Your Questions
Your Questions
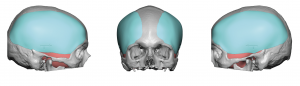
Q: Dr. Eppley, I am a young male seeking help and guidance about my skull shape. I am concerned about the top portion of my skull, it looks like i have a ridge / bump on the sagittal structure. I was never aware of my skull shape until i recently shaved my head due to some thinning and balding. This makes me concerned about my appearance, and i was hoping you could take a look at the attached photos and if you could recognize sagittal ridge and i would like to know if bone burring would be a effective way to reduce this.
A: Thank you for your inquiry and sending your pictures. I don’t think you have a true sagittal ridge and this is just the way your head is shaped which is a bit more peaked. (see attached) But that does not mean that out can not be reduced as normal sagittal ridge bone is adequately thick to do so. The key question is whether such reduction is enough to make you feel better about its shape. (see attached)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Ok with Botox, in some instances it can cause poisoning and permanent nerve damage. I think if we use a high dose the risk is higher of botox spreading to other parts in the face. If you remove part of the muscle, what % of the muscle are you removing. Is it 10%, 50%? Has any of your patients(younger and older), experienced any chewing problems. Can chewing issues develop?
A:In answer to your questions:
1) Every drug has a known LED. (lethal effective dose) For Botox that has been shown in laboratory animals to be around 35,000units of extrapolated to humans by weight. So a few hundred units injected into a human is not going to cause any of the symptoms to which you describe. (poisoning or permanent nerve damage)
2) I assume you are referring to the posterior temporal region which is the only temporal region where muscle can be technically and aesthetically safely removed. Typically 100% of the muscle is removed to get the maximal effect which is what many male patients need/desire. But there is a technique for subtotal reduction where about 50% of the muscle mass is left.
3) No patient will complete temporal muscle reduction ever experienced any masticatory (chewing) dysfunction….nor would I expect them to.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had class 3 orthognathic surgery when I was a teenager – my lower jaw was moved backward and my upper jaw was moved forward. A sliding genioplasty was also performed at the same time. I’ve since fully recovered. I suspect this may have left me with excess fat deposits under the neck which could be removed. I also suspect I never had a particularly well developed lower jaw to begin with. My questions are:
– Do you have experience with lower face surgery on prior orthognathic patients?
– I suspect the visual change, at lease in profile, from improving the neck/jaw angle would be significant. Is it possible/advisable to try to project this along with additional procedure(s) (e.g. jaw implants)?
A:Thank you for your inquiry, sending your pictures and detailing your objectives. I have done lots of orthognathic surgery in my career but have undoubtably have done more post-orthognathic surgery jawline reconstructions and aesthetic jawline augmentations. Orthognathic surgery is a functional occlusal operation that can have some aesthetic benefits as well but which are relegated primarily to the sagittal plane. (side view) I have seen many after orthognthaic surgery patients with altered jawlines from sagittal splits and sliding genioplasties as well as jawlines that lack definition and width particularly. While I haven’t seen your 3D x-rays, what counts is the objective to which I have attached one version of an overall jawline/neck change as a starting point for discussion.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello,I’m inquiring about a service you offer. Since I was young I’ve had a dented skull which is pretty largely visible but I manage to hide it fairly well & it’s not really noticed ever. But I will foresee the need the surgery one day if I ever go bald lol, so I’m inquiring on cost for this services? I’d say it’s a good 3/8 inch dip with 2 inch circular diameter.
I would love to get this handled one day but I just don’t have thousands & thousands to fix it. But hoping if price is right that I can go in a correct this.
A:Thank you for your skull dent inquiry and detailing your head shape concerns. But your description that is a fairly small skull indentation (roughly 5 x 5 x 1cms) which could be filled in with different types of materials and, if one is able, could even be done under local anesthesia or IV sedation. The most economical material would be PMMA bone cement. While many skull augmentations and defects are done today using custom made implants that adds considerably to the cost. PMMA bone cements is how I used to do all skull onlays so it may an older technique but still effective.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley: I would like to ask several things in detail.
I also uploaded my pictures and CT of my head and picture of head of female that I want to have.
First, second and third file uploaded are pictures of my head
And fourth and fifth file is pictures of female’s head that i want to have.
Please see my head pictures and the pictures of a female and give me exact answer about whether the surgery can make me satisfied.
1. Safety and problem of thinner skull after the surgery really matter sir. I heard from many korean plastic surgeons who have Ph.D in plastic surgery said that head reduction is dangerous and there is no way to do that.
I have never seen korean plastic surgeon who perform skull reduction surgery.
So I would like to know how and why it is safe.
And as far as I learn through your website it burs or remove the bone of the head which surrounds and protects a brain.
I really wonder whether this surgery makes skull much thinner weaker and lower the protectional function of the skull from outside physical attack.
And I would like to know whether when it fails it leaves permanent injury or brain damage.
2. I think to have a much smaller head, temporal, occipital and sagittal reduction in terms of skull reduction to make a female head that I really wants. Please let me know whether the head that I want to achieve is possible by the surgery or not, by objectively considering the female head of the pictures that I uploaded
3. How much the head reduction is possible on sagitally occipitally and temporarily in mm scale?
4. What is a total cost of surgery that includes everything from surgery cost, hospitalization cost to any other cost that i need to pay.
Thanks. I would like to recieve the answers as soon as possible.
A:Thank you for your skull reduction inquiry and sending your pictures to which I can reply:
1) Your questions about the safety of skull reshaping surgery are common and understandable. A surgeon who has never done this type of craniofacial surgery can not truly speak for its safety and/or effectiveness but I can. Others may have an opinion but I have extensive experience in actually doing it. Removing the outer cortical layer of the skull does not weaken it in any appreciable way as that is about 1/3 to 1/2 of the total skull’s thickness. The issue is not one of safety but of how effective it can be in terms of the patient’s aesthetic objectives.
2) The critical question in every skull reduction patient is whether it will be effective enough. Just looking at your picture and an ideal female head example does not really tell me much. Both have hair which masks the actually head shape so this information alone doesn’t help much.
3) Without seeing a 3D CT scan of your skull and making measurements (you have only attached a 3D face CT image) I can not say where and how much of the skull bone can be reduced. Temporal reduction is the easiest to comment on because in that skull area it is the muscle that is reduced which creates the most dramatic change. (posterior temporal muscle is removed and the anterior muscle thinned which produces reductions of at least 5 to 7mms per side)
4) Whether total skull reduction would be effective injections your case I can not yet say. It would take a 3D skull CT and then comparing it to a 3D CT scan of a Korean female to best answer that question.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am based in Canada and my background is Indian. I have thick skin and my original nose was wide AND long! I’ve had 3 surgeries (Primary in India and two revisions in Canada) but the result is still bulby looking, the tip still long. I was wondering if you are comfortable operating on patients with thick skin, and with previous surgeries. (revision rhinoplasty)
A: Thank you for your inquiry and detailing your rhinoplasty surgery history. The question is to whether any surgeon (myself or anyone else) feels comfortable performing revisional rhinoplasty surgery but whether they feel they can make a difference and justify the putting the patient through a 4th rhinoplasty. Admittedly a thick skinned nose that has had 3 rhinoplasties, all in an effort to make it shorter and thinner but without great success, does not bode well for any further surgery finally making the ‘big difference’. But that basic issue aside, I could provide a more qualified opinion by seeing some nose pictures, and as best as you can recall, having some information as to what did they do in the last two surgeries to try and make it better?
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello and how are you? I am emailing you as suggested by Camille with my inquires and photos. First let me begin with the background. Overall, I am happy with my face and think I am approaching this from a decent baseline but I was wondering if it is possible to enhance it with a change that can still be subtle. I am seeking the chiseled jaw look. Although I am a male, I was inspired Angelina Jolie’s chin projection jawline very much (although she may had other work done along with a low percent body fat). I am wondering if chin and jaw implants (specifically the jaw implant that emphasizes a stronger angle as opposed to increased width) or wrap around implant would give me my desired look. My concerns is having a swollen face look even after the healing has completed or having a drastic change. One thing to note myself is that I had fillers placed, my last round was over a year ago in the chin and jaw lines, hopefully this won’t be an impediment to your assessment. Below is a list of questions along with a video. Also note, there is a picture from the RealSelf website of a prior patient. I put it up there because it is one of those cases where the before or after is too drastic!-hence my desire for subtlety. Any feedback is greatly appreciated!
1 I am scared about nerve damage, can you comment on that, particularly your success rate and experience with this? -especially if the implant is a wrap around.
2 I am also scared about the swelling and realizing it will take months for it to get back to normal only to see that my new face is a swollen look. How common is that concern, how do you counsel?
3 Is it possible for changes I desire to be achieved yet subtle so it’s not obvious to others or does that defeat the point?
4 Is it possible for computer imaging to show what I will look like after the implants?
5 I am also physically active, I assume I won’t be able to lift weight six to eight weeks after? or would it be longer?
6 How often are people not satisfied with their result and thus request a removal? Does their face go back to normal?
7 Roughly how much could this cost (i.e what is the most expensive this could be?)
8 I live in NYC, thus this impact your practice given COVID, also how long would I have to stay and how soon could I go back home?
9 I also suffer from psoriasis and on an immunomodulator suppressive therapy, thus does that play into any factor? Do people immunologically react to the implants? Can all the incisions may be intraorally only?
10 Do people feel the implant ?
11 Does having some filler in the face complicate the surgery?
12 Also you will see in the video that my face gives ME the impression that I have a fatty chin when I have been told that is not true, would implants incidentally ease the appearance?
Thank you Dr. Eppley,
A: In answer to your custom jawline implant augmentationquestions:
1) The only nerve of any relevance is the mental nerve which controls feeling of the lower lip. This implant is passed under that nerve which can cause some short term temporary numbness in a few small cases but not permanent loss of feeling.
2) While the swelling can be considerable from a patient’s perspective most of the significant swelling is but a few weeks (2 to 3 weeks) where one may feel a bit distorted. I can say that I ever recall a patient months down the road that ever look ‘bloated or just had a fat face as implants expand the tissue. But it is true that thinner faces always end up with more defined results with smaller sized implants.
3) Your question is based on the common misconception that other people are a lot more observant than they really are. Just because you know you had a jawline implant doesn’t mean other people can even tell almost regardless of the magnitude of change for two very specific reasons…1) people can only recognize plastic surgery procedures that they know exist (99.9% of the world would never believe a total jawline augmentation change is even possible) and 2) everyone is a lot more concerned about themselves than about you. They are a lot more worried about themselves not looking right or looking good most of the day than they are perceiving any change you may have done.
4) It is a requirement than every facial reshaping patient undergoes computer imaging. But your perception of the role of computer imaging in facial surgery, which is common, is inaccurate. Computer imaging is about setting the target…what is the patient’s goal? As the old motto goes one can not hit a target they do not have. I have no preconceived notion of what type of change you want and frankly I don’t care what your jawline augmentation goal is. I only care about what you want so I can strive to achieve it. That is the real purpose of computer imaging. We may or may not hit the target exactly but we have a much better chance if I know what it is. Such a philosophy takes on the greatest relevance in custom facial implant surgery where the creation of specific implant dimensions are required.
5) Your assumption in regards to working out/weight lifting is inaccurate. You can do any of these activities when you feel comfortable to do so. Such activities will not displace the implant nor interfere with its healing.
6) Almost no one ever requests a removal. They may want it revised bit almost never just removed.
8) Other than requiring patients to have a negative COVID test before surgery, there are other unusual preoperative requirements. The goal is to get the patient home asap, usually within a few days. There is no advantage or need to remain here. You want to get home to recover on familiar ground.
9) The would depend on what type of immunosuppression you are on. But I can assume since the treatment is for psoriasis that it is a more contemporary drug regimen as opposed to prednisone etc. Implants do not evoke an immunologic reaction and no one develops an immune reaction to the implant materials. Implants can get infected which is often confused with being ‘rejected’ or developing an ‘immune reaction’. I rarely place jawline implants through an exclusive intraoral approach since that has a higher rate of infections. While the back incisions are placed inside the mouth, the front incision is placed under the chin.
10) No more than you can feel your own jawbone now.
11) The location of synthetic fillers is irrelevant in regards to both designing an implant or surgically placing it.
12) I would defer to computer imaging to visually answer the question as to what will happen to your ‘fatty chin’.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Thank you for your reply and your feedback about the photos! And i think you are right that I do not have a true sagittal ridge but it looks a bit more elevated at the sagittal structure. But it still affects me negatively, and I am still interested in the surgery. In order to be more informed about the sagittal ridge bone burring procedure, i would like to ask you 2 questions.
1. Is it necessary for me to make a CT scan of my skull in order to determine if it is possible to perform the surgery?
2. Will there be a visible scar left on my head when the procedure is done? (I assume, yes)
Thanks in advance!
A: 1) The only reason to ever get a CT scan (2D CT scan, no contrast) on a midline sagittal elevation is to determine if enough bone can be safely reduced to make a difference. In other words one wants to make the elevation is due to thicker bone not because the underlying bone has gotten thinner. While I have never seen such a situation in which the bone is too thin to operate it is always better to be ‘safe’/certain.
2) There will be a fine line scar about 4 cms in length but such scalp scars usually heals so well there has yet to be a resultant scar in a primary procedure that a patient felt was problematic. (request for scar revision)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have eye asymmetry. I have had it since i was young. What can be done for it? I have attached pictures for you review.
A: Thank you for your inquiry and sending all of your pictures. Your eye asymmetry is due to a well known condition of VOD. (vertical orbital dystopia) The orbital box (bones that surrounds the eyes) is lower on the one side by 3 to 4mms. This is evidenced not only by the horizontal level of the eyes being different but also by the eyebrows that its lower on that side as well as the slightly flatter cheek in that side as well.
To understand how VOD is surgically treated I would refer you to one of my websites, www.exploreplasticsurgery.com and search under Vertical Orbital Dystopia where you can read and see how that is done.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, my issue is mainly the posterior part of the temporal muscle. I looked it up and it was stated online that the posterior muscle is responsible for moving the jaw forward and back. I have three questions:
1) Is it possible to remove 50% of the posterior muscle, cut it in half so that it goes from being 7mm to 3.5mm. I don’t want to use the word shave it down, but slice it down the middle.
2.) Are there any complications at all even from removing a portion of the posterior muscle and not the whole thing? I’m not looking to have a flat side of the hea. I’d still like there to be some curve, I just think there’s a high risk if we go down the Botox route of the units shifting to other parts of the face.
3.) Would I be able to talk to a few other male patients who had this procedure, before I commit to having it.
My main fear is having something permanent that causes functional problem because muscles do shrink with age. How will my temporal muscle fair up when I turn 80?
A: In answer to your posterior temporal reduction surgery questions:
1) Muscle is not like bone, there is no shaving of it particularly from a remote incisional access. As I said earlier a portion of the muscle can be removed through a release and rotational maneuver to keep some of the muscle thickness.
2) Regardless of what any anatomic textbooks say the entire posterior belly of the temporal muscle can be removed without any functional sequelae on mouth opening and closing. I would know after over 100 posterior temporal muscles removed and no patients has ever even had temporary mouth opening stiffness. That is because 70% of the temporal muscle lines anterior and the posterior part makes up a small percentage of the muscle despite its apparent large surface area coverage.
3) Botox does not shift to other parts of the face. It has a well known intramuscular diffusion range of only 1 to 1.5cms from the injection site.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a board certified plastic surgeon. I recently had a patient requesting an skin excision from her elbow. (elbow lift) I had never heard of that procedure and did not even realize one existed. I saw that you have indeed done this procedure. I was wondering if you have any pics of the scars many months out? I would be so grateful if you could share any advice on this procedure.
A: Like all tissue excisional/tightenng body procedures, and elbow lifts are no exception, it is all about whether the scar is a worthy tradeoff. Forget about whether the scar is good looking as that is the hope but there is no guarantee across a moveable joint. Paint the picture of an adverse scar that will require revision (I have only done one such revision in more than 20 elbow lifts….but that is not the point) and then see if they want to do the procedure. The best candidate for any aesthetic procedure where the scar is unpredictable is when they tell you quickly and upfront after the scar discussion that they would rather have a scar than loose skin. Any wavering about the scar disqualifies them from the surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am looking for a plastic surgeon that can remove a skin graft that took place due to a car accident where I had a scalp flap rotated forwarded to replace forehead tissue and a skin graft put in place behind the rotated flap. This took place when I was very young. The graft is thin as no tissue underneath so tends to get injured easily if bumped and doesn’t heal well as well as disfiguring now with hair loss. The graft is approximately 6 inches long by 2 inches wide with the 6 inches going left to right on my head and the two inches front to back of head. Do you perhaps a procedure such as the Extended Scalp Reduction or other techniques in place now that were not available when the accident happened? Thanks for the response.
A: The question you are asking is whether a scalp skin graft site can be excised and primarily closed….without a flap and creating a tissue deficient somewhere which requires skin graft coverage. (which is what you have already had done many years ago) If you had not had prior surgery a scalp tissue defect of 6 x 2 inches might be able to be excised and primarily closed. But with prior surgery and loss of 1/2 of the scalp’s ability to stretch due to the previous flap, that is much more in question. Using tissue expansion of half of the scalp that has not previously operated on, it is undoubtably possible. That raises the next question of whether it is possible without tissue expansion. To provide a more qualified answer I would need to see pictures of your scalp and the skin graft site.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I plan to fly out this summer and set up an appointment with you. I’ve read numerous studies and doctors have been able to reduce the temples by 4-5 mm with Botox injections.Yes your right, multiple injection rounds are needed every 3-6 months. But I’m willing to pay and fly out to you every 3-6 months. Is there anyway we can run scans at your office and formulate a plan with Botox. I’m not interested in excision of the muscle under any circumstances. If its impossible to achieve the temporal reduction results as you illustrated with Botox, please tell me up front, but I’d rather fly out every 3-6 months to achieve reversible results. Have you ever reduced the temporal muscle with Botox injections?
A: There is no question that Botox can shrink a masticatory muscle. But like all drugs its effect is dose dependent. And the temporalis is an enormous muscle that would require very high doses (in comparison for example to the masseter muscle) to see a substantive effect.(of which 4 to 5mms would count as substantive) What dose that is per side can not be fully predicted beforehand and the dose:effect ratio per patient can only be learned by doing it. (pick a dose, see the effect and adjust accordingly next time) There is no scan or imaging that is going to be helpful when injecting Botox into any muscle as long as the target muscle location is known.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Looking through the internet about “chin ptosis” (I just find out this is the medical name) I found a blog in which you provided some valid points and and your views on patients with the same “issue” that I have. I had no idea that I was not alone about this, usually I always hear about “chin enhancements” such as implants or fillers to make it prominent but never to make it smaller or “reduction”, so I was very happy when I read about it and find out about you. Im still not sure what procedure would be best for my unique case because it seems that the bone in my chin is way short, and the “pointy” or “prominence” comes from a “fatty ball” that is seating on the bone, I am aware that I need probably an x-ray, but what kind of x-ray should I request? Do I need a prescription? Or this is something that its include on the examination? Or maybe a referral? I have many questions, concerns and doubts that I’m sure it could resolve with an initial consultation. Please I will be so happy to hear from you soon.
A: Thank you for your inquiry and sending your pictures. The one simple x-ray that shows best the relationship of the chin bone to the overlying soft tissues is a lateral cephalometric x-ray. This is a very common x-ray done in any orthodontists office. Whether the bone has any contribution to the appearance of your chin and the thickness of the overlying soft tissue pad of the chin will be revealed in this classic lateral facial x-ray. That piece of information will be critical for our virtual consultation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Can you perform hip implant and butt implant surgery at the same time?
A: It is technically possible to perform buttock and hip implants at the same time…but that makes for a difficult recovery. I have had numerous patients go through this combo body contouring/augmentation surgery but they will tell you it was rough and it comes with increased risks of complications. (four implants and notes two) The other caveat is that the buttock implants have to be intramuscular if hip implants are concurrently performed or eyen in the future to keep the tissue pockets from merging.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had posterior temporal reduction surgery by muscle removal three months ago and am very pleased with the result. My question now is what can be done for the anterior temporal muscle closer to my eye.
A: Based on your email previously and the current one, I assume the remaining issue is the front part of the side of the head, the anterior temporal region. The anterior temporal region is different from the posterior in that the muscle can not just be removed like the posterior temporal region. That would cause contour deformities as well as potential jaw opening/closing problems. Thus the anterior temporal fullness must be treated differently. Options include non-surgical (Botox injections…very effective but not assured of permanency)) and open electrocautery surgery which causes permanent muscle shrinkage due to the thermal injury of the outer muscle fibers. Botox injections take weeks to see their effects while electocautery can take up to three months after the surgery to see the full effects of muscle thickness reduction.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had 300ccs of Aaquafil injection into my hips last year. I am interested now in getting hip implants for more volume. Is it safe to do so after these injections?
A: Aquafil is an injectable filler that is composed of 97% saline and 3% polyamidized hydrophilic gel. (It is not FDA-approved in the US) It is a filler that is allegedly absorbed but can take up to five years or more to do so. While a 300cc injection is really about 30 cc of the actual gel material (or less) the actual amount of material there is relatively small. But it primarily works by inducing a lot of scar tissue reaction around it. BUT with the high rate of seromas (fluid collections) in hip implants anything that could increase that risk gives one pause.
It is hard to say for certain that it would or would not be a problem knowing the total volume injected. But given that this is elective surgery is always wise to limit risks when possible. Certainly the safest course is to not proceed with the hip implants for now and await one day when one is more certain that the filler has gone away….or at least there s less of it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in custom pectoral implants.I’m 6’ 3” and anywhere from 220 to 250lbs so the 900cc custom pectoral implants would work. Is my silicone that was injected in my chest an issue? I am also planning on having shoulder surgery soon, is that an issue? Ideally I’d like to get the surgery not so far after the shoulder surgery so that I’m not going through tons of “down time” but I don’t know if that’s a possibility.
Thank you
A: In answer to your custom pectoral implants questions:
1) I assume that the silicone injections were either placed into the chest soft tissues above the muscle or into the muscle itself. Pectoral implants are placed under the muscle which presumably is out of the zone of the silicone injections….with the operative word ‘presumably’. Do you know what volume of silicone was injected, how many injections and how long ago?
2) Pectoral implants can be done after shoulder surgery. (or before) The critical question is how long after the shoulder surgery. That would depend on what your shoulder surgeon says is advisable as we have to put your arms out to 60 degrees from your body during surgery. Whenever he/she says it is safe to do so would be the guiding principle for the timing of the surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am concerned about long term infection with a Medpor chin implant. I had a medpor chin implant placed one year ago and I’m worried about the infection possibility of the implant. Is it beneficial to switch this into a silicone implant now?
A: By your description you have an existing Medpor chin implant but without any previous or current signs of infection. If it has been one year since its placement and you have never yet had an infection, I would just leave to alone if it is aesthetically satisfying. The risk of any implant infection is almost exclusively in the perioperative period. (first three months) Once past that time period the risk of infection is so low that it is not worth removing and switching it to any other implant material.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My son is 5 years old and was born with scalp aplasia cutis congenita. Around 3 x3 xm on the scalp. The dermatologists does not wish to help us correct this until my son has a say on this when he is older which I think is ridiculous as a parent.
A: Thank you for your inquiry. Congenital scalp cutis aplasia areas can be excised at any age. The real question is not whether it can be excised but whether it can be primarily closed without undue tension or excessively long incisions from scalp rotational flaps. Scalp surgery in a growing head is interesting in that scars do expand with growth so many of these scalp surgeries require further surgery in the future for scar widening from the expansion of skull growth. But certainly it can be substantially reduced. I would need to see some pictures of it for further assessment.
Some cutis aplasias have either very thin skull bone underneath them or rarely I have seen them with areas of missing skull bone underneath them. But I assume that the latter is not evident in your son’s case.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Im writing to you because i find your work amazing! I want to do several aesthetics procedures with you. But i have a big big problem, who makes me sad everyday…..
I would like to find a definitive solution for my shoulder. I have a skin congenital atrophy yon my shoulder. (lack of fat?? or I don’t know I was born like this). It looks like a crater. I was looking for doing PMMA injections on it as I have already had multiple fat injections and they didnt work.
It would be my biggest dream to find a permanent solution, without thinking about doing several injections, or taking care or my weight for not loosing graft, or be able to use my shoulder.
Is that possible for you, to customized an implant for me? To fill the hole? Like this it would be definitive! I found a doctor in China but I have seen your work and it would be amazing if you can help me.
Thank you in advance doctor!!!
Have a very nice day!!
A: Thank you for your inquiry and sending your pictures. That shoulder appears to have a congenital subcutaneous atrophy/dermal thinning. While injection fat grafting would be the obvious solution, having failed that numerous times it is time to try something else. While the implantation of ‘something’ would be the correct alternative, and one could use an implant (ultrasoft thin sheet of perforated silicone), I would think first about an allogeneic dermal graft. (e.g., Alloderm) This very pliable sheet of 2mm dermis would act like an implant from a fill standpoint but it would be incorporated into your tissues which I think is better long-term in such a high motion area.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am 21 years old and I have plagiocephaly which has never been treated. The cranial malformation does not bother me but the asymmetry of my face is really showy and ruins my life, I am in depression because of this, I have no social life. I send you photos of my case, hoping that there are solutions. Thank you for taking the time to read me.
A: Thank you for your inquiry and sending your picture. You have a left facial asymmetry that is complete, meaning it extends from the forehead down to the jawline, and the entire side of your face is shorter vertically than the other side. You have an inferior-based facial asymmetry which means it affects most the inferior part of the face (jawline) and becomes less severe as one heads further up on the face.
Like all complete facial asymmetries the patient has to prioritize the facial features that are most important to improve or will create the biggest difference. Technically a complete facial asymmetry surgery involves an endoscopic browlift (to raise the lower eyebrow), vertical orbital dystopia correction (raise up the eye), cheek augmentation, nostril repositioning, mouth corner lowering and chin/jawline augmentation. From your viewpoint what asymmetric facial features bother you the most?
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello there, I’ve been looking for someone that could offer skull reshaping surgery for years and have just discovered you! I suffer from scaphocephaly, its bothered me for years to the point where, now at 28 years old, I need to do something about it. I understand I probably wouldn’t achieve a normal head shape, but anything to improve the overall look would make such a difference to my self esteem.
How much would this cost roughly?
A: Thank you for your inquiry and sending your pictures. In the scaphocephalic skull it is long from front to back and narrow on the sides. With your hair and the angle of these pictures all I can appreciate is the narrow forehead/temporal areas outside of the hair zone in the front. Please tell me what would be the significant part of it to change from your standpoint so I can devise a skull reshaping surgery to do so. Once I know exactly what needs to be done then my assistant can pass along the cost of the surgery to you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I underwent otoplasty nearly 30 years ago and and the results were very average. In my opinion, the tips of my ears were pulled back too far and now appear very flat if not contorted. I have tolerated it for this long, but now my hair is starting to thin I’m becoming more conscious of it.
Aside from traditional cut and stitch, are there any other methods available now that could achieve a more ‘natural’ look? I’m a bit wary about going under the knife again.
A: Any attempt at trying to shape your ears as an adult requires surgery. There are no non-surgical efforts to do so. That is only done right after birth when the east cartilages are moldable by external means. But that ear reshaping capability is lost months after birth. I would need to see pictures of our ears to provide any surgical insight.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a 9mm medpor chin implant placed last year from a submental approach which was not secured by the screws. One month after 1 surgery it shifted. Then two small titanium screws from an intraoral approach were placed but it shifted again. Thereafter two larger titanium screws were inserted also from an intraoral approach. Unfortunately, I was eager to have two more large screws after some trauma placed because I feared malposition which was also done.
Thereafter, I developed scar adhesion after triple surgeries in a 6 month period from the intraoral approaches!!! This creates bumps over the implant, and causes me intermittent numbness and lack of mentalis control.
I’m extremely frustrated… I guess it’s pretty hard to remedy. I know you are an expert on chin implants. I was wondering if it’s possible to deal with this situation? Many thanks.
A: As you have aptly stated stated you have developed scar tissue from multiple intraoral entrances through the same incision. Like scar adhesions anywhere on the body they are treated by release and the placement of an interpositional soft tissue graft of which my preference is a autologous dermal fat graft. This will certainly remedy the scar adhesions, where that also improves mentalis muscle function fully can not be predicted beforehand but the two are almost always related to a significant degree.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m still torn on which midface surgery I should undergo.
I can’t tell if I have a recessed or average maxilla, but if that turns out to be the case, will your maxillary implants be able to create a protruding maxilla to the same extent as a lefort II or lefort III procedure? I don’t have an overbite, and according to this test I have an average/slightly receding maxilla.
“1. Make a picture from the side while smiling
2. then compare the sagittal position of your front teeth compared to the nasion (image a vertical line from the nasion – nasion line)
results:
if your teeth are at the same lvl with the nasion line your maxilla is average
if your teeth are beyond the nasion line your maxilla is protruding
if your teeth are behind the nasion line your maxilla is recessed”
Thanks a lot for the help,
A:Thank you for your inquiry and detailing your concerns. With an ‘average to slightly receding maxilla’, regardless of how that is determined you are certainly never going to undergo any form of a LeFort osteotomy advancement unless you have a compelling need to bring your lower jaw forward as well. Modified midface osteotomy designs that leave the occlusion alone are poor substitutes for what a custom midfaceimplant can do because of the magnitude of the surgery and the resultant irregular osteotomy lines and bone contours. Bring the midface out in a smooth and contiguous fashion that is predesigned for the aesthetic effect produces superior results. The only thing that a midface implant can not do is change the occlusion but that is what osteotomies are for which is their primary benefit.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi I’m interested in a more rounded head and temple shape. I feel like my head causes asymmetries to my face structure which is very different from both sides. I also don’t like that it looks like I have a long profile view and asymmetrical view from the front. Let me know what you think.
 A: Thank you for your inquiry and sending all of your pictures I believe you are referring to what many such patients described as a ‘pinched head’ where the sides of the head (bilateral temporal area including the sides of the forehead and back of the head) are too narrow. This is consistent with what I see in our frontal view picture and why you describe a desire to have more round or normal shaped head. I treat this head shape with custom fronto-temporal implants (as per the attached custom skull implant design images) which provides increased head width from front to back. Such implants are placed mainly through an incision begin the ear with a few very small scalp positioning incisions.
A: Thank you for your inquiry and sending all of your pictures I believe you are referring to what many such patients described as a ‘pinched head’ where the sides of the head (bilateral temporal area including the sides of the forehead and back of the head) are too narrow. This is consistent with what I see in our frontal view picture and why you describe a desire to have more round or normal shaped head. I treat this head shape with custom fronto-temporal implants (as per the attached custom skull implant design images) which provides increased head width from front to back. Such implants are placed mainly through an incision begin the ear with a few very small scalp positioning incisions.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to start by thanking you for taking the time to reply my email. I would like to convey how grateful I am for your email. I love how the Vertical Lengthening Chin implant looks on my face. I had a relatively small chin so the s size of the VLC was perfect. It gives my face a longer and sharper look. So thank you so much for designing this. The only problem that I am having so far (I’m on day 4) is that the part where the implant ends (under my chin, close to my neck) is protruding out of my skin and is very apparent, almost as though it’s not sitting on my jawline. I am aware that this may be swelling. Also during surgery, I asked my surgeon to trim the implant if needed, he did not do it as he probably didn’t think it was necessary. I’m worried that these lumps on my neck will remail there. I would really like a smooth jawline. Have any of your patients complained of similar instances? I would like to apologize if my questions are silly. I’ve just been a little stressed out.
Once again, thank you so much for your precious time.
A It is not exactly clear to me what your mean by ‘protruding from my skin…and… not sitting one my jawline’ without any visual or doing your actual chin implant surgery. What I do know about any facial implant ss that the combination of swelling which peaks at day 3 and doesn’t really go down enough to tell much for weeks after surgery freaks out a lot of people early on. My usual statement is ‘this is not instant oatmeal’ and trying to make any assessment now about the result or shape is meaningless since everything is so distorted.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am inquiring about having a bulbous rhinoplasty done and am hoping for a symmetrical, smaller, thinner and narrower nose, including the nostrils. What is the cost? I have also sent 7 pictures.
Thank you
A: Thank you for your inquiry and sending your pictures Like many bulbous nose patient you have thick nasal skin which does provide some limitations as to how much thinner/more narrow your nose can become with rhinoplasty surgery. While I don’t think it is possible to have a substantially smaller or thinner nose, there are improvements that can be made as per the attached prediction imaging. As long as one has a realistic understanding of the limitations of what a rhinoplasty surgery can do in the thick skinned nose patient then surgery can produce a satisfying improvement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi! I haven’t been in for a while…if u remember when I was young I got cheek implants..(somewhere else before I moved here) I fell last week and hit my face hard..my face has been swollen on one side..beside my cheek clear to my nose and down..can my cheek implant bust…I fell Thursday night face is still really swollen clear to my nose…I know its prob just still swollen from fall I hit it really hard…can u ask dr if the implants are hard and wont bust or could implant have busted?
A: Good to hear from you and sorry to hear of your fall. Almost all cheeks implants placed since the 1980s have been solid silicone cheek implants which can not bust for break. I don’t know the exact year when your cheek implants were placed, but it is a 99% probability that they are solid. So your face many be swollen but it is highly unlikely that your cheek implants are ‘broken’.
Dr. Barry Eppley
Indianapolis, Indiana