Your Questions
Your Questions
Q: Dr. Eppley, I was inquiring to see if masseter muscle reduction surgery is something you can do? So rather than a jaw reduction of the bone, just reduce the muscle in the jaw. I’d be coming in from Arizona for surgery so approximately how much would something like that cost me? And what would the recovery time be? Thank you.
A: Masseter reduction surgery can be done but it does slightly different than one would think. You do not go in and cut a portion of the muscle out as that would be very bloody and would likely leave the outer facial contour irregular when it heals. Rather the muscle is lift off the bone from the inside of the mouth and its inner surface treated by electrocautery. This will cause some muscle fibers to die and a portion of the muscle to atrophy obver time. Also Botox is injected into the muscle at the same time to help the atrophy process. I assume you are aware that you can treat masseter muscle hypertrophy with repeated Botox injections to help it shrink without surgery.
Other than some swelling there really is not much recovery or limitations after surgery. The jaw will feel stiff for a few weeks from the muscle treatment.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a mild chin cleft that I would like corrected. I have attached a picture so you can have a better understanding. It drives me nuts when I smile as it is so visible particularly in pictures.
A: By your picture what you have is a chin dimple not a chin cleft. That may seem like a semantic difference but anatomically there are somewhat different entities and are treated a little differently. A chin dimple that presents itself when you animate (smile) represents a defect in the mentalis muscle that covers the chin. Lacking fat underneath it and a defect in the muscle, the skin is pulled inward acting like an adhesion to the underlying tissues. Conceptually, volume needs to be added under to dimple to push it outward. This can be done by a number of ways but the simplest method is to place some injectable fillers (e.g., Juvederm) underneath the chin dimple. While this simple office treatment will not be permanent it will last 6 to 9 months and will answer the question whether the ultimate placement of fat injections would be the best long-term treatment of your chin dimple correction.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am very interested in your custom one-piece wrap-around jawline implant but have a few questions.
1. I saw an example of your custom wrap-around implant in an article you published on August 24, 2014 on your website. It was very impressive and exactly what I’m looking for. How difficult is that procedure compared to the standard 3-piece chin/mandible implant?
2. Is the recovery time and swelling reduced in the one-piece wrap-around implant compared to the 3-piece (because it is inserted only under the chin and not inside the mouth as in the 3-piece)?
3. Is the incision under the chin larger in a wrap-around implant compared to just a standard chin implant incision?
4. Apart from cost, what disadvantages do custom wrap-around implants have against an off the shelf 3-piece? (In other words, if cost wasn’t a factor, why would I or anyone ever consider a 3-piece implant?
 A: In answer to your questions about a custom wrap around jawline implant:
A: In answer to your questions about a custom wrap around jawline implant:
- If your questions about difficult relates to its surgical placement, it is not more difficult than placing standard chin and jaw angle implants…if one had done it a fair number of times.
- Usually three incisions are still used for a custom wrap around jawline implant because it is critically important to check and ensure that the posterior jaw angle portions are properly positioned on the bone. But the overall swelling and recovery are no different than placing three separate chin and jaw angle implants.
- The incision under the chin is the same for either standard chin implants or a custom jawline implant.
- Good question! They are so superior that cost would be the only reason not to use them…and when the costs are considered for either a standard or custom jawline implant approach the custom implant is not significantly more costly.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 32 year old male. I have a very flat brow bone and have been looking at getting something done as I believe it detracts from my overall appearance. My biggest concern has always been about the severity of the surgery to do something about it. It seems to me that you have multiple solutions which offer a more minimally invasive procedure. My question is about the cost of Endoscopic Placement of Custom Brow Bone Implants and the lifetime of those implants. Do they need to be replaced? And what are the complications with the procedure. If you could please let me know that would be greatly appreciated. Thank you.
A: Custom brow bone implants, like all custom facial implants, are made of a solid silicone elastomer material. They are permanent implants, will never degrade or breakdown and will never have to be replaced. They are placed through an endoscopic technique using two small incision either in the scalp or at the edge of the hairline. While there are potential complications with any facial implant procedure (e.g., infection, malposition), I have yet to see any with that of the brow bone. The one huge advantage to a custom approach is that the implants will have a precision fit and the their size and shape will have been designed in advance to the aesthetic desires of the patient.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a consult scheduled with you in the next few weeks for a breast lift and removal/replacement implants. I was also wondering if you could answer some questions about the differences between Exilis, Vanquish, Venus Freeze, Cool Sculpting and I-lipo. A friend of mine has tried the I-lipo. I have read about all of them online. Hard to tell what the “best” option for a little targeted fat loss and skin tightening would be. Maybe they are all good options.
 A: In today’s world of non-invasive/non-surgical body contouring, there are a number of devices that are currently available for some degree of fat loss and a little bit of skin tightening. (and I want to emphasize the phrase ‘a little’) All available devices are based on some form of penetrating energy from ultrasound, infrared, radiofrequency and thermal sources. They all claim effectiveness but whether one is better than the other can never be proven since there are no comparative clinical studies of them. I have used most of these devices and, in the properly selected patient, can offer some reasonable results. Currently we use Vanquish and Exilis for the best non-invadive body contouring results, They are best used in those patients who are never going to have surgery to those that want to give it a try with actual surgery as a final treatment if needed.
A: In today’s world of non-invasive/non-surgical body contouring, there are a number of devices that are currently available for some degree of fat loss and a little bit of skin tightening. (and I want to emphasize the phrase ‘a little’) All available devices are based on some form of penetrating energy from ultrasound, infrared, radiofrequency and thermal sources. They all claim effectiveness but whether one is better than the other can never be proven since there are no comparative clinical studies of them. I have used most of these devices and, in the properly selected patient, can offer some reasonable results. Currently we use Vanquish and Exilis for the best non-invadive body contouring results, They are best used in those patients who are never going to have surgery to those that want to give it a try with actual surgery as a final treatment if needed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am unhappy with my nose and I have been considering rhinoplasty for a while as well as jaw augmentation. For my nose, my first main concern is that I don’t like the bulbous tip it has. I’d like the tip to look pointier and to project a bit more. Second, I think my nose is too wide. I would like my nostrils to be narrower from the front view. I have attached a few photos of my face, as well as a couple models whose noses I like.
For the jaw, I have been considering some combination of chin and especially jaw angle implants. Perhaps even sliding genioplasty, the latter I understand is the only way to add vertical chin height. I basically want to create a stronger looking profile that balances my face.
I also have a few secondary procedures I am considering but not sure about. A reduction of my lower lip reduction (I think it is too big compared to the upper, and might make my chin appear larger if it were reduced). And also forehead augmentation (to reduce the appearance of my sloping forehead/prominent brow bone)
I am trying to figure out which procedure/s would produce be the best result in my case.Would it even be possible to do all of them at once?
A: Briefly, all the facial procedures you have discussed can be done as the same time and it would not be rare in my experience to do so. But first we must go through each procedure and determine what is the best approach for each change and how much change you desire for each area. Options in rhinoplasty and jawline enhancement are best done through initial computer imaging. I will do some computer imaging using your pictures of these changes and this will be a good starting point for our treatment planning discussion.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, the right side of my face looks bigger and more elevated than the other side, and the position of my right eye socket is higher than that of my left one. My jaw is also asymmetrical. When I bite, I can feel that the left side of my upper jaw and lower jaw is higher than the right side. I can also feel that the bone between my right eye socket and.my upper jaw is bigger than that on the left side when I touch. Is it possible to make my right side identical to the other side? If so, could you advise me on what procedures I should take and their costs? Thank you.
A: For your facial asymmetry correction, there are some structures that can and can not be changed. It is not possible to lower a higher eye socket. (orbital box) A lower eye can be raised somewhat but a higher eye can be lowered. Your maxillomandibular cant (jaw asymmetry) can be corrected by a LeFort I osteotomy to shorten the longer side. (vertical maxillary reduction) To keep your current occlusion (bite) a sagittal split ramus osteotomy is needed to rotate the lower jaw back into occlusion as well as complete the vertical shortening of the right lower face.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in getting a chin implant but had radiation for a sarcoma on my chin as a teenager which was over thirty years ago. I have read that you like to inject fat prior to placing an implant in an area that has previously received radiation. But doesn’t the fat just go away?
A: The purpose of the fat injections is not to create the augmentation effect, although it may have some mild benefit in that regard. Their purpose is to improve the blood supply and healing potential of your chin to eventually withstand the effects of placement of a chin implant. Fat injections are well known to help reverse the effects of irradiated damaged tissues through a process known as neovascularization. The fat may indeed partially or completely resorb but it will have improved the blood supply of the tissues through various stem cell and growth factor effects. With your history of facial radiation treatments with the chin as the direct recipient of them, placing a chin implant into these damaged tissues could be fraught with wound healing and infectious problems afterward. At the least, fat injections will help soften the chin tissues in preparation for the stretch effects of what an underlying chin implant will create.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m currently in the midst of orthodontic treatment and I’m scheduled for some surgical palatal expansion and double jaw surgery later on (Lefort I). I have recessed maxilla and mandible bones, so they will both be advanced (after my palatal expansion is complete).
I also have a midface deficiency. I have a tear trough deformity and scleral show. I believe that a LeFort III would work for me, but I have to be realistic because it’s very invasive. I don’t suppose I’ll be able to find a surgeon to perform such an invasive operation on me – which is why I would like to ask if a malar osteotomy and some kind of orbital rim procedure after my jaw surgery would produce the same results as a Lefort III – filling out my midface, making my cheekbones more prominent, and correcting scleral show. Do you offer those procedures?
A: There is no question that a simpler and more effective treatment to your upper midface concerns is NOT a LeFort III but custom orbito-malar facial implants. They would provide a much better result than trying to move the bone and are made from a 3D CT scan and could be done after your orthognathic surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am inquiring about abdominal implants to create a 6 or 8 pack look to the abdomen. I think they called are ‘blocks’ and up to 8 implants would be needed. Can you tell me anything about this procedure?
A: In the fast track way to six-pack abs, abdominal implants are different than abdominal etching by linear liposuction. While linear liposuction looks to make the six-pack look by accentuating the muscular inscriptions through fat reduction under the skin along their lines, implants do exactly the opposite. They are placed between the inscriptions under the fascia like a muscle implant to accentuate the bulging between the inscriptions. Thus they are like ‘blocks’ so to speak. Other body implants, like buttock or pectoral implants, are carved down to make the soft supple implant shapes that go between the inscriptions under the abdominal fascia. There are not true abdominal implants, just other body implants that are modified. But shaping the implants is not real the hardest part, it is the placement of them that is the challenge. If one was having an open tummy tuck, then their placement would be easy and this is why it is frequently recommended to do them at that time. But the vast majority of patients that want six-pack abs don’t need a tummy tuck. Thus they must be placed through a belly button incision and with this limited access it can be a 2 to 3 hour surgery to do so.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a chin implant revision. I wrote to you awhile back about getting a button style chin implant after a chin reduction by sliding genioplasty. My chin was reduced about 4mm. I then got a 3mm button chin implant placed, hoping to reverse the outcome of the chin reduction. Thankfully I’ve had no complications but I know have the look of slight jowls of both sides of the implant, especially on the left side. I’ve tried fillers but I really can’t afford to get fillers placed every year. Have you ever placed an extended anatomical implant with wings that measure 1mm in thickness? Have you ever placed an extended anatomical that has one wing thicker than the other to fix asymmetry? Thanks for your time.
A: Most chin implant wings, if they are made of silicone, are very thin often being only 1 to 2mms in thickness as they taper back along the jawline. The chin implant wings can be adjusted in length and thickness to compensate for asymmetry between the two sides. That is not an uncommon modification done in some chin augmentation patients whether it is a primary surgery or a chin implant revision.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I recently posted a question on Real Self regarding my cupid’s bow and if/how it could be changed in shape. (upper lip reshaping) I got a response from you and was wondering if you could possibly explain it further. You said you can change the distance between the height of the cupid’s bow slightly through small skin excisions on each side of the existing cupid’s bow. Forgive my ignorance here but does this mean that the height between the cupid’s bow can be lowered? I was also wondering if a dermal filler on the outer portion of the upper lip would even out my lips and make the cupid’s bow less prominent. Thanks in advance for your response.
A: My remembrance of your question was that the height or peaks of the cupid’s bow was too vertically high. By removing the peak of the cupid’s bow through small vermilion excisions, their height could be reduced by a few millimeters. That would smooth out the cupid’s bow to some degree. The trade-off is that there would be a very tiny scar between the vermilion and the skin. You could also go in the opposite direction and lift up the sides of the vermilion outside of the cupid’s bow to reduce their appearance. (lateral vermilion advancements) Injectable fillers may help in that regard but do not have the same vermilion lifting capabilities and would have to be repeated. But it is certainly a non-surgical lip reshaping test of that approach and there is no harm in doing so.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, It was good to meet you today to discuss my wife’s breast augmentation incisions options. We had a follow-up question for Dr. Eppley regarding one aspect of the proposed augmentation that we were hoping he could comment on.
We visited with another plastic surgeon later today,who suggested that because of her ever-so-slightly nipples facing outward and to the sides and not completely to the front, he would most likely insert the implants somewhat to the outside edge of her breasts so as to promote a more inward-facing profile of her breasts post-surgery. In effect, the surgeon expressed an interest in being able to have the greatest amount of control possible in the placement of the implant during surgery. To achieve this greater control, however, the surgeon advocated for inserting the implants through the areola instead of through the armpit.
While she definitely likes the idea of a transaxillary implant so as to avoid the presence of scars on her breasts, we would like to understand whether in fact it’s true that this approach might not give as much control around the implant placement, especially given her particular physical circumstances. Could you give us some perspective on this issue and whether indeed there’s a tradeoff here between the two insertion approaches that we should more carefully consider?
A: It is important to understand that the location of the incision in breast augmentation is largely about access to the submuscular and subfascial breast planes..once you are in there what is done is the same…the development of the implant pocket. Considerable experience and skill allows a plastic surgeon to use any of the incisions will equal ability to make whatever pocket one wants. Plastic surgeons frequently use only one incisional approach because that is what they are most comfortable doing so it eventually becomes the ‘best’ way to do the operation…and if that is what their comfort zone is then it is in fact the best way for them to do it. But the areolar incisional approach offers no advantages in terms of visibility or pocket creation than either the transaxillary or inframammary approach breast augmentation incisions.
One of the keys to breast implant placement is to get it centered on the existing breast mound. Trying to place it more to the side so the nipple might be ‘pushed inward’ is not going to create that effect and tuns the risk of having an implant becoming lateralized or ending up too far to the side of the chest wall. This is one implant location to avoid as it is a difficult problem to fix later. It is far better to accept some minor nipple location flaws than to create what may turn out to be a bigger aesthetic problem later.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in the customized one-piece jawline enhancement. I live in Sweden and have been talking to a doctor in NY who is using implants made of Medpor instead of silicone for the mandibular angles. Medpor is a material that your body grows into therefore the risk of misplacement or jawline breakdown is reduced.
1. Is it possible to have the custom implants to be made in Medpor instead?
2. Could you send me at least 10 before and after pictures of patients who have had jawline enhancement with the custom implants?
3. I know the custom implants varies in price but could you give an approximate price so that I know how much money that I need to save?
4. Can I pay 1000 dollars/month?
5. How soon can I have the surgery done? I would prefer to have it done this month or the next since I have my vacation now.
6. How long do I need to stay if I want the custom implants? I read from the Q&A that it takes 3 weeks to get the custom implants from the 3D-scan. After surgery I need to stay probably another 2 weeks right?
7). As I fly in from Sweden, where can I live during my stay and how much will it cost for 5-6 weeks?
A: In answer to your questions about a custom one-piece wrap around jawline implant:
- A custom one-piece jaw implant can only be made of silicone not Medpor. Even if it could be made of Medpor, it could never be placed as a single piece. That material is too stiff and would need to be sectioned into three pieces to place it…but even that would not be easy. The ingrowth of tissues into Medpor often poses more problems than it ever solves, particularly if you have to revise, replace or try to remove them. A custom implant does not shift because of its precision fit.
- Due to patient confidentiality, we do not distribute patient photos randomly across the internet.
- I will have my assistant Camille pass along the cost of custom jawline implants to you tomorrow.
- Surgery fess must be all paid in advance not in partial payments after the procedure.
- It would take a minimum of three weeks just to have a custom implant fabricated. Thus unless one wants to use a three-piece implant approach with standard implants it can not be done this month.
- The 3D CT scan is done in your country and send here to make the implants. You come here one day before the surgery and return home 48 to 72 hours after the procedure.
- You only need to be here a few days to have the actual procedure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I asked you about my skull shape problem before but I don’t think I’ve describe it accurately.The problem with my “big head” has been troubling for years and I hope to resolve it once and for all.
Here is my problem:
My head looks normal when viewed from the front or back. But when viewed sideways, it looks big. Specifically, the distance between the forehead to the back (the occipital region) is too large.
If one would to look at the top of my head from a bird’s eye view, the back region is sort of a “trapezoidal” shape, in that the middle portion protrudes too much out. I wonder if it’s possible to “push back” on the middle portion and fill up the side, so that the head will be a more flat or rounded shape rather than trapezoidal.
I think the only way this can be done is via a partial removel of the skull, and putting it back like a jigsaw, or maybe even replacing that portion with an artificial skull. I wonder if this is within your specialty. I heard the risk of death or disablement from this might be as high as 50% so I might not do it if that’s the case.
My goal is to reduce the said distance between the forehead to the back by 20mm. On your website, most of the skull reduction procedure I’ve read about deals with mechanically removing a portion of the skull and making it thinner. I’m not sure if that would be enough in my case. I’ve read that the human skull thicknes is only about 10cm thick at most.
A: Realistically what you are asking can not be done. The outer portion of the skull can be shaved down by removing the outer cortex. When done in the forehead and occiput, the anteroposterior (front to back) distance can be reduced probably 10 to 12mms at best. You can not remove skull pieces and put them back together any way you want because of the space occupied by the brain. This space can not be reduced or intruded upon, only the outer portions of the skull can be reduced which protects and maintains the intracranial space for the brain.
Dr. Barry Eppley
Indianapolis, Indiana
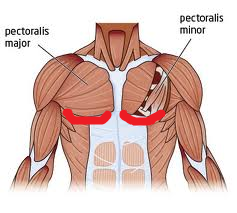 Q: Dr. Eppley, I am wanting to know how much the costs would be for fractional laser resurfacing underneath the bottom outline of my pectoral muscles would be. There are some small, fine wrinkles that I am wanting to treat. I highlighted in red the approximate area in the photo.
Q: Dr. Eppley, I am wanting to know how much the costs would be for fractional laser resurfacing underneath the bottom outline of my pectoral muscles would be. There are some small, fine wrinkles that I am wanting to treat. I highlighted in red the approximate area in the photo.
A: Fractional laser resurfacing is most commonly done on the face which responds very favorably due to its excellent blood supply and quick re-epithelization properties of the skin. As you move below the jawline, and particularly below the neck, greater caution must be exercised as the skin healing properties as not as great as that on the face. This does not mean that laser resurfacing on the chest can not be done…just that it must be done less deep and in stages to avoid creating scarring and hypopigmentation.
I would recommend that you first have a test patch of a certain laser resurfacing depth done to make sure this body area can heal without any adverse effects.
As general cost information, I will have my nurse send to you tomorrow a fractional laser resurfacing series cost.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have some questions about implants for skull reshaping. These are the questions that I would like for you to answer. Thank you for taking the time to answer them.
1) My main concern is to eliminate the cone shape at the top of my head. It appears that using implants would give me better results than just burring the scalp. Which one of the two do you believe would give me the best possible aesthetic look? Meaning the most proportional/normal looking head? If I can achieve a normal shaped head, “with implants only” I do not see the need for you to burr the scalp. However, if you believe that implants “alone” cannot give me the best possible shaped head, I would go with the option where you burr and insert implants. I don’t think I would have a problem with the height of my sagittal crest if the sides of my head would not be so slanted.
2) If you only use implants and do not burr the skull down, would this create too much tension on the top of my head? Will the skin on my head once pulled over the implants create too much tension that would then lead to pain in my head?
3) Am I going to be limited in the kinds activities I could take part in? For example, would an activity like diving head first into water be considered unacceptable for fear that the implant will move out of place?
4) Does this procedure require maintenance? Will I have to replace the implants after time goes by? Or can I can I live out my life without having to worry about it again?
5) What kind of material are the implants made from?
6) How long until the scar is completely healed, or the time frame when I will know the scar will look as good as it’s going to look?
A: 1) That is why I do computer imaging to look at all options available for skull reshaping. By looking at the head shape outcomes from all three methods, YOU can make that determination. This is a purely aesthetic judgment of what you think looks the best.
2) No, The skull implants are not that big.
3) No, you would have no physical restrictions and they will not become displaced no matter what you do.
4) The skull implants are permanent and will never need to be replaced.
5) They will be custom implants made of solid silicone elastomer and will feel just like bone.
6) Scars take put up to six months to fully mature. Although many scalp scars do well and mature before that time period.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a deviated nose and feel pressure in my nasal bones. ENT doctor said nasal passage was clear from what he could see and prescribed allergy meds for constant stuffiness and post nasal drainage. Wondering if any chance insurance would cover any of my deviated nose repair procedure to improve how I breathe and the way the nose looks.
A: Insurance can cover internal nasal surgery for breathing issues such as septoplasty and turbinate reductions. These are often done as part of many rhinoplasties and fall under the name of septorhinoplasty when both functional and aesthetic nasal changes are done during the same operation.
Before one can submit to insurance to determine whether coverage is possible, this would require a paranasal CT scan to first be obtained to look at the internal nasal anatomy and see what abnormalities exist. If structural problems exist that block the nasal airway then a predetermination letter can be submitted to insurance to determine whether they would cover the functional surgery to correct it. You can not submit a predetermination letter without a CT scan to document what anatomic abnormalities exist inside the nose.The aesthetic part of the rhinoplasty (any external changes) would not be covered by insurance.
Dr. Barry Eppley
Indianapolis Indiana
Q: Dr. Eppley, I have a question about chin augmentation. I am on Remicade for Crohn’s disease and was wondering if you have experience working with patients on Remicade and any recommendations you might have for them when undergoing chin implant surgery.
 A: Remicade or infliximab) is a TNF-alpha (tumor necrosis factor alpha) blocker used to treat inflammatory bowel disease. (IBD) It is effective in Crohn’s disease and ulcerative colitis since IBD patients have more TNF-alpha in their systems than people without IBD. Remicade is usually given by infusion every 8 weeks. The best way to reduce the risk of infection or wound healing problems is to do surgery 6 to 7 weeks after their last Remicade infusion. Then have the next Remicade infusion 2 to 3 weeks after surgery. This balances the increased risk of infection versus the risk of a flare up of IBD symptoms.
A: Remicade or infliximab) is a TNF-alpha (tumor necrosis factor alpha) blocker used to treat inflammatory bowel disease. (IBD) It is effective in Crohn’s disease and ulcerative colitis since IBD patients have more TNF-alpha in their systems than people without IBD. Remicade is usually given by infusion every 8 weeks. The best way to reduce the risk of infection or wound healing problems is to do surgery 6 to 7 weeks after their last Remicade infusion. Then have the next Remicade infusion 2 to 3 weeks after surgery. This balances the increased risk of infection versus the risk of a flare up of IBD symptoms.
Since chin augmentation surgery is a fairly small insult on the body, this approach may be unnecessary. But I have used it successfully in the past for cosmetic surgeries far more major than chin augmentation such as tummy tucks and breast augmentation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had cheek implants and paranasal implants placed overseas two months ago, but it appears that the ones on the left side have been infected (yellow drainage, mild swelling). My issue is that I do not have the time to get them removed right now. I’m thinking of going to a local doctor to get antibiotics to try and control the infection in the interim. If I do that and wait till year’s end to remove them, will it cause any permanent issues (excessive tissue scarring)?
As for the removal, have you ever had any cases whereby you only removed the infected implants? I understand that this will cause asymmetry, but could I use fillers for the side where the implants were removed to compensate (at least until I get the implants reinserted)?
Finally, would waiting 6 months before reinsertion be enough time for the tissues to heal and for the infection to clear? Or, would you recommend waiting even longer?
Sorry for these questions, but I can’t seem to contact my original surgeon right now, and I was hoping you could just help assuage some of my concerns.
A: This is disappointing that you trusted a doctor to do the surgery and now you can not get a hold of him to answer the most basic of questions when you have a problem that he created.
In short, antibiotics will only keep the problem at bay temporarily with infected cheek implants. Leaving them in, if infected, is just going to cause a lot of scar tissue that could make future surgery problematic. If infected it is in your best interest to have them removed, let it heal and then reinsert 3 to 6 months later. Injectable fillers or fat injections should not be placed into the cheeks after implant removal for a minimum of 6 to 8 weeks after the infection has cleared.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have spoken with you in the past regarding jaw implants and chin implants. Through looking at your case examples, I feel as though custom implants produce the best results. Quite frankly, the results you are getting are incredible.
In looking at your recent example: http://www.exploreplasticsurgery.com/tag/male-custom-jawline-implant
I was hoping you could tell me the dimensions of the implant for the jawline (vertical and lateral) as well as the chin, just so that I could get an idea of what what kind of changes are produced from a given size (though I know it will be different for each person). Also, is the recovery easier with a custom implant as opposed to an “off the shelf”?
A: Your assumption is correct about custom jawline implants on two counts. First, it usually does offer a significant aesthetic improvement over a three-piece jawline enhancement approach. This is not only because that it is one continuous piece, which is very much like the natural jawline, but being able to create the individual dimensions of the chin and jaw angle that best suits the patient can be a huge advantage over standard chin and jaw angle sizes. Second, the jawline dimensional changes that are used for each patient are unique to them. Thus, the implant dimensions used for one patient should not be attempted to be transferred to any other patient and assume they would get a similar result. Since they are no software programs that can tell the surgeon what any dimensional change of a custom designed implant will really look like in the patient, it takes a lot of experience to learn what will work for each patient. Thus I do not provide numbers for jawline implant measurements unless I am actually designing the implant for them.
The amount of tissue dissection for a custom jawline implant or a three-piece standard chin and jaw angle implant approach is really the same. Thus the amount of swelling that results and the recovery should be similar between the two implant approaches.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in having a tummy tuck but do have a bit of a twist with my medical history. I have rheumatoid arthritis and have been on Xeljanz 10mg twice a day to control my symptoms. It has controlled them fairly well and I am not keen on potentially going off of it to have surgery. Can I have a tummy tuck while on this medication?
 A: Xeljanz, known generically as Tofacitinib, is a recently approved drug (2012) for the treatment of rheumatoid arthritis. It works as an inhibitor of the enzyme janus kinase 3 (JAK3) which interferes ultimately with DNA transcription in the cell nucleus. It helps in arthritis because it inhibits production of inflammatory mediators in joint tissue. As an inhibitor of the inflammatory process, the drug is known to increase the risk of opportunistic infections such as tuberculosis, cancers and lymphomas.
A: Xeljanz, known generically as Tofacitinib, is a recently approved drug (2012) for the treatment of rheumatoid arthritis. It works as an inhibitor of the enzyme janus kinase 3 (JAK3) which interferes ultimately with DNA transcription in the cell nucleus. It helps in arthritis because it inhibits production of inflammatory mediators in joint tissue. As an inhibitor of the inflammatory process, the drug is known to increase the risk of opportunistic infections such as tuberculosis, cancers and lymphomas.
But as it relates to surgery, the key questions are does it present an increased risk of infection or in any way impede wound healing?This would be particularly relevant in a large healing wound like that of a tummy tuck. There is no specific information in the medical literature that addresses the specific effect on wound healing of the Xeljanz medication. This is likely because it is relatively new although almost all anti-rheumatoid drugs, with the exception of corticosteroids, have a similar void of specific information on their effects on postoperative wound healing.
What I can find is from the newsletter Drug Safety Quarterly Fall 2013 issue which has an article entitled ‘Wound Healing and Anti-Rheumatic Drugs’ authored by Drs. Goodman et al from NYU. From it I quote…
‘Healthy wound healing proceeds through an inflammatory phase, followed by wound remodeling and finally re-epithelialization of the skin edges. These are the normal sequential stages of wound healing. Patients with rheumatoid arthritis (RA) are often on multiple medications to control their symptoms. These medications may include analgesic, anti-inflammatory, biologic or synthetic disease-modifying antirheumatic drugs. (DMARDs) With the exception of methotrexate, there are very few controlled studies that have evaluated the effects of these medications on wound healing and infection risk after surgery.’
‘…with the exception of methotrexate, there is a lack of data regarding optimal practice for perioperative management of antirheumatic treatment in RA patients undergoing surgery. Existing data, however, indicates that methotrexate may be continued throughout the perioperative period for otherwise healthy individuals. For the other anti-rheumatic drugs, while continuing medication may hamper wound healing and predispose to infections, discontinuation may lead to disease flare, which increases the need for corticosteroids or other medications that may also increase the risk for inadequate wound healing and infection to regain disease control. Moreover, there is no consensus among the various rheumatic disease societies regarding optimal practice. Although there are clear effects of anti-rheumatic therapy on wound healing and clear infection risk, the role of RA inflammatory activity on wound healing, infection, and rehabilitation should also be considered. For surgeries such as the implantation of a prosthetic joint, where surgical site infection carries significant morbidity, current practice favors a conservative approach.’
This summary comes from an institution that is performing joint replacements in orthopedic surgery. So these types of patients have significant functional and pain issues related to joint dysfunction. So accepting whatever increased wound healing or infection risk may be worth the trade-off for the benefits. Tummy tuck surgery is much more elective and those unquantified risks must be considered even more carefully.
This is a good discussion you should have with your rheumatologist. He/she probably will not be as understanding about tummy tuck surgery as the need for a joint replacement. But in the end you should follow their advice. The only thing we know for sure is that you are at some increased risk of potential wound healing problems or infection if choosing tummy tuck surgery while on Xeljanz but the magnitude of that risk is unknown.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had jaw surgery just over a year ago and it left me with some irregularities. This led me to get chin and paranasal implants a month ago. While they have provided some improvement and there is still some swelling, they still have not completely solved the appearance of nasolabial folds and pre-jowls.
 I now suspect that this may be a soft-tissue problem. However, because I am only 25 years old such soft tissue deficiencies seem unusual. Anyway, I’ve googled facial fat grafting and this image really pinpoints the areas I would like to build up and bring forward (the direction of the arrows). My biggest questions are as follows:
I now suspect that this may be a soft-tissue problem. However, because I am only 25 years old such soft tissue deficiencies seem unusual. Anyway, I’ve googled facial fat grafting and this image really pinpoints the areas I would like to build up and bring forward (the direction of the arrows). My biggest questions are as follows:
1) Could my soft tissue issues have been caused by my previous underbite (thereby affecting soft tissue development) or the jaw surgery itself?
2) Given my age, can fat grafting be done for these regions? If so, how much volume of fat is usually required?
3) Instead of fat grafting, are permanent fillers an option? Alternatively, are there any different implants that can be placed in these regions?
4) I have implants near these areas. Can fat grafting be done safely without infecting my implants?
Anyway, I also had some fat grafting done to my brow ridge and central forehead to make it look masculine. My surgeon did a decent job, but I’m noticing that insufficient fat was placed in the central forehead (the area between the two eyebrows and just above the nose), which means that my outer/lateral brow ridges are more augmented than the inner portion, causing it to look like I’m constantly frowning. I’m looking to add more fat to the central forehead, but I understand that a revision should only be done a few months later. Regarding this, I have a couple of questions:
5) It has only been 4 weeks since the fat grafting, can I use temporary fillers to augment the deficient areas in the meantime?
6) If so, will fillers affect how my fat graft survives at this stage?
A: I am going to assume that your jaw surgery was orthognathic surgery, possibly a mandibular advancement osteotomy. But that issue aside, let me address your specific facial fat grafting questions.
- The cause of your nasolabial folds and prejowls is impossible for me to comment on since I don’t know what you looked before your jaw surgery or your most recent facial implant surgery.
- While injectable fat grafting can be done for these areas, how retentive it will be is somewhat dependent on your body habitus. Thin young people usually have a poor rate of fat graft survival and retention. The fat graft volumes needed for the nasolabial folds are 3 to 5ccs per side. The prejowls usually require a similar amount of injectate.
- There are few permanent fillers available in the U.S. and, even if there were more, I would not use them. All of the so-called permanent fillers run the risk of lump and nodules. While more often these do not occur, but if they do they are problematic to treat. Other styles of facial implants may indeed be more effective than what you have such as a true maxillary implant. (combined medial and lateral maxillary coverage which is much ore comprehensive than a simple paranasal style which I find archaic and inadequate for many midfacial hypoplasia needs)
- Fat grafting is done above the level of the bone where the implants reside so they are not in danger of being accidentally injected.
- I would probably wait another month before placing synthetic fillers into the fat grafted areas. The fat grafts are still healing and there is an increased risk of causing an infection by introducing another material into these areas.
- At 8 weeks after fat grafting, injectable fillers will not have any adverse effects on the outcome of the fat grafting.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 26 year-old male from Europe. I have a major concern about the proportionate shape of my temples, specially above ears. The muscle in the region is very thick and also the bone is protruded to large extent which makes heads looks very big. So I have decided to contact you as I can see you are the only one having expertise in this area of plastic surgery.
I have some questions regarding this:
1) How much muscle can be reduced..does this involves any risk?
2) How much muscle can be reduced?
3) How about narrowing the width of the forehead near the hairline?
4) Will this make considerable changes in my appearance?
5) What will be the recovery time?
6) What will be the cost of the surgery?
7) Iit possible to come for consultation and surgery once as coming to US twice will not be feasible?
A: In answer to your questions about temporal reduction surgery:
1 and 2) Usually the entire posterior belly of the temporalis muscle above the ears is removed. This constitutes a thickness of at least 5 to 7mm per side, sometimes even more depending upon the thickness of the muscle. I have seen temporalis muscle as thick as 10mms in some patients. Removal of this portion of the temporalis muscle causes no functional loss of jaw movement or any other disability.
3) Reducing the temporalis muscle near the eye and just below the forehead is a different matter than that at the sides of the head. This muscle can not be surgically reduced. It must be treated with Botox injections if any reduction in thickness is to be achieved.
4) Changing the convex shape of the head above the ears to more of a straight line (and hence narrowing the head width) is seen by those so afflicted as providing major improvement in their concerns.
5) Temporal reduction surgery has a very quick recovery time with little discomfort and minimal swelling. The change in temporal appearance is immediate.
6) I will have my assistant Camille pass along the cost of the surgery to you on Monday.
7) There is no need to come initially for a consultation. All before surgery discussions etc can be done by e-mail or Skype video. You would only need to come for the surgery and could return home within 48 hours after the procedure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have some questions about a custom jawline implant.
1) Does having a custom jawline implant that increases chin dimensions of 15 mm or so place undue stress on the bone? Presumably not, otherwise this wouldn’t be discussed as an option.
2) You had mentioned off the shelf mandibular angle implants are two wide in many cases. Would that hold true in my case?
3) Since my previous implant created a pocket, will this be favorable to swelling in that area?
4) What type of lead time do you need when designing this implant prior to surgery? I don’t think I’m as concerned about quantifying millimeters as other patients may as I am with having some broad criteria of the implant not looking overly large and unnatural.
5) You had mentioned getting Voluma prior to surgery would not affect things. There’s a surgeon locally adding this to his practice and providing this for free if I want to slightly accentuate the jaw angles. I don’t know if this issue still holds true with this custom implant option. I would assume in the worst case scenario this product could be dissolved, however, I don’t want to risk affecting this process in the future or perhaps even the 3D scan somehow.
 A: In answer to your custom jawline implant questions:
A: In answer to your custom jawline implant questions:
- A larger implant, like the custom jawline implant, distributes its forces (stress) on the bone over a very wide surface area. Thus one does not see the traditional implant settling phenomenon that can occur from an isolated chin implant.
- Most patients, men or women, need a vertical lengthening component to their jaw angles not just width. Most current styles of jaw angle implants only add width and very little if any length to the jaw angles.
- Having an indwelling implant with an existing pocket will tend to create less swelling in that area with a new implant than during the initial implant placement surgery.
- From obtaining the 3D CT scan to having the sterile implant in hand ready for surgery is a three week process.
- Getting a synthetic injectable filler, like Voluma, will not interfere with the images obtained in a 3D CT scan. It will also not interfere with placing any jawline implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I came across your web site while googling for plastic surgeons. Six months ago I got hit in the forehead with a beer bottle (blunt trauma). The plastic surgeon only looked at the injury two days later and applied micropore tape rather than stitches. Around a month ago, I started going to to a few local plastic surgeons to see what could be done about the car. All the surgeons having different ideas on what to do. I really don’t want to have to travel overseas for treatment, but I do want the very best results (as I’m stuck with my face the rest of my life).
It seems like the local surgeons have the following two schools of thought:
1) To wait until a year has passed, and re-evaluate. I do not like this option, as it seems to be getting worse as time goes on, not better
2) To cut out the scar and re-stitch it. Within this there are 3 opinions:
a) Cut out the scar, and remain with a horizontal line which conforms to my face’s natural lines.
b) Cut out the scar in it’s current orientation (around 45 degrees), because it can not be adjusted to a horizontal orientation without doing a z-plasty
c) Make a horizontal cut through the middle of the scar, leaving a small vertical mark on the top and the bottom (which the plastic surgeon claims will disappear)
Within the opinions above:
1) No surgeon was exactly sure what is causing the scar to bulge. Some claim it is excess scar tissue from not being stitched initially after the injury. Others claims it is a cyst that has formed. Another claims it is some kind of “fluid” under the scar. Keep in mind that the bulge currently feels more like a hardish jelly that a hard bump.
2) I have asked each one regarding geometric broken line scar revision. Some just refer to the Z-plasty or W-plasty when I mention that word. They claim that W-plasty is not necessary as the scar is small and with a straight cut, it will eventually result in a smooth white line. Some even suggest that making any jagged patterns will make it more noticeable.
3) I have also asked regarding dermabrasion and/or laser. All of them have said that as long as the surgery is ok, and healing goes normally, they do not see any reason for dermabrasion or laser. Only if the scar looks like it is becoming hypertrophic will they apply some extra treatment.
4) I have also asked all of them about botox before surgery. They all claim it is unnecessary.
5) Regarding final outcome, some surgeons claim the scar will be a fine white line, others claim it will almost disappear, and others say “we can assume it will be better than it is now, but no guarantees”. From one end of the spectrum to the other?!
So my question is:
1) Is there any way to get it horizontal without Z-plasty?
2) Would a straight cut be better than GBLR?
3) Is demabrasion/laser really necessary?
4) What is your personal recommendation at this point? Am I taking a risk doing it locally, and if not, which school of thought should I trust?
Sorry for the long winded message. Just spent hundreds of dollars and hours
trying to find someone who is confident and know what they are doing,
but it seems hard to find someone who can suggest the best and most
optimum treatment locally.
Thanks in advance for your help/advice.
A: I will take your very detailed description and various opinions and summarize your forehead scar revision issues/recommendations succinctly.
This is a hypertrophic scar and would be expected given the original unrepaired wound. There is no mystery as to why it is there.
Totally removing the scar (excision) is the most expeditious and effective method to getting to an eventual better scar. Everything else is just wasting time and effort.
The excision should be based on a stair step pattern closure to at least get 50% of the scar horizontal.
Botox injections should be done at the time of scar revision. (not before so the wrinkles lines are well demarcated) This will provide several months of tension free healing in the critical few months after the procedure
Microdermabrasion or light laser resurfacing may or may not be needed afterwards based on how it heals.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a custom jawline implant option and have some questions about it. You have mentioned that this particular implant will be able to address all of the following aesthetic issues of my jawline:
- Address the approximate 10 or 12 mm horizontal chin deficiency
- Address the approximate 5 to 7 mm vertical chin deficiency
- Address vertical and width dimensions of the mandibular angle (curious how this is accomplished if I visualize this as a chin implant with very long wings as this looks quite different than an off the shelf mandibular angle implant)
- Account for any existing jaw asymmetries
- Creation of a continuous jawline from to the chin back to the mandibular angle
I can see that this certainly seems favorable considering the decreased operating room time and relative cost between alternatives involving multiple procedures and implants as you explained.
A: You have thoroughly hit on all of the aesthetic benefits that a custom jawline implant would provide. And it is also the only way you could achieve all of these dimensional jawline changes with a single implant. Such an implant is not really an ‘extension’ of a chin or jaw angle implant. Rather it is an implant that accentuates the entire jawline rather than just being a forward extension of a jaw angle implant or a backward extension of a chin implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had cheek implants and facial liposuction two weeks ago. Since my procedure I can’t feel my upper lip and it still doesn’t move like its supposed to with no improvement since the first day after surgery. Is it highly likely something was transected or the fat closer to my lip was removed along with the nerves? The doctor did it through the same incision used for my cheek implants implants rather than one further back and it concerns me both sensory and motor function are absent from the same spot and there has been no recovery in more than two weeks.
A: It is not rare that numbness and facial muscle movement are temporarily impaired after cheek implants, particularly when it is combined with facial liposuction. It would be highly unlikely that any nerves were transected. But it could easily take up to three months or longer after the procedure for both normal facial feeling and lip movement to return. Two weeks is way to early for these small facial nerves to ‘wake up’ and begin functioning. Your sense of what is normal and how nerve recovers is understandably limited to this present experience. But it takes much longer to return to normal that most patients think after any form of midface surgery including cheek implants.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a chin implant revision. I had a silicone chin implant a few years ago which was terrible and looked awkward. So 1 year ago I replaced it with a Medpor chin implant which is no doubt much much better than that original nightmare. But this Medpor chin implant does not look rigid as opposed to silicone. It looks more like a “U” shape instead of “V” shape. The edges are not sharp as opposed to the famous MB picture either. So what is your suggestion, is it possible to add some medpor cuts to the edges to make it look more sharp do you think? Or is it a common issue with all Medpor chin implants? Thanks a lot for your great experience and knowledge.
A: The success of any chin implant to create a specific chin shape is not material based. It depends on the shape of the implant and the thickness of the overlying soft tissues and underlying bone shape. You did not state what style of Medpor chin implant you have which would be helpful to know. But Medpor implants in general are thicker and ‘bulkier’ than most silicone implants because the material from which it is made is machined into shape rather than poured into a mold like silicone.
The ideal chin shape image you are showing is more of a square shape unlike yours which is more circular and long. Whether your existing chin implant can be shaped into that form would depend on knowing what shape and thickness your existing implant is. It certainly could be improved but tot what degree can not predicted without further information. Medpor implants are generally bulky and some improvement in its form can usually be obtained by giving it a more angular shape.
I would point out that shaping an indwelling chin implant has its limitations based on the existing incision length and access to it. It is often better to place/replace an implant that has been shaped before it is put in with the dimensions that one wants.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had cheek and paranasal implants placed in another state 4 days ago before flying back (1 hour flight). I think I have developed a slight cold, and have a slight runny nose while coughing up some phlegm too. My biggest worry right now is that there is some ‘squishiness’ when I press on my left cheek. Are there signs of a cheek implant infection, and what can be done for it?
Anyway, I’m still taking my antibiotics as prescribed, and there are no other symptoms (no redness, excessive swelling or fever). I’m hoping that I don’t have to get these implants removed, which is why I’m seeking your counsel with regards to what I can do.
Thanks for any help rendered!
A: I would not consider this squishness to be a sign of cheek implant infection. Most likely it is due to the positioning of the implant and/or a little fluid around it since it is so early after surgery. Many cheek implants are placed partially off the bone and/or are not screwed into position. This will allow the implant to ‘float’ around for awhile until scar tissue settles and secures it down. Further healing will also allow any fluid around the implant to be resorbed.
Dr. Barry Eppley
Indianapolis, Indiana