Your Questions
Your Questions
Q: Dr. Eppley, My son is 5 years old and was born with scalp aplasia cutis congenita. Around 3 x3 xm on the scalp. The dermatologists does not wish to help us correct this until my son has a say on this when he is older which I think is ridiculous as a parent.
A: Thank you for your inquiry. Congenital scalp cutis aplasia areas can be excised at any age. The real question is not whether it can be excised but whether it can be primarily closed without undue tension or excessively long incisions from scalp rotational flaps. Scalp surgery in a growing head is interesting in that scars do expand with growth so many of these scalp surgeries require further surgery in the future for scar widening from the expansion of skull growth. But certainly it can be substantially reduced. I would need to see some pictures of it for further assessment.
Some cutis aplasias have either very thin skull bone underneath them or rarely I have seen them with areas of missing skull bone underneath them. But I assume that the latter is not evident in your son’s case.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Im writing to you because i find your work amazing! I want to do several aesthetics procedures with you. But i have a big big problem, who makes me sad everyday…..
I would like to find a definitive solution for my shoulder. I have a skin congenital atrophy yon my shoulder. (lack of fat?? or I don’t know I was born like this). It looks like a crater. I was looking for doing PMMA injections on it as I have already had multiple fat injections and they didnt work.
It would be my biggest dream to find a permanent solution, without thinking about doing several injections, or taking care or my weight for not loosing graft, or be able to use my shoulder.
Is that possible for you, to customized an implant for me? To fill the hole? Like this it would be definitive! I found a doctor in China but I have seen your work and it would be amazing if you can help me.
Thank you in advance doctor!!!
Have a very nice day!!
A: Thank you for your inquiry and sending your pictures. That shoulder appears to have a congenital subcutaneous atrophy/dermal thinning. While injection fat grafting would be the obvious solution, having failed that numerous times it is time to try something else. While the implantation of ‘something’ would be the correct alternative, and one could use an implant (ultrasoft thin sheet of perforated silicone), I would think first about an allogeneic dermal graft. (e.g., Alloderm) This very pliable sheet of 2mm dermis would act like an implant from a fill standpoint but it would be incorporated into your tissues which I think is better long-term in such a high motion area.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am 21 years old and I have plagiocephaly which has never been treated. The cranial malformation does not bother me but the asymmetry of my face is really showy and ruins my life, I am in depression because of this, I have no social life. I send you photos of my case, hoping that there are solutions. Thank you for taking the time to read me.
A: Thank you for your inquiry and sending your picture. You have a left facial asymmetry that is complete, meaning it extends from the forehead down to the jawline, and the entire side of your face is shorter vertically than the other side. You have an inferior-based facial asymmetry which means it affects most the inferior part of the face (jawline) and becomes less severe as one heads further up on the face.
Like all complete facial asymmetries the patient has to prioritize the facial features that are most important to improve or will create the biggest difference. Technically a complete facial asymmetry surgery involves an endoscopic browlift (to raise the lower eyebrow), vertical orbital dystopia correction (raise up the eye), cheek augmentation, nostril repositioning, mouth corner lowering and chin/jawline augmentation. From your viewpoint what asymmetric facial features bother you the most?
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello there, I’ve been looking for someone that could offer skull reshaping surgery for years and have just discovered you! I suffer from scaphocephaly, its bothered me for years to the point where, now at 28 years old, I need to do something about it. I understand I probably wouldn’t achieve a normal head shape, but anything to improve the overall look would make such a difference to my self esteem.
How much would this cost roughly?
A: Thank you for your inquiry and sending your pictures. In the scaphocephalic skull it is long from front to back and narrow on the sides. With your hair and the angle of these pictures all I can appreciate is the narrow forehead/temporal areas outside of the hair zone in the front. Please tell me what would be the significant part of it to change from your standpoint so I can devise a skull reshaping surgery to do so. Once I know exactly what needs to be done then my assistant can pass along the cost of the surgery to you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I underwent otoplasty nearly 30 years ago and and the results were very average. In my opinion, the tips of my ears were pulled back too far and now appear very flat if not contorted. I have tolerated it for this long, but now my hair is starting to thin I’m becoming more conscious of it.
Aside from traditional cut and stitch, are there any other methods available now that could achieve a more ‘natural’ look? I’m a bit wary about going under the knife again.
A: Any attempt at trying to shape your ears as an adult requires surgery. There are no non-surgical efforts to do so. That is only done right after birth when the east cartilages are moldable by external means. But that ear reshaping capability is lost months after birth. I would need to see pictures of our ears to provide any surgical insight.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a 9mm medpor chin implant placed last year from a submental approach which was not secured by the screws. One month after 1 surgery it shifted. Then two small titanium screws from an intraoral approach were placed but it shifted again. Thereafter two larger titanium screws were inserted also from an intraoral approach. Unfortunately, I was eager to have two more large screws after some trauma placed because I feared malposition which was also done.
Thereafter, I developed scar adhesion after triple surgeries in a 6 month period from the intraoral approaches!!! This creates bumps over the implant, and causes me intermittent numbness and lack of mentalis control.
I’m extremely frustrated… I guess it’s pretty hard to remedy. I know you are an expert on chin implants. I was wondering if it’s possible to deal with this situation? Many thanks.
A: As you have aptly stated stated you have developed scar tissue from multiple intraoral entrances through the same incision. Like scar adhesions anywhere on the body they are treated by release and the placement of an interpositional soft tissue graft of which my preference is a autologous dermal fat graft. This will certainly remedy the scar adhesions, where that also improves mentalis muscle function fully can not be predicted beforehand but the two are almost always related to a significant degree.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m still torn on which midface surgery I should undergo.
I can’t tell if I have a recessed or average maxilla, but if that turns out to be the case, will your maxillary implants be able to create a protruding maxilla to the same extent as a lefort II or lefort III procedure? I don’t have an overbite, and according to this test I have an average/slightly receding maxilla.
“1. Make a picture from the side while smiling
2. then compare the sagittal position of your front teeth compared to the nasion (image a vertical line from the nasion – nasion line)
results:
if your teeth are at the same lvl with the nasion line your maxilla is average
if your teeth are beyond the nasion line your maxilla is protruding
if your teeth are behind the nasion line your maxilla is recessed”
Thanks a lot for the help,
A:Thank you for your inquiry and detailing your concerns. With an ‘average to slightly receding maxilla’, regardless of how that is determined you are certainly never going to undergo any form of a LeFort osteotomy advancement unless you have a compelling need to bring your lower jaw forward as well. Modified midface osteotomy designs that leave the occlusion alone are poor substitutes for what a custom midfaceimplant can do because of the magnitude of the surgery and the resultant irregular osteotomy lines and bone contours. Bring the midface out in a smooth and contiguous fashion that is predesigned for the aesthetic effect produces superior results. The only thing that a midface implant can not do is change the occlusion but that is what osteotomies are for which is their primary benefit.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi I’m interested in a more rounded head and temple shape. I feel like my head causes asymmetries to my face structure which is very different from both sides. I also don’t like that it looks like I have a long profile view and asymmetrical view from the front. Let me know what you think.
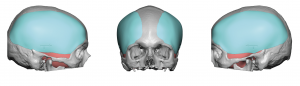 A: Thank you for your inquiry and sending all of your pictures I believe you are referring to what many such patients described as a ‘pinched head’ where the sides of the head (bilateral temporal area including the sides of the forehead and back of the head) are too narrow. This is consistent with what I see in our frontal view picture and why you describe a desire to have more round or normal shaped head. I treat this head shape with custom fronto-temporal implants (as per the attached custom skull implant design images) which provides increased head width from front to back. Such implants are placed mainly through an incision begin the ear with a few very small scalp positioning incisions.
A: Thank you for your inquiry and sending all of your pictures I believe you are referring to what many such patients described as a ‘pinched head’ where the sides of the head (bilateral temporal area including the sides of the forehead and back of the head) are too narrow. This is consistent with what I see in our frontal view picture and why you describe a desire to have more round or normal shaped head. I treat this head shape with custom fronto-temporal implants (as per the attached custom skull implant design images) which provides increased head width from front to back. Such implants are placed mainly through an incision begin the ear with a few very small scalp positioning incisions.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to start by thanking you for taking the time to reply my email. I would like to convey how grateful I am for your email. I love how the Vertical Lengthening Chin implant looks on my face. I had a relatively small chin so the s size of the VLC was perfect. It gives my face a longer and sharper look. So thank you so much for designing this. The only problem that I am having so far (I’m on day 4) is that the part where the implant ends (under my chin, close to my neck) is protruding out of my skin and is very apparent, almost as though it’s not sitting on my jawline. I am aware that this may be swelling. Also during surgery, I asked my surgeon to trim the implant if needed, he did not do it as he probably didn’t think it was necessary. I’m worried that these lumps on my neck will remail there. I would really like a smooth jawline. Have any of your patients complained of similar instances? I would like to apologize if my questions are silly. I’ve just been a little stressed out.
Once again, thank you so much for your precious time.
A It is not exactly clear to me what your mean by ‘protruding from my skin…and… not sitting one my jawline’ without any visual or doing your actual chin implant surgery. What I do know about any facial implant ss that the combination of swelling which peaks at day 3 and doesn’t really go down enough to tell much for weeks after surgery freaks out a lot of people early on. My usual statement is ‘this is not instant oatmeal’ and trying to make any assessment now about the result or shape is meaningless since everything is so distorted.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am inquiring about having a bulbous rhinoplasty done and am hoping for a symmetrical, smaller, thinner and narrower nose, including the nostrils. What is the cost? I have also sent 7 pictures.
Thank you
A: Thank you for your inquiry and sending your pictures Like many bulbous nose patient you have thick nasal skin which does provide some limitations as to how much thinner/more narrow your nose can become with rhinoplasty surgery. While I don’t think it is possible to have a substantially smaller or thinner nose, there are improvements that can be made as per the attached prediction imaging. As long as one has a realistic understanding of the limitations of what a rhinoplasty surgery can do in the thick skinned nose patient then surgery can produce a satisfying improvement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi! I haven’t been in for a while…if u remember when I was young I got cheek implants..(somewhere else before I moved here) I fell last week and hit my face hard..my face has been swollen on one side..beside my cheek clear to my nose and down..can my cheek implant bust…I fell Thursday night face is still really swollen clear to my nose…I know its prob just still swollen from fall I hit it really hard…can u ask dr if the implants are hard and wont bust or could implant have busted?
A: Good to hear from you and sorry to hear of your fall. Almost all cheeks implants placed since the 1980s have been solid silicone cheek implants which can not bust for break. I don’t know the exact year when your cheek implants were placed, but it is a 99% probability that they are solid. So your face many be swollen but it is highly unlikely that your cheek implants are ‘broken’.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I just had a few brief questions regarding facial implant surgery. Last year I had custom CT-designed facial implant surgery with another surgeon to place custom cheek and chin implants, which mostly went well. However, even though I like the general design/aesthetic look of the cheek implants, I think they are just a bit small and don’t provide enough projection for my face.
Therefore, I was just wondering if it would be possible for to obtain a copy of the actual cheek implant design file, keep the general design the same, and just change only the dimensions of the implants by adding 2-3 mm of additional projection.
Would a complete revision need to be performed, or could a second set of implants be manufactured and placed on top of my current implants as an “onlay” layer of sorts?
A: That can be done but you want to just make new ones and replace them. Placing one implant on top of another is never as good as having one solid single piece implant….and the surgery is really the same from an access standpoint. So there is no advantage to an onlay approach as opposed to just a complete replacement.
Dr. Barry Eppley
Indianapolis, Indiana
Dr. Eppley, I hope all is well! It has been right about a year since our procedure on my custom pectoral implant for Poland’s syndrome!
Just wanted to give you an update and let you know everything healed great and as a personal trainer, I am back to lifting 5-7 times per week and am stronger than I have ever been!
I have attached some photos below to provide some visuals!!
I also wanted to ask about your recommendation for how long the implant will typically last? And when you recommend getting it redone?
Thanks again so much for your help!
A: Besides that it is impressive that the implant has done so well, your body builder efforts are equally impressive! That is a solid silicone implant so it will never degrade, breakdown or need to be replaced. It will never need to be redone unless there is something from an aesthetic standpoint you want go improve. But other than that I would leave it alone, both it and you are doing well.
As an aside I always wondered how well a pectoral implant, in the presence of lack of muscular coverage over much of the implant and exposed to truly strenuous activities after surgery, would do. I believe you have adequately answered that question.
Good to hear from you and glad to see and hear you are doing well,
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hope you’re well.
I’ve got a question in regards to Custom infraorbital-Malar implants and veneers.
I’m planning to undergo 20 emax veneer procedure shortly after (2-3 months) having Malar implants done by you, however I’m worried about chance of implant infection.
What I mean is when aesthetic is being injected into top teeth in order to shave them down, wouldn’t that increase chance of infection massively as it is pretty close to Malar area?
If true, would having veneers before cheek implants be a better idea?
Looking forward to your reply.
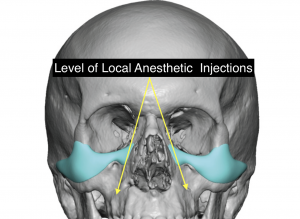 A: That is a good question. But where the level of the custom infraorbital-malar implants are is high comported to the placement of vestibular local anesthetic injections. So I do not see that as a risk. But of course when in doubt consider the reverse…but then there is the remote risk of injury to the veneers from anesthetic oral intubation. It is a small risk but always present. Given the two risk profiles, the risk of implant infection from local anesthetic injections is lower (closer to zero) than the risk of tooth injury from anesthesia.
A: That is a good question. But where the level of the custom infraorbital-malar implants are is high comported to the placement of vestibular local anesthetic injections. So I do not see that as a risk. But of course when in doubt consider the reverse…but then there is the remote risk of injury to the veneers from anesthetic oral intubation. It is a small risk but always present. Given the two risk profiles, the risk of implant infection from local anesthetic injections is lower (closer to zero) than the risk of tooth injury from anesthesia.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had some questions regarding plastic surgery for the lower jaw. How could I go about achieving a sharper, more angular/acute jawline, when mine is very wide and obtuse? Furthermore, I also have a very weak jawline, as it is vertically short. Without implants, would it be possible to vertically extend the lower third by physically moving the lower jaw, similar to the techniques used in bimax surgery (assuming that the upper jaw could be moved as well so that the bite remains the same)?
A: Thank you for your inquiry. To provide a qualified answer to your questions I would need to see pictures of your face /jaw from different angles. But on a basic conceptual basis I don’t see how bimax surgery makes your jawline more angular/acute as it just takes the same lower jaw shape and provides some increased horizontal and/or vertical lengthening. That may help chin projection and provide some jaw lengthening but won’t really make a significant change in the overall jaw shape….at least not by the definition of a more angular and acute jawline shape.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to have a revision canthoplasty with an orbital rim of cheek implant for projection and support. I had a canthopexy a year ago, done by an oculoplastic surgeon which was a failure. Within less than a month my eyes were back to their natural state. This surgeon had also suggested fillers in the temples, cheeks and undereyes to balance out my long face shape and give it volume from the side. What do you suggest for my eyes? I am also open to suggestions for the face.
A: Thank you for your inquiry and sending your picture and a description of your concerns. It is no surprise that the use of a canthopexy in the negative canthal tilt/undereye hollow patient failed to hold its position other than for a very short period of time. Besides the fact that a canthoplasty is needed for more secure canthal positioning, failing to add support for the lower eyelid via either spacer grafts or infraorbital rim augmentation even dooms a good lateral canthoplasty. In the end something must hold the eyelid up or even the most secure form of tethering will likely fail.
As for the longer face the basic approach is to look for vertical shortening and widening effects that would be aesthetically beneficial. Vertical facial shortening could be done by either frontal hairline advancement (upper third reduction) or vertical chin reduction (lower third reduction) or both. This address the long face directly and are the most effective. Widening has a complementary effect of which temporal and/or cheek augmentation are the two choices. Thus you have five types of facial reshaping procedures to consider. Which ones work the best requires computer imaging of them separately or in combinations to see which ones make the biggest differences. You may already have a feel for what you think is most important and if you can tell what you think that is I will be happy to some imaging for you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi I had a question regarding some pricing/ What is the price range of maxillary-infraorbital-zygomatic-malar implant? Is that the same thing as the mask implant that you create?
A: Such midface implants comes in a wide variety of surface areas coverages depending upon the patient’s aesthetic needs. While the design and implant fee remains the same regardless of what midface area is being covered, the surgical fee to place them can change a bit based on the incisional access needed and the operative time to place it. The key is whether it is placed through an intraoral incisions alone or needs a combined lower eyelid access as well. If I knew the general outline of the midface area you want to cover (draw on a facial skeleton image or on a picture of your own face) then we can provide you with an exact answer to your custom implant cost question.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is shoulder widening surgery more dangerous than the shoulder narrowing surgery you offer? Is it possible to widen the shoulders with surgery? Thank you.
A: Shoulder widening is just as safe as shoulder narrowing as it is the same osteotomy cut in the identical clavicle location. The difference is that the risk of non-union is higher in shoulder widening because widening requires a bone graft while narrowing puts two good cut bone ends right together where primary bone healing can occur quickly. It takes a longer time for the bone to travel across the graft to heal in widening surgery. But it is not dangerous, it just has a slightly different risk profile.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am writing because I just got a vertical lengthening chin implant yesterday. I’ve always been so fond of the design and asked to get it. My surgeon, a board certified plastic surgeon had it done for me yesterday. He has a lot of experience with chin implants. He managed to get the implant in and was a little surprised at how big the implant was. However, after putting it in, he says that he’s pleased with how it looks. He did however, not use a screw to secure the implant. He said it was not necessary and instead used sutures. I read from a past instruction from you that it is necessary. Should I be worried about this? Or once my chin heals, perhaps it will not move anymore? Also I feel two lumps under my neck, at the edge of where the implant was placed. Could this just be swelling? Sorry for these questions, I have been very stressed out and worried if I had chosen the right implant. Please do get back to me.
A: While I prefer screw fixation for any chin implant, it is not an absolute must as many surgeons don’t use them and they presumably don’t have any issues by not doing so. Ultimately the implant is secured into position by the enveloping scar which occurs by a month or so after the surgery.
All chin implants will develop swelling beyond where it was placed because of the need to develop a wider pocket than that what the implant actually covers for placement. So everyone thinks it looks too big or has unusual lumps among the jawline/neck in the first few weeks after surgery.
Whether this is the right chin implant style or size for you is not something I can answer for you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi I had a question about cutis vertices gyrata. (CVG) I have mild CVG. I see that you inject fat for its treatment. Is this fat from my on body then transfer to the ridges? If so I guess my question is if I sweat or lose weight doesn’t it shrink? Which it then show the ridges down the road?
A: Thank you for your inquiry and sending your pictures. Your question is a valid one as transplanted fat will still have the biologic behavior from where it was harvested. (this is the same principle as to why hair transplantation works) Since the abdomen is the typical harvest site for most fat injections, theoretically weight gain/loss could make the transplanted fat get bigger or get smaller. However the real question is what amount of weight or loss does it take to see those effects. Most likely it takes a considerable amount of weight gain or loss for that to occur. It is not going to occur from just a few pounds up or down or from working out and sweating.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a younger male and am interested in perioral liposuction to create a more hollow accentuated jawline. I just wonder isn’t some fullness anteriorly desirable to support the skin and create the hollowed out appearance in the middle? Also it says on your site you continue the line down and lipo the jawline/jowl fat, what is the reason for this? – won’t it weaken the jawline and make the skin more likely to sag in a patient who doesn’t have excess fat there?
A: Skin sagging is not an issue in perioral liposuction. The zone treated in perioral liposuction depends on the extent of the fullness which can vary amongst patients. The jowls are only treated in perioral liposuction if there is excess fullness there as well.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m planning to have a sliding genioplasty, I have a recessed chin and a bit of asymmetry. I’m afraid doing it and my front face will be to long, a dr told me I need a 6mm advancement and I told him about the asymmetry he says he cant see it, What do you recommend about the asymmetry and the front face being long?
A: If the preoperative concern is that any vertical lengthening will occur as the chin is brought forward then you plan on shortening the length of the chin bone as it comes forward. That is done by tilting the fixation plate to allow for some vertical shortening.
If you look for your chin asymmetry it is easy to see that really the two sides of the jaws are different. Many chin asymmetries are not just isolated to the chin but are due to differences in the two sides of the jawlines. While subtle it is nonetheless present and if the patient sees it before surgery they will most certainly see it after surgery if unaddressed and may likely appear worse. The chin asymmetry appears to be that the left side is a bit more recessed than the right and may be higher as well. Rather than just guess or ‘eyeball’ how to set the chin bone in its new position a 3D CT scan of the lower face should be done to better understand how to rotate the chin accordingly to account for the pre-existing asymmetry
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,Could I ask you a short question ? You don’t have to help me, but I would be so happy … 🙂 I had a hyaluron injection one week ago. It was “profhilo” (just for skin glow) I was at the dentist today and he pressed his hands on my cheeks for 20 min or so … exactly were the Hyaluron was injected. On Real Self some doctors write about teeth cleanings and bacteria which go into bloodstream while having the teeth done and then it will make an infection in the filler Region or a biofilm…that makes me crazy. 💥
Can this be a problem 1 week post hyaluron inj. ?
Thank you very very very much.
A: I do not see that as causing an infection problem with the injectable filler material. It may distort the shape of the injected filler but would not cause an infection. Biofilms occur as as result of the injection of the filler not from some disseminated bacteria which occurs later.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was very curious about their was any surgery that could reduce the size of a protruding forehead. I was born with a large, protruding front skull (not frontal bossing, just unfortunately how I was born), and was wondering if you were capable of preforming this procedure, as it is something I am insecure about. I am not looking for a hairline lowering procedure by the way. I have seen one notable doctor responding to a similar question saying their is a procedure that is capable of doing this, but didn’t supply much information about it. I hope you read this and are able to answer my concern, and hopefully I will be able to get my concern resolved thank you.
A: Bony forehead reduction, with or without hairline lowering, can be performed in anyone. The question is not whether the protruding forehead can be reduced but by how much and whether that would be satisfactory to the patient. That I can not tell you without seeing pictures of your forehead in profile. Conversely, however, like all skull reductions there are limits as to how much bone can be safely removed. So whatever amount can be removed, even if it falls short of the patient’s ideal goal, is the result a patient has to accept.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a middle-aged man and I have an asymmetry in the forehead where the right side is slightly more prominent, probably positional plagiocephaly. I am very disturbed by it and wonder if you can do something about it. I understand that there are limitations right now in these corona times, but asks anyway. Of course I have pictures if needed. Grateful for the response by email to begin with.
A: Thank you for your inquiry. You are undoubtably correct in that a forehead protrusion is likely the result of positional plagiocephaly whether an ipsilateral occipital flattening is present or not. Most of these forehead protrusions/asymmetries are well within the limits of safe bone removal (less than 7mms) to create improved forehead symmetry. Most are more in the 3 to 4mm need of reduction. Please send me some pictures for a more qualified answer.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have searched for someone to correct my chin ptosis for the past few years and seeing a slew of negative reviews about the few who specialize in correcting droopy chins has been frustrating and cause for my apprehension. I felt as if plastic surgeons in general didn’t listen to their pts well, but it’s clear now that your advice was sound. Could you please consider discussing possible surgery soon. I have the time to have a submental tuck and / or whichever other procedure you recommend, whenever you have availability . Thanks for your consideration
A: Just to be clear it is critically important for you to understand the differences between a type 1 and type 2 chin ptosis correction, both of which you have concurrently shown in prior pictures when trying to illustrate your desired result. In a type 1 chin ptosis correction the goal is to fix the overhanging tissue by lifting up the soft tissue chin pad into a higher position. This is a tissue relocation procedure which is done through an intraoral muscle/chin pad suspension. The success of this procedure is not great unless it is combined with a chin implant which helps support the lifted chin pad. In a type 2 chin ptosis correction the chin pad position remains the same but tissue is removed from the bottom. This is a tissue excision procedure which vertically shortens the chin a bit which is highly successful IF the diagnosis is hanging tissue off the bone.
Your prior pictures, which are attached, seem to show different types of soft tissue chin pad eshaping goals.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, is there a safe surgical method to correct frontal bossing of the forehead? I have read online on some medical websites that there is no surgical fix but on Dr. Eppley’s website I noticed there were a few photos. My son is 21 and is experiencing some hair loss already in his hairline which exposes his forehead more and we are looking at hair transplant surgery which may help, however I wondered if there was a surgical repair that could safely be done and what that may entail. Thank you for any information you can provide.
A:Bony forehead reduction (frontal bossing reduction)can be performed in anyone. The question is not whether the forehead bossing can be reduced but by how much and whether that amount would be satisfactory to the patient. That I can not tell you without seeing pictures of the forehead in profile and ultimately a side x-ray of the forehead to measure the bone thickness of the outer cortical table. Like any type of skull reductions there are limits as to how much bone can be safely removed. So whatever amount can be removed, even if it falls short of the patient’s ideal goal, is the result a patient has to accept. Thus it becomes important to have a good idea before surgery as to what can be achieved.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had jaw angle implants two months ago and the left side has been swollen ever since. I now seem to have a parotid gland leak on the left side that stems from the frontal edge of the jaw angle implant that may or may not also be an infection. I am fairly sure it is a parotid leak because it has swelled up twice painfully upon eating spicy food. The first time the swelling lasted almost two months, and this time happened again just a day ago. If I remove the implant on the left side, will this be resolved? Will I need a drain, etc.?
A:I have never seen a parotid gland leak from jaw angle implant surgery nor can I imagine how that would be possible since the mandibular vestibule and/or ascending ramus is positioned much lower than the parotid duct. I can only assume that the chronic swelling on the left side causes some partial obstruction of the parotid gland when highly simulated. This is ductal obstruction not a gland leak. It would be anticipated that that thighs will remove when the implant and its associated swelling resolves.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m a young male. My head is convex at the out direction near my ears. I’ve always been self conscious about the width of my head. If you injected Botox into the muscle would it affect the temple muscle on the side and shrink that. I have seen pictures of people getting the injection done near the eyes for crows feet with deep impressions on their face after associated with temporal wasting.
These are photos of what I’m looking for before and after. I’d like to shrink it 5-7mm. Thats what this photo shows. In my opinion its a big difference.
I’m not big on plastic surgery. this is more of a self conscious thing. I’m not interested in excision of the muscle. Is this something you’ve done before with botox and had success before. Do I need an X-ray before determining if its possible. And would you be able to promise something like this doesn’t happen. This person got injections near the eyebrow for crows feet and the temporal muscle shrank that it gave this indentation. Thanks, hope to hear from you soon.
A: Thank you for your inquiry and sending your desired result. That type of side of the head width reduction is only achievable by removal of the posterior temporal muscle which is 5mm to 7mms thick in most Caucasians. Botox injections will not create that amount of shrinkage no matter what dosage is used as the temporal muscle is bog and thick. And even if it did, it will last less than three months after the injections. Botox does not cause permanent atrophy of the masticatory muscles. I have never seen anterior temporal wasting with crow’s feet Botox injections or any form of posterior temporal muscle reduction surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, my question to you is if you could diagnose my head shape. I am having issues with understanding what the condition is it’s either deformational plagiocephaly or lamboid craniosynostosis. They look very similar but I don’t know which one it is. It could be possibly be something else but I don’t know so if you could help me out with this issue I would be truly grateful.
A: Only a 3D CT scan can separate those potential diagnoses for the flat back of your head. It will show whether the lambdoid sutures are open or closed which will provide the diagnosis. Statistically speaking it is far more likely it is deformational plagiocephaly than lambdoid craniosynostosis which is much more uncommon and would present with more severe flattening.
Dr. Barry Eppley
Indianapolis, Indiana