Your Questions
Your Questions
Q: Dr. Eppley, Just out of curiosity… I know that sometimes people will just have larger ones placed in front of the smaller testicles and I’m wondering how much that cost to do, or if that’s even an option with Dr. Eppley.
Also, is there an option where you can do the ones that wrap around the testicle but aren’t custom ordered? In other words are there pre-made versions of that particular style?
A:You are referring to the side by side or displacement testicle implant
technique.
There are no non-custom wrap around testicle implants.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hey there, I just have a question about the orbital rim implants, is there a screw involved in the procedure?
A: Yes, a titanium microscrew.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, How much does skull reshape surgery cost?
I want to make my flat crown area rounder.
Age 32,
Weight 165 pounds
Height 5’11
What is post surgery process and how fast can person recover and return back to work afterwards?
Does the hair grow back up?
A: As I understand your skull reshaping it is a crown of the skull augmentation which is down using a custom skull implant designed using the patient’s 3D CT scan. Recovery from such a skull implantation procedure is often quicker than one would think. Most of the recovery is about swelling and how mucgh time it takes to go away. (10 to 14 days) In regards to returning to work the critical question is what type of work are you returning to?
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Bonjour j’ai un crâne allonger depuis ma naissance. , j’ai 31 ans et j’aimerai savoir si ce handicap pouvais être soigner
A: You undoubtably have some form of congentall sagittal craniosynostosis to have siuch a long anteroposterior skull length. The question is whether the occiput (back of the head) could be reduced enough to make the surgical effort worth it. It would require a CT scan to determine the bone thickness to see how much reduction could be safely achieved.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, . After giving it more thought, I believe that the reason I dislike my shoulders is not because of the size but because of the shape of the clavicle joints. So a shoulder reduction would not address that.
I was wondering if Dr Eppley could take a look at the photos I’ve attached below and let me know if there is anything that could be done to reduce the clavicle joints (for example with shaving down). I know he has blog post in which he describes a surgery where scapular shaves were performed, so it would be more similar to that.
I am very interested in Dr Eppley’s response
A: What your concerns are is the amount of bone show that the distal clavicle and AC joint show. (see attached diagram and x-ray) While some of your distal clavicle and joint show could be reduced I don’t think enough of a reduction could be achieved that the result would justify the effort and scar. You can’t overly weaken the clavicle bone nor enter the joint space.
That being said as a general statement of AC joint clavicle show, your distal clavicle show is unique. While you have a lot overall clavicle show the distal clavicle actually bows upward and then goes back down into the AC joint. This distal bowing provides room for a safer clavicle bone reduction that would avoid entering the joint space. (see attached picture) Your side view picture shows it best of how prominent the distal clavicle is which does not even allow for the acromion process of the AC joint to show as it would in most people.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have to say I am very interested in the locking mechanism of your own design from a recent blog post. I can’t help but wonder if this could be utilized to facilitate slightly larger implants? As you have noted previously, due to the vertical placement of hip implants they are at risk for impact forces over time, folding, mal-rotation among others. Of course to mitigate some of that you can use higher durometer implants with the trade off being less of a feathered edge and likely more risk of implant show especially in thin patients. Perhaps if you created a locking mechanism for larger implants (see see pictures for my potential interpretation based off of your previous designs), you could use the iliac implant as a boney anchor that would support the implant, with less force directed to the inferior edge as a result. This might allow you to use a softer durometer implant with a more general and natural appearing feathered edge.
A: In comments to your inquiry:
1) Higher durometer implants can have very feathered edges. Implent edging is not affected by material durometer.
2) A major component of Implant show is a thin subcutaneous fat layer.
3) The locking mechanism for hip implants used with iliac crest plates can be used with any implant design or size. Its major benefit is that it would prevent implant bending at the bottom edge of the implant.
4) One developing idea for hip implants is to use a very small iliac crest plate fora superior bone anchor for hip implants.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’ll have braces to widen my smile arch and veneers to restore my teeth to it’s original condition. I also want my downturned mouth corners to be more straight, and lips a tad fuller, with an even oral fissure.
I know that braces can widen the mouth a little bit and make the lips a tad thicker due to the muscle stretching thanks to the wider dental arch (a nice effect for me), and must be done first.
My main concern is that I can’t find anything about what to do first after braces, if veneers before touching the lips, or the work on the lips first. All the information I’ve found is contradictory, with the surgeons saying “deal with the teeth first” and the dentists saying that they “follow the lip line” (which will be different after something like a corner lip lift or fat grafting) to design the smile. To add even more confusion, some cosmetic dentists say that veneers can make the lips a bit thicker if desired.
What should I get done first after braces: the veneers or the lips? I’ve attached you a picture of my lips next to someone who was similar lips to what I want to achieve, for reference.
A: Like building a house do the framework first and then worry about the exterior. Finish all dental work needed/desired and then see what the lips look like and go from there.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a question. Can u do “hunter eyes” ?
A: Yes,. Hunter eyes is defined as an elevated lower lis and corner with a more narrow eye aperture. In some men that may also mean a lower brow bone and decreased upper eyelid space.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
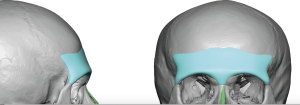
Q: Dr. Eppley, Hi, I’m wondering if plagiocephaly can be improved with skull reduction? I suffer from plagiocephaly, so my head is extremely crooked and the left side of my head sticks out a lot. I’ve been insulted and mocked on my head shape many times due to this. Skull implants are not an option for me as my skull is already huge and so a skull implant will only make it bigger, and it also won’t help the fact that my head sticks out so much on one side. So I’m really hoping a skull reduction will help. My head shape has ruined my life so I’m willing to undertake even the most risky of procedures in order to look normal. So I’m wondering if a skull reduction could indeed improve the look of my plagiocephaly?
A: How much the enlarged side of the head could be reduced depends on the thickness of the protruding bone. Only a CT scan can make the determination of the amount of bone reduction that is possible.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, What is the intraoral approach for reduction of the soft tissue chin pad effective?
A:The management of the excessive soft tissue chin pad with any form of chin reduction has always been an important consideration…which is not really a new concept. But I think for those surgeons who are focused only on an intraoral approach that is always going to pose a problem. But when the submental approach to horizontal bony chin reduction is done the excessive chin pad is removed as part of the procedure. I have done that approach for decades so I would not call it a new or revolutionary approach. It has always been the anatomically correct approach to many chin reduction patients
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, For webbed neck surgery:
1) what are the risks? – could there be muscle or nerve damage involved?
2) are the imaged photos below the best possible outcome or is there a chance I could see more significant results
A: In answer to your webbed neck surgery questions:
1) Muscle or nerve damage has never yet occurred in webbed neck surgery. So that risk is very low.
2) The purpose of the planning pictures is not to show patients the exact result they will get…as no one can accurately predict any surgical outcome. Rather the imaging is done to show patients what may be the LEAST amount of outcome that I think will happen. In other words if this is the best long-term outcome would the patient still choose to have the surgery? The trigger for surgery should not be hoping for the best outcome. Rather it should be what is the least outcome I can expect. Might the result end up better than the imaging….maybe. But what if it ends up just like the imaging…would you still undergo the surgery?
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, What is the largest testicle that a patient can receive?can receive? I currently pump and feels my scrotum is pretty stretched
A :Its more about what size that the scrotum can accommodate. The largest size testicle implant I have made and placed is 8.5cms. But there are numerous factors that influence testicle implant size from height and weight to how flaccid is the scrotal sac.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m looking for a correction for my impression of eyes spread that I’m not sure I have hypertelorism. I measured my interpupillary distance is 64mm, I don’t know, where it places me, I would like to have your advice on the question in terms of solutions to my problem.
A: The proper surgical solution is transcranial orbital box osteotomies …which is not a procedure I recommend for an adult.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My desire is firstly, to reduce my chubby cheeks. In the picture where I have the white strip behind my head Im anywhere from 12-15% body fat (middle distance track athlete), yet my cheeks are still chubby, and Im convinced that it is due to genetics as my fathers side tends to have rounder faces. I want my face to be slim so my facial structure, cheekbones, and jawline show. Secondly, I would also like to correct my receding/weak chin. Lastly, Id also like my face to appear forward projecting rather than narrow, with a stronger jawline.
A:’Fortunately’ you have a weak chin as the best soft tissue cheek reduction results come from concurrent treatment with chin augmentation, particularly that of a sliding genioplasty.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in a clavicle reduction. Am I a good candidate for the surgery? I measured my chest with a ruler and from edge to edge(between the two green lines I drew) I am 48 cm overall.
A:Technically anyone can have their shoulders reduced. What makes someone a good candidate is whether the surgery can achieve their aesthetic shoulder reduction goal. At 48cm bideltoid width with the ability of surgery to drop you down to ay least 44cms (see attached imaging) I would say you are a good candidate.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am considering a chin augmentation, and after some initial research, it appears that a vertical genioplasty may help me achieve the results I’m aiming for. I would greatly value your expert opinion on whether adding horizontal movement would also be beneficial in my case. If so, how many millimeters would you recommend for horizontal advancement, and would it make sense to simultaneously widen the chin to prevent it from appearing smaller in the frontal view?
My primary goals are to address an obtuse cervicomental angle and improve jawline definition. I am uncertain whether a combined vertical and horizontal genioplasty would best suit my needs or if additional procedures, such as liposuction or submentoplasty, might offer more comprehensive results.
For your reference, I’ve attached my profile and side profile images, along with front and side morphs.
Thank you very much for your time and insights on the best approach to achieve my aesthetic goals.A:As you have shown by your imaging what you are showing is a vertical chin lengthening to which I can say then following:
1) Your imaging shows no need for any horizontal chin advancement.
2) It is usually not a good idea to destabilize the chin (cut into two pieces to widen it) when it is undergoing any significant dimensional change. Your imaging also does not show any need for chin widening
3) Submental liposuction can only help to try achieve an obtuse cervicomental angle. A submentoplasty would be a more ideal procedure in that regard.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, About four years ago, while trying on glasses, I had my wife take a picture to see how I looked with a particular pair. For the first time, I noticed that one of my eyes was positioned slightly lower than the other. I’d never been aware of this asymmetry, and the discovery was quite shocking.
Since then, I’ve become increasingly sensitive to social interactions, noticing how often people avoid making eye contact with me. This has highlighted past experiences where I felt self-conscious but couldn’t pinpoint the reason. Realizing there was a noticeable asymmetry in my eye alignment has helped me understand some of those experiences. Unfortunately, this awareness has also impacted my self-confidence, causing me to avoid social settings and become more introverted.
I’m reaching out to discuss potential corrective procedures to address this vertical asymmetry. I’ve attached a photo showing that one eye sits slightly lower than the other. I’ve read about treatments like orbital floor implants and other corrective procedures and would like to know if options are available that could help restore my confidence.
Thank you for your time and consideration.
A:In assessing vertical orbital dystopia (VOD) the first thing I look is the amount of vertical discrepancy. In adults and non-craniofacial syndromic VOD (what I call aesthetic VOD) the key is whether camouflage techniques (e.g., custom orbital floor-rim-cheek implant, – a non-orbital box osteotomy approach) can be effective. This usually has to be a VOD that is 5mms or less in vertical discrepancy. That appears to be your case so it worth investigating potential VOD corrective surgery. The next step is to evaluate ‘internally’ the differences in shape and position of the orbital boxes. This requires a 3D CT scan which can be done in your geographic area and we place the order for it. That should be obtained before a virtual consultation so that time is more meaningful for treatment evaluation and planning.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’d like to address a pronounced “barrel chest” contour in my upper torso. My main goal is to create a more feminine, proportional appearance that will look natural once I begin hormone replacement therapy and breast development. Specifically, I’m hoping to reduce the forward protrusion of my ribcage so that my chest appears flatter and more contoured. This change would be an important step in my transition and would significantly improve my confidence and comfort in my body.
A: As you know there is not an established procedure for reshaping the barrel chest. It is certainly a ribcage problem that I have not yet treated. I have thought about it before but weas never certain what would be the correct approach. The article to which you have linked is the approach I would think would be effective (side rib length reduction with stabilization) but besides a lateral approach it is very unclear what they were doing exactly. They do not describe any rib length shortening and only discuss placing steel bars for modification…which I don’t see how that would work. And I also don’t see any details about the procedure or the patient’s upright postop photos which makes me suspicious.
That be said the lateral approach with rib shortening of #3 – #8 with plate fixation would seem the logical approach…..but like I said previously it is not a procedure that I have yet done so I can not vouch for how effective it would be.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
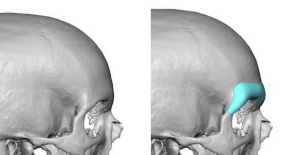
Q: Dr. Eppley, I had a TBI a few years ago. My doctor did covered it after medicaid approved it, but the company who made the implant didn’t do the scan of my head the right way so I still have small dent on my head.
A:If I understand your surgical history it appears that you had a custom skull implant for a craniotomy defect. This appears to have been in the left fronto-temporal area. I suspect the contour defect you are seeing is not the result of an ill-fitting or improperly made implant but due to the loss of the temporal muscle over it. This is very common in the temporal region as the muscle is stripped off to access the bone and, although it is sutured back up, it always atrophies and creates a soft tissue contour depression. You could prove that by a postop 3D CT scan.
So this is more of an issue of soft tissue augmentation than bone augmentation per se. Options include fat injections, ePTFE sheeting or a custom made implant overlay….each with their advantages and disadvantages.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in receiving a custom chin implant as well as a custom cheek implant for my right cheek (the side with the mole on it). I think the right side of my face is underdeveloped and the main cause of my facial asymmetry. I honestly think i have a mild form of hemifacial microsomia. I like the left side of my face and my goal would be to get the right side to look as similar to the left as possible. I also have asymmetrical lips and the right side lifts up higher than the left exposing more teeth when I talk and smile. Is there a solution to fix this? If you have any other ideas for procedures to correct my facial asymmetry I would be interested. Thank you
A:Like many facial asymmetries they are usually complete (involving the entire of the face) if you look close enough. (see attached grid analysis) These are aesthetic facial asymmetries as opposed to syndromic ones due to their more modest presentations. While all facial features on the side of the face are affected it is best to focus on the ones the patient has identified as most problematic as well as the ones that can be most effectively improved. Not all asymmetric facial features can be effectively improved.
You have identified the bony chin and cheek as your top two targets. The right lip asymmetry is not so effectively improved and as has the tradeoff of some potential scarring so that would be an asymmetric facial feature that I would leave alone.
Likie all facial asymmetries that have a bony component, and almost all do, the next step is the need for a 3D facial CT scan which will allow for more in depth assessment as well as is the platform on which the custom chin and cheek implants are made
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Concerning the result I want to receive from facial surgery, I would like to systematically explain my problem:
Before puberty I was looking like normal but at the age of 15-18 I experienced elongation of my face. So much that I cannot recognize myself anymore in the mirror. The “T” zone of my face became extremely elongated during those years. Making me so insecure about myself. I never understood what was the cause of my problem – why my face deformed so extremely?
The procedures I was considering for my condition were: Mandible jaw implants, cheekbone implants, maxilofacial sugery, rhinoplasty, lip lift, fat transfer under the eyes, or lower blepheroplasty.
I have very flat sides of the face. At first I wanted to do mandible jaw implants (that goes into width) – to widen my face. But then I was afraid it might make my face masculine, giving the fact that the T-zone of my face is extremely long. How is it possible to reduce the elongation of my face and make my face healthy and feminine looking? Also, I was thinking about fat-transfer to my under-eye and cheeks, but then I was afraid it might just make my face puffy and elongate the T-zone even more.
Ever since I was 16 I dreamed of some operation that would get my face back to normal. Is there any chance of converting my deformed face back to normal?
A: Thank you for your inquiry and sending your pictures to which I can say the following:
1) What has occurred in your face is normal development after puberty. It is not a true facial deformity per se. You simply liked your more pubescent face than what mature facial development has created. That does not negate that your do not like the facial proportions that have resulted. (long midface and shorter lower face)
2) You can not really shorten the middle third of the face as effectively as changing the lengths of the upper and lower face. That has always been and will always be a challenge. There are only a few limited changes that can be done that can help soften the length of the midface.
3) That being said one surgical approach is chin/jaw augmentation to increase the size of the lower face. As you have mentioned one must be careful in a female to not masculinize their face. The best way to make that determination is computer imaging to see what such a potential change would look like. Your reaction to that imaged change will determine if this is an acceptable or unacceptable change. (see attached imaging)
4) The aforementioned midface shortening procedure would be subnasal lip lift and a rhinoplasty that shorten the length of the nose.. I have put those changes on top of the jaw augmentation to show all procedures that may be helpful in improving your facial third proportions.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m reaching out to ask if your clinic offers custom brow ridge implants. I’m interested in enhancing the prominence of my brow ridge for a more defined and masculine look and would love to know more about the options available.
If you do provide this service, could you please share some details about the process, including costs and any consultation requirements?
Thank you very much for your help—I look forward to hearing from you.
 A: Custom facial implants, including custom brow bone implants, are procedures that I do regularly. The designs you see on the Custom Facial Implants site are from actual patient surgeries. To learn in greater detail about custom brow bone implants from design to placement please visit www.exploreplasticsurgery.com and place the term Custom Brow bone Implants in the search box and you will a large number of articles written in this topic from various patient surgeries.
A: Custom facial implants, including custom brow bone implants, are procedures that I do regularly. The designs you see on the Custom Facial Implants site are from actual patient surgeries. To learn in greater detail about custom brow bone implants from design to placement please visit www.exploreplasticsurgery.com and place the term Custom Brow bone Implants in the search box and you will a large number of articles written in this topic from various patient surgeries.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in a mouth widening surgery…altogether both sides ½ inch or so
(btw I don’t feel good with my nose). it should be half cm higher from tip to bridge
A:Mouth widening is usually done 5 to 7mms per side which would be consistent with the 1/2inch you have mentioned.
For the nose you are referring to increased tip rotation which is what shortens nasal length.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I was wondering how far can the nasal base or apex can be projected for a less flat profile. If you don’t mind. What’s the max on average could be projected by a midrange implant with focus of the nasal base. As you can see with this black and white illustration the nasal base or apex protrudes farther than the brown and chin. And with this model slightly as well.
 A:Typical nasal base projections in custom midface implant range from 3 to 8mms based on patient need.In custom implants you can create any implant dimensions so it really comes down to tissue tolerances in larger dimensional needs.
A:Typical nasal base projections in custom midface implant range from 3 to 8mms based on patient need.In custom implants you can create any implant dimensions so it really comes down to tissue tolerances in larger dimensional needs.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I was wondering if custom infra-malar implants would be the best procedure to improve my infraorbital rim hollowness/discoloration, zygomatic arch, cheekbone setness and overall lack of cheekbone mass.
-improving the overall mass and getting that “high set” look are paramount to me.
– is infraorbital discoloration due more to the lack of bone prominence in the area or could their be other reasons that are separate from the bone prominence itself?
A:To improve the number of midface issues that you have described custom infraorbital-malar implants would be the only effective way to do so. Undereye discoloration comes from two sources, shadowing and hyperpigmentation, often occurring concurrently. Custom IOM implants addresses shadowing but not hyperpigmentation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a problem with the small size of my head, and my head is also flat from the back.
A: The flat back of the head is very clear with widened biparietal-temporal areas. One can make no conclusions about head size based on just a 3D CT scan.
The flat back of the head is a straightforward implant augmentation approach. Addressing smaller head sies requires a multi stage approach.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
 Q: Dr. Eppley, I’ve been a fan of your work for a while. This is my first time contacting you and I was just hoping to get a few answers to some questions I had. If you could help with any of them, it would mean a great deal!
Q: Dr. Eppley, I’ve been a fan of your work for a while. This is my first time contacting you and I was just hoping to get a few answers to some questions I had. If you could help with any of them, it would mean a great deal!
Is there a difference between a supraorbital implant, a supraorbital rim implant and a brow bone implant?
I understand that every patient is different but how much is the average custom ct guided brow bone implant? (A range is completely okay to give).
How many millimeters does the implant in the attached picture add to brow bone projection? (Not sure if this is the right way to phrase it)
A :In answer to your brow bone implant questions:
1) The terms brow bone and supraorbital are interchangeable.
2) The attached brow bone implant design has 4mm centrally as seen in profile.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m considering jaw implants but have concerns about potential bone imprinting.
On your website, you mention:
“the average implant settling into the bone… was in the range of 1.5 mm…this is actually not just seen on the chin but can be seen in other facial implant sites as well (eg. jaw, cheek),”
but also state:
“I am not aware that there is any bony erosion with jaw implants. I have removed many from surgeons over the years and have never seen that issue.”
Could you clarify if bone imprinting occurs with jaw implants, and if so, by approximately how many millimeters? Should this be considered in the design—for example, if I need 5 mm of width, would it be better to choose 6 mm to account for potential bone imprinting?
Thank you.
A: Every facial implant gets some degree of bony imprinting, manifest more prominently at the chin and jaw angles. I don’t consider it to have any clinical relevance and you don’t create implant dimensions or pick implant sie based on its potential occurrence.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I realize it depends on individual cases, but generally speaking, would you consider a 3mm orbital decompression to be conservative?
A:For the eye area a 3mm change is likely ‘significant’.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I actually don’t hate my resting face, but when I smile I feel like my chin and maybe even jaws just look terrible.
A:The general concept here is that this is a dynamic facial problem….meaning at rest the face is fine but the problem only appears in dynamic facial motion. (e.g.,smiling) It is also important to remember that surgery is a static action not a dynamic one. In other words surgery is done on a resting face not a moving one.
That being said what I see is a bit of a vertically short chin, which at rest is very acceptable, but when smiling the soft chin pad is pulled down over it creating a dynamic chin pad ptosis. The only way to treat it would be vertical chin lengthening to prevent that dynamic chin pad ptosis. This will change the appearance of the chin at rest, making it a bit longer so one has to be certain that static facial change is acceptable. (see attached imaging)
Dr. Barry Eppley
World-Renowned Plastic Surgeon