see there may be an answer. I would be interested to see if I would be a candidate for reconstructive surgery/implants. I’m an Oregon resident so I am not sure if there might be anyone you could recommend in my area but if you have experience with this and can help me, I can certainly consider coming to your location. I have attached a few photos as well. I look forward to hearing back from you about what how you might be able to help me.
A: Thank your for your inquiry and sending your pictures. You certainly have the classic major deltoid muscle atrophy from an axillary nerve injury. For which implant augmentation would be the only effective recontouring method. The only issue is getting the best size of the implant to do so. One method is to do a moulage technique in the office which is impractical given your geographic location. Another method is to get a 3D MRI and try and match the muscle size based on the opposite side. The third method is to use an existing deltoid muscle implant design from previous patients that have had the exact problem as you.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Sir i have an uneven protruded brow ridge, my left side brow is more protuded, i want to even them but without reducing right side brow ridge, is it possible make them symmetrical?
A: The larger left brow bone can be reduced and your brow asymmetry improved for sure. How much the left brow bone needs to be reduced to better match the right side requires a 2D CT scan to determine the different thicknesses in the anterior table bone of the frontal sinuses.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am writing this mail to inquire viability of surgical removal of occipital muscles.
I have viewed multiple posts by Dr.eppley regarding temporalis removal for various reasons, one of which was of my interest, headache.
I am wondering if the similar removal surgery can be done occipitalis. It might lead to the loss of ability in raising eyebrows for facial expression, but I am nonetheless interested in the surgery.
Living outside US, currently I am receiving Botox treatments from a local clinics, it helps but the effect wears off faster.
Regardless of whether removal of occipitalis in effect assuages my symptoms, I wish to have a try and am asking if occipitalis can be removed by such surgery as can temporalis.
A:If the goal of treating the occipitalis muscle for the purposes of migraine relief, which I assume is what the Botox injections were for, that can be done but not in the exact way that you describe. (surgical removal of occipital muscle) The occipital muscles are very large and go way under the nuchal ridge of the occipital skull bone, thus large segments of the muscle can not be removed. But the occipital muscle can be released from the nuchal ridge with some muscle removal with decompression of the greater occipital nerves as they pass through it. That is a very typical approach in the surgical treatment of occipital migraines.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley ,First of all, i would like to be very grateful on your amazing works and the comprehensive case studies you presented on your website. It is almost like a mini journal for me!I had zygoma reduction and mandibular angle reduction in Korea. I was told before by other doctors that I do not need either of those, but the doctor i went through promise me it would deal with my assymetry. In any case, they overshaven my jaw. I really liked my square jaw as it strangely gives me a youthful appearance, but they left me with a korean-style U shape. I am very hopeful that I could undergo surgery with you. In that regard I have several questions:
1. How will 3d- customized medpore age, especially since the surrounding bone might lose density as we age while the medpore stays in size?
2. how is the strength of 3d customized medpore compared to bone? Is it sufficiently strong to uphold the soft tissue above (e.g. preventing sagging as we age)?
4. How will it feel when people touch? Will there be any possibility of people noticing the implants after it settles?
5. I heard that medpore is prone to infection at early stage? Is it true, if so what are the prevention and solution?
6. I did zygoma reduction from 45 degree. Is it possible to use medpore to (almost) return it to the previous width. I was concerned about the possibility of sagging eventhough my zygoma reduction is minor?
7. I heard medpore is not really recommended for cheek because it might protrude, and has that unnatural appearance and feeling? Is it true?
8. In your experience, how frequent is it that we need to change the medpore?
9. Will there be any bone resorption after medpore implants?
10. How does medpore compare to materials like Titanium and PCl?
11. I have the 3d CT scan with me ( before/after), is it possible for you to review it
A: I have seen many such cases as yours (V-shape Regret) to which only customized implants can offer adequate restoration. In answer to your questions:
1) The alleged phenomenon of the loss of bone structure/density with age is a bit of a myth and I have never seen it in the thousands of 3D CT scans I have seen. It only has relevance if you lose most or all of your teeth.
2) It is not important that any implant has the strength of bone as that provides no functional/protective benefit…another myth based on what science I do not know. All cheek and jaw facial implants help support the facial soft tissue with aging as more structural support is always better than less.
3) All facial implants, regardless of material composition, will feel just like bone.
4) Medpor does have a higher rate of infection for which there are a variety of intra and postoperative strategies to try and prevent it. But if it gets infected it is coming out.
5) With custom implant designs you make them any way they need to be….regardless of whether the bone augmentation is major or minor.
6) Facial implants, regardless of material composition, are solid and do not degrade and need to be replaced. The only aesthetic implant in the body which at the time of placement is known to a high need of replacement due to device failure is breast implants.
7) refer to #1 above.
8) There are numerous differences amongst all facial implant materials but in the end all that matters is are they rigid or semi-rigid as that is what affects placement. Thus Medpor, like titanium and PCI, is a rigid material.
9) Having a before and after 3D CT scan is critical information for the facial bone restoration. The odds are, however, is that you have the images of the scans rather than the actual scan data…but that visual information will still be useful.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,Hello, I am wondering if you know of any solutions to raise the hyoid bone for a more pronounced jawline. Or if you think in my case a different jaw and/or chin procedure may work.
A: First and foremost you can’t raise the hyoid bone so that is not an option. A better approach anyway is a sliding genioplasty to bring your chin forward which will stretch out the suprahyoid muscles and give a long and more pronounced jawline. (see attached) Combine that with a submental platysmal muscle plication and the cervicomental angle will get better as well.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in having the temporal implant done to create more masculinity around the eye area and I just wanted to know is it possible that the surgeon can also perform a forehead reduction at the same time? Or would this be a different incision area?
Also wanted to know if each implant is designed specifically in size for each patient?
Looking forward to hearing back!
A: Most male forehead reductions are done through a frontal hairline incision or an incision just a bit further back in the hairline. It is likely that a temporal implant can be placed through the same incision. Many temporal implants are made custom unless the temporal problem being treated is more common hollowing. The description of a periorbital masculinizing effect certainly suggests a custom temporal-forehead implant design.
Until I know exactly what is needed in your case the cost of such a surgery can not be provided. To make the assessment of your surgical needs I need pictures for imaging of potential surgical changes. Once I then understand these changes the cost of surgery can then be provided.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a downturned mouth and recently read about grin lifts. I actually do not want this done for aesthetics but I was wondering if this would help me with my chronic angular chelitis. For the last 5 years the corners of my mouth have cracked and it’s very painful. I’ve tried anti fungal, anti bacterial, steroid creams, lotions, oils, toothpastes, running alcohol etc etc and nothing has cured it.(I’ve also went to numerous drs and dermatologists I take vitamin b2 religiously) I think the way my mouth is shaped is trapping saliva in the corner of my mouth and causing this. I would like your professional opinion on if this would help me.
A:Usually in refractory angular cheilitis the more definitive treatment is surgical excision of the involved mucosa and skin areas. While a corner of the mouth lift does change the downturned mouth corner it would not involve excision of the chronically infected tissues. While the downturned mouth corners may be the origin of the problem I don’t know if changing that now would beneficial/curative since the involved tissues are not what would be removed in the lift. But given the chronic nature of this problem the argument could be made that there is little to lose in trying.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am contacting you in regards to a webbed neck as you can see from the photographs. I have met with a surgeon local to our area and discussed options with him. His recommendations left us a little concerned. He kept mentioning doing a Z-Plasty, and we had already researched and found many examples on your website where you avoid Z-Plasty and scarring on the side of the neck by keeping all scarring on the posterior of the neck. He said he would do his best to hide the Z-Plasty behind the neck and claimed that the approaches you typically use may not work for me although he also noted that the webbing was not very tight.I would really like a second opinion from you.
A :In answer to your webbed neck questions:
1) I do not know what is meant by the Z-plasty location in terms of hiding it. Typically that means the Z-plasties are put along or at the lateral web lines in which there is no hiding it. But it may the Z-plasty is put on the back of the neck. If you really want to know what it means exactly have the surgeon draw it on your pictures of howe plans to do it…because he is going to have to draw it on for surgery. Just as good would be to see some actual intraoperative pictures of he does it. Then you will known for sure.
2) It is not clear to me how he would know that a posterior approach to the webbing would not work or why it would be a poor choice for your neck webs ….unless he has done the actual procedure. Is this a theory or is that opinion based on actual clinical experience.
3) The basic concept about neck web surgery is that, while improvement is possible, you have to be careful about trading off one aesthetic problem for another. If you make the assumption that the direct lateral Z-plasty approach produces better reduction of the neck webs than the posterior approach (I am not saying it does but for the sake of this discussion let’s assume that it does) the question then is it is better to have less neck webs but visible scarring OR less neck web improvement with no visible scarring. As that is fundamentally what the decision is between the two approaches.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I read your articles about the chin implants settling into the bone and that bone erosion is a myth.
The fear of a bone erosion is something that prevents me from having an implant.
I read this article in which patient 4 had 7mm “bone erosion”. So, I would to ask you, if that patient has the implant removed, will his chin be 7mm smaller?
A: What I have said is that implant imprinting into the bone is a normal biologic response and has no clinical significance. I have seen thousands of 3D CT scans of chin implants and have never seen imprinting more than 1 to 2mm into the bone. Not to memtion the hundreds of chin implants that I have actually removed and replaced. So I can not speak to the case in which the article refers.
But fears are not overcome by any form of logic. Thus have a sliding genioplasty instead and make that concern irrelevant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I am an American residing abroad. I have been looking for a clinic providing custom jawline and cheeks implants.. I saw a video on youtube where you performed such surgery. Because of the distance, I do not have the flexibility to fly in readily, so I would like to know the following:
Will it be possible to create the custom implants if i can get 3D scans done here and mailed to you?
Or, is it possible to get the scan and implants made, and surgery perform all in 1 trip? ( 2-3 weeks)
A: In answer to your custom facial implant questions:
1) I only design implants for patients in which I am going to surgically place them.
2) The custom facial implant process takes about 3 months to go through the design and manufacturing process to have them ready for surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in XL or XXL testicular implants. I’m confident that my testes are 3 cm or smaller. But, unlike your example in the article above, I do not have any redundant skin in my scrotum. Might you use osmotic tissue expanders to provide the additional skin in order to accommodate the implants?
A: There are two methods to expand/stretch out the scrotal skin. A tissue expander can be used and then replaced with a permanent implant later probably two months layer. (Dynamic tissue expansion) Or a larger permanent implant (5.0 or 5.5cms) can be placed and then 4 to 6 months later a 6.5/7.0/7.5 implant can be used to replace itplace. (Non-Dynamic Tissue Expansion)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello. I had a sliding genioplasty 1 year ago and I am so unhappy with the aesthetic result. The step offs are quite noticeable and it makes it seem that my chin doesn’t fit in at all with my face. Is there any way that the step offs puke be corrected at this point? I don’t want to have a revision surgery. Is there a way to correct it that would be less invasive? .
It just doesn’t look like my chin blends in. The nothings on the side really bother me. As well as the muscle pull that is occurring right below my lip.
A: With this many symptoms from your sliding genioplasty (visible stepoffs, excessive horizontal movement and muscle pull below the lip) there is no other method to improve all three without subtotal reversal.
The stepoffs can be treated in isolation by filling in the bone defects without recutting the bone but the other two symptoms wlll remain.
Dr. Barry Eppley
World-Renowned Plastic Surgeon