Your Questions
Your Questions
Q: Dr. Eppley, I’m interested in 5mm mouth width expansion per side, I was wondering how long it would take for “normal” scarring that usually happens as a trade-off to look acceptable enough to not have it be easily noticeable by other people or distract from the result.
A: Corner of mouth scars generally take 3 to 4 months to mature particularly in intermediate skin pigments.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in revision options for my custom jawline implant. During my last discussion with Dr. Eppley, he mentioned several options beyond a full revision. One option involved adding additional components to the existing implant to enhance projection and angles. He also suggested a soft tissue graft to address and cover the bulging near the masseter muscles.
Could you please provide more details about this approach? Specifically:
• Would the current implant need to be removed to incorporate the new components, or can they be added without removal?
• How are the additional parts secured—are surgical screws or adhesive methods used?
A:‘During my last discussion with Dr. Eppley, he mentioned several options beyond a full revision’
FYI it would be a full implant replacement….not a revision. A revision is when you are taking what you have and try to modify it. Plus a revision relates to the primary surgeon wo did the original work. When a new surgeon assumes that initial work it is a secondary procedure not a revision. While a bit semantical there are very different implication between the two.
‘One option involved adding additional components to the existing implant to enhance projection and angles’
 You are referring to Transcutaneous Soft Tissue Jaw Angle Implants. A common technique that I employ to treat masseteric muscle dehiscence with implant reveal. It is the only technique that works if one desires to keep their current jaw angle implant shape. The alternative is to change the implant with a new design that doesn’t have such a square jaw angle shape…which is what caused the problem in the first place.
You are referring to Transcutaneous Soft Tissue Jaw Angle Implants. A common technique that I employ to treat masseteric muscle dehiscence with implant reveal. It is the only technique that works if one desires to keep their current jaw angle implant shape. The alternative is to change the implant with a new design that doesn’t have such a square jaw angle shape…which is what caused the problem in the first place.
Soft tissue jaw angle implants are placed in the soft tissues overlying the current implants, they are not bone implants. (see attached picture)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in Lefort 1 osteotomy surgery. The reason I want to have this surgery is that the maxilla, the middle part of my face, is long and I want to make it look shorter. My face, which is between the eyes and the lips. how much of a change there could be?
A: You are under a common misconception that if you shorten the maxillary bone (LeFort I impaction) your external midface appearance will get shorter…which it will not. The LeFort I impaction is for the treatment of the excessive gummy smile patient to achieve less tooth and gum show. It can not shorten the appearance of the midface as where does all the soft tissue go if the bone is shortened? It doesn’t go anywhere…it will remain the same.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, What is the recovery time for temporal muscle reduction? I suffer from migraines a lot, would Botox injections help shrink the temporal muscle?
A: It takes a good 2 to 3 weeks for the swelling to resolve. But there are no physical restrictions during the recovery.
My assumption in your questions is that you may be seeking temporal reductions for migraines?? If that is the case the important question is where is the location of the migraine pain in the temporal area? Knowing that information will determine whether surgical reduction or Botox is the appropriate treatment.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in aesthetic skull reshaping surgery & the costs involved. I’ve attached a few photos to see of the desired “after” results are possible and what costs would be involved.
A: Based on your own imaging it appears that you have done a modest left forehead-parasagittal augmentation. This would be very achievable as with a 3D Ct scan one could see the difference between the two sides and from that difference a small custom skull implant can be designed/made to provide a symmetry-achieving effect.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hi Im very interested in ZSO on my right cheekbone to expand and match my left.
A: The main concept to grasp is that when one side of the cheek is asymmetric (smaller ot bigger) it is a three-dimensional problem not a two dimensional one. The cheek is a solitary projection from the side of the midface so there is more than just a width deficiency when it appears amaller. The zygomatic sandwich osteotomy (ZSO) creates a two dimensional effect not a 3D one. This will likely become glaringly apparent when the ZSO operation is performed. This is why a 3D cuystoim cheek implant produces a better aesthetic result from all facial angles.
But even if a ZSO is to be performed the critical question is how much expansion is needed to optimie cheek symmetry. This is where a 3D CT scan of the face is needed to determine not only how much width addition is needed but how significant the 3D bone differences are
Dr. Barry Eppley
World Renowned Plastic Surgeon
\
Q: Dr. Eppley, I am interested in changing the shape of my head. Attached below are two pictures of me and 3 picture that I can find to best describe what I want. Hope this helps.
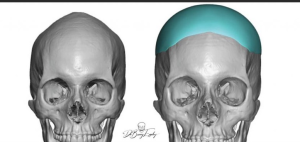
 A: Based on the pictures you have sent you appear to have an inverted V shaped top of the head with narrow sides. (parasagittal and temporal deficiencies) The two skull implant shapes you have shown are designed to address those goals and can be placed during a single surgery.
A: Based on the pictures you have sent you appear to have an inverted V shaped top of the head with narrow sides. (parasagittal and temporal deficiencies) The two skull implant shapes you have shown are designed to address those goals and can be placed during a single surgery.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hi!! I just heard that dr barry eppley had done inferior orbital box osteotomy, which is less riskier than 360 degree OBO. Actually i just wanna reduce my IPD as a woman. Can this technique reduce my IPD by upto 5 mm. Also can Dr. Eppley perform it?
A:Inferior box osteotomies can be effective for modest IPD increases but not for IPD decreases.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I was looking at some videos on youtube of Dr. Eppley performing this procedure and I was wondering if the implant that is slid under the skin on the scalp could cause some kind of damage to hair follicles?
Also once the surgery is performed could the implant move? If the back of the head was to be hit or hit some sort of surface could the implant be displaced under the skin?
Would wearing a motorcylce helmet also potentially cause this? Or other complications?
A: 1) The implant is placed on the bone under all five layers of the scalp way under the location ofmthe hair follicles. As long as the patient doesn’t insist on having an implant that is too bog there is no excessive stress on the hair follicles. (shock loss)
2) Because of their large surface area coverage and the tightness of the overlying scalp skull implants can never move or change position.
3) Skull implants are impossible to fracture or be damaged. As a result ther are very much like putting a bumper on the skull….providing inadvertent protection to the skull from any future trauma.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I wanted to do plastic surgery on my forehead.
A: I believe you are referring to the bony prominences of upper forehead known as large forehead horns which is a form of frontal bossing. How successfully they can be reduced depends on the thickness of the upper forehead bone which requires a CT scan to determine. (how much the bone can be safely reduced)
Dr. Barry Eppley
World Renowned Plastic Surgeon
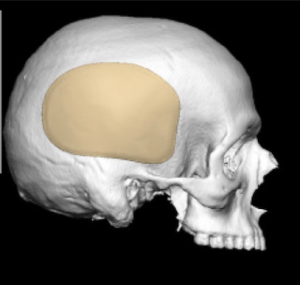
Q: Dr. Eppley, I am interested in Skull Reshaping. Although I am a petite person, I feel that my head is too small head and would like to add some height and volume to the crown of my head. What is involved in this surgery and how safe is it?
A: You are referring to classic female crown of the head augmentation nusing custiom skull implants which I do regularly. There is no question about safety of the surgery. The more pertinent question is whether your desired result requires a one or two stage skull augmentation approach. (the latter is what most females need to achieve their desired result)
I would need to see some head pictures for an assessment and imaging to help make that determination.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, isis any type of procedure that can shorten the midface area? I am assuming no because I already had double jaw surgery 8 years ago and cannot have any further orbital surgeries due to my surgical history.
Is a custom supraorbital/infraorbital implant something that may improve the eye area appearance compared to my current fillers and implant
The main thing I am unhappy with is how my eyes look when looking downward – the hollowness and sunken space above my eyes – maybe a better supraorbital implant would help
In regards to the rest of the face – shortening my midface and maybe a slightly wider and longer jaw
If the midface cannot be shortened I am assuming that lengthening the jaw a little bit will make it look more proportional.
A:You have correctly surmised that you can’t vertically shorten the midface. What can her done is to vertically lengthen the lower third and mildly augment horizontally the middle third as in the attached imaging.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I contacted a couple of months ago about clavicle reduction surgery as a trans woman 28 with large shoulders at the beginning of transitioning. I was hoping to get a consultation to discuss this further and if you have done any manipulation or reduction of the scapula as my shoulders are so broad and it’s one of the biggest parts of distress to me and really really need help with this. I’m not fully committed yet, but I still would like to pay for a virtual consultation as I really would like to discuss my concerns.
A:While scapular spine reduction can be concurrently done in shoulder reduction surgery for its prominence you are probably referring to the width of the scapula for which there is no satisfactory reduction technique.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Would temporal artery ligations be covered by insurance?
A:That is a question to which the answer I would not know. But I would highly suspect unless their were medical symptoms associated with it (e.g., autoimmune, visual impairment) that it would be viewed as a cosmetic issue.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have attached pictures of my penius both erect and flaccid. I suppose this sort of surgery is always for aesthetic reasons, but I feel the need to justify anyway. :-)In the flaccid picture I just feel that the scrotum is smaller than it “should” be proportionally. I realize this is because I have an above average flaccid length that varies but with the suprapubic area retracted (as I am hoping it will be post lipectomy) the flaccid length is in the neighborhood of 6 or 7 inches. The skin tightening will draw the scrotum up more and I would prefer the scrotum to hang down at or even past the length of it flaccid. That just seems like the traditional shape in my head.
The “problem” is exacerbated when I become erect as I believe they become very much dwarfed by the rest of my shaft both in girth and length. If I am not explaining myself well, please feel free to ask questions if it will get more useful information.
The last picture is sort of a goal picture. It is of me a day or some after having infused about 750ml of 0.9% Sterile Saline IV Fluid. (I take every precaution imaginable.)
A:This is classic aesthetic penile-scrotal disproportion. When it comes to testicle implant size selection using a side by side or displacement technique here are the concepts to know:
1) It is not an exact science. Until one is in surgery there is no way to know what will ‘fit’ or what the maximum implant size the scrotum can handle. There are no preoperative measurements/tests that will answer that question.
2) But since every testicle implant over 5cms in size must be made custom we do have to pock a size since it is one custom design per patiebnt.
3) A good rule to follow is that for adequate displacement of your natural testicles the implant should be at least 70% that of your natural testicle size. (100% is even better)
4) If any custom testicle size that is chosen does not fit in surgery I can manually reduce them so that they will. (would like to obviously avoid)
5) ) Many custom testicle implant size selections are a battle between myself (who is worried about having them fit and the creation of potential problems ) and the patient who wants the maximum size possible. (who is understandably only focused on the their benefits)
6) Your goal picture sh0w very low hanging testicle, which may or may not occur from large testicle implants, but most certainly will not in the early after surgery phase. That requires time and scrotal skin relaxation….and may well require ‘ball stretching’ postop as well.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I wanted to inquire about what I could realistically achieve when I commit to a full jawline implant and 2 cheek implants. I would like to restore what I had but wanted to see if it was possible without adding much vertical length. I feel that on the side that I liked the most they mostly took the jaw angle and the thickness of the bone. I wanted to attach pictures to have you run by Dr. Eppley to see if this is achievable. Additionally would it be better to have my zygoma knocked back to the original position and have standard cheek implants put in or will custom be better for adding width and projection back to my cheekbones instead of just forward projection. I am attaching the photos below. These are all before my jaw surgery in Korea. The first is what I had before and the second is the width from the side I liked.
Thanks for all your help!
A:In looking at your panorex xrays before and afters, which provide the best information we have as to what was actually removed in your V line surgery (3D CT scans are best), it can be seen that it was really in the jaw angle area where most of the bones was removed vertically. (the chin was spared) When reducing jaw angle length that also reduces jaw angle width. I see no bony reductive changes anterior to the jaw angles. Thus if the goal is jaw restoration, but without adding any vertical length, then it would be just adding back some width only to the jaw angles. Whether that amount of width reduction is worth a custom implant approach can certainly be debated.
For the cheeks you can’t just cut the bone and push it back out. Such cheekbone reduction osteotomies are a one way street so to speak. Cheek restoration requires an implant overlay. The debate there is whether standard or custom implants can do so better or more effectively.
While it is always hard to argue that custom implants are always better for any form of facial bone restoration that always depends on how much bone augmentation is needed, whether any significant asymmetry exists and what the patient prefers.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had double-jaw surgery some time ago to correct my short face syndrome. The swelling is almost all gone. While there has definitely been some improvement in the length of my face, I still feel that my chin is too short and I think I could benefit from another 4-6 mm of vertical height. But if you refer to the picture I shared, I think the way the surgeon has done the genio cut makes it difficult to get another vertical genioplasty. Am I correct?
A:You are correct in that with that genioplasty design it would be very precarious to try and do a secondary vertical lengthening genioplasty…not to mention the bony stepoffs would become much greater and noticeable with that osteotomy design. To achieve another 5mms of vertical chin lengthening you would be better served inferior implant augmentation, particularly a custom implant desitn to add length, smooth over the bony stepoffs and blend into the jawline behind the chin with smooth inferior border contour.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi there, I contacted a couple of months ago about clavicle reduction surgery as a trans woman 28 with large shoulders at the beginning of transitioning. I was hoping to get a consultation to discuss this further and if you have done any manipulation or reduction of the scapula as my shoulders are so broad and it’s one of the biggest parts of distress to me and really really need help with this.
A:While scapular spine reduction can be concurrently done in shoulder reduction surgery for its prominence you are probably referring to the width of the scapula for which there is no satisfactory reduction technique.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I currently have custom 3D PEKK jaw angle implants in place which was done in Houston. I would like the current implants removed, and replaced with a different custom made jaw implant. I was looking into double jaw surgery to fix slight jaw canting and my midline, but most surgeons agree that my case is not severe enough to warrant such an invasive surgery. Instead, I would like to have a different design of implants that is more modest, smaller in shape and thickness, and fit more into the Korean aesthetic. My main concerns is symmetry and balance, while also providing more jawline definition rather than the “roundedness” that I currently have.
A:According to the attached design file those jaw implants are fairly large and have a very square angle shape to them. I can certainly see how one can perceive them as too big. (although I have not seen any before and after pictures of the change) But the only aesthetic judgment that matter is yours so if you think they are too big then they are. Certainly smaller jaw implants can be made and placed and the size issue addressed. What I do not see as happening is improved jawline definition when implants are down sized. Definition comes from stretching out the overlying soft tissues creating better show of the implant/bone underneath. (in other words increasing the hard to soft tissue ratio) When decreasing an implant’s size that ratio reverses a bit and more soft tissue ‘appears’, thus decreasing the favorable definition ratio.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, What about a mini facelift to accompany a custom jawline implant? To address the jowls and get rid of the nasolabial folds?
A:Any form of a facelift will get rid of the jowls along with the jawline implant but it can never really improve nasolabial folds. No one has been able to solve that central aging facial problem in an adequate way with facelift surgery for over 100 years.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I was just looking at your amazing work as regards to chin wing !I’m a middle age guyand I would like to know more please, recovery times, awaiting list? & cost please.I have just finished Invisalign retainers so my teeth are good! I would ideally like a more stronger jaw line ? & wider jaw /chin ??
A:Bone procedures like the sliding genioplasty and chin wing only make sagittal projection changes, they can not make any chin or jaw width increases. If one wants chin or total jaw augmentation in which width is added this requires a custom jawline implant approach.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I want the top of the head to look not peaked. I guess I need implants. I want it to be straight.
A:Based on your pictures you don’t have a true peaked or sagittal ridge head shape. It is a parasagittal deficiency for which implants would be the correct treatment approach.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I ended up getting bi-max… could there possibly be any room, room whatsoever, for a custom VLC implant”. The geniplasty fixed my lip incompetence but created a MASSIVE step-off.
A:There is always room in my experience to add an implant along the inferior border of the jawline in cases of sagittal split and sliding genioplasty stepoffs
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, my goal to widen my face and look more masculine. Currently, my bigonial/bizygomatic/bitemporal width all fall into the ideal range, but that’s only because the 3 are narrow. Therefore, would getting infraorbital-malars + jaw implants be enough, or would I need a total skull augmentation with skull implants for the effect to work? My worry is that without skull implants. I could get a big step-off while widening the zygomatic arch, or it’s just not possible to achieve such an effect without them. Thanks
A: The way to answer that question is computer imaging using our own pictures to look at these potential facial changes, individually as well as collectively. You need to take the theory and put it into reality.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, My maxilla has no forward growth and my cheekbones are not prominent at all
I have quite wide zygomatic bones, and quite low cheekbones if im correct but I dont want to widen my face anymore, I want more hollow set cheekbones that look higher similar to the model like Francesco lachowski, im the 18 years old so my face is stopped growing.
You can see these cheekbones are the desired effect,
But I dont know if this is possible with malar implants becuse my maxilla is quite recessed maybe it would make my face look more wider?
A: The short answer is that you can’t have more prominent cheekbones without making them wider.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Well i think i have plagiocephaly as i have my left side of the skull bigger, eyes and ears at different height and an irregular jawline. I also noticed as you can see in the x ray , my higher face (eyes and nose area) is moved all to the right wich contributes to my asymmetry. My question is if , even though i’m an adult, the plagiocephaly can be almost fully corrected and if my midface (eyes and nose root) can be repositioned to be more central and while doing so also making my face a bit narrower (I think my condilar bones get too wide at their joint), giving it a more masculine look.
A: As stated previously any further discussion about what changes are possibloe begins with a 3D CT scan as well as a full picture assessment. I would be cautious about using the term ‘full correction’ in plagiocephaly. as some asymmetry issues are correctable while others are not.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I read your recent article on iliac crest reduction in October 2024 and i was blown away by the results! I have been battling with gender dysphoria because of the width of my pelvis for awhile but could not find any before and after photos online, nor examples of surgical scaring thereafter. I really appreciate Dr. Eppley’s detailed explanation on the surgery. I feel more confident that this is a surgery i want to undergo now. However could I request information on down time after surgery
A: The recovery from iliac crest reduction is related mainly to discomfort with walking which tskes about 2 weeks to go away and return to normal.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Previous implant in chin and very unsatisfied with it with previous Dr. My 3D T scan shows a tilted chin implant with long wings.
A: This is a classic aesthetic issue with most commonly used chin implant styles in females….they make the chin wider because they all have wings.(aka extended anatomic style) These are really male chin implants because males can tolerate and often want a wider chin…most femake do not. This is the result of only considering preop the side view and not the frontal view ot the patient’s gender.
What you need is a specific V-shaped chin implant of same horizontal projection but without wings. In other words an implant shape that is more compatible for a female face.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve been thinking about getting the mouth widening procedure for a while because I’ve always felt like my mouth width is too small but I decided against it earlier due to the risk of scarring being bad and needing a scar revision.
However, after my genioplasty, my mouth seems even smaller to me now and I’m strongly interested in getting mouth widening done.
If I were interested in achieving the width of my mouth to be approximately equal to vertical lines dropped down from the inner edge of the iris of the eyes, I was wondering if that would be achievable and what the risk of adverse scarring would be. I was also wondering if it’s possible to make a morph for this as I’d greatly appreciate it.
A: While your mouth width did not really get smaller after the sliding genioplasty it may appear that way now because the chin size is bigger…so the lips/mouth to chin ratio has changed. As the swelling fully goes down that may tip back to a more favorable ratio/proportion.
That being said it appears it would be at least 7mms per side…where the risk of adverse scarring in increased with your skin pigmentation.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I dislike the vertical length of my lower face. I am interested in a consultation for a custom jawline implant can adequately vertically lengthen the entire bone along the inferior border from angle to angle. Dropping down the entire jawline 5mm to 7mms with some small horizontal lengthening if required.
A: I believe this is the type of jawline change you are seeking of which you have correctly surmised can only be accomplished by a custom jawline implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon