Your Questions
Your Questions
Q: Dr. Eppley, I had a sliding genioplasty two years ago and 5 days post op, the Doctor asked if I feel numb esp on the left side of my lower lip/chin and I said yes. He said it’ll be gone in 6 weeks or it’ll take years. I waited but 2.5 years after, I still have numbness on the left side of my lower lip. I am experiencing tightness and weird sensation on the area. I now have a crooked smile and I can feel it get tighter when I talk. Is this nerve damage, impingement or muscle weakness? Should I do a revision or remove screws?
A: At this prolonged time after sliding genioplasty surgery the left mental nerve numbness can be assumed to be permanent. Removing the plate and screws will not make any difference in the numbness as they are located far from the mental foramen. Persistent tightness may be improved by release and placement of a fat graft.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a long midface. The length from the eye to the end of my nose is too long. I didn’t found a surgeon who can reduce the Part of my midface. I wanted to know is it possible to reduce the bone of my midface from the eye to the nose? And if it is possible who much is the average price. Thank you for your time and help.
A: You are asking for a midface procedure that does not exist. While the midface bone can be shortened that will change nothing on the outside. The only two midface soft tissue ‘shortening’ procedures are rhinoplasty and lip lifts. There are no midface narrowing procedures between the eye and the nose.
Dr. Barry Eppley
Indianapolis Indiana
Q: Dr. Eppley, I suffer from a condition known as occipital deformational plagiocephaly. I’ve seen that you have significant experience in the correction of this issue through a variety of different methodologies.
Unfortunately, I reside in Canada. Do you conduct procedures on individuals who travel across the border? If not, would it be possible for you to point me to a Canadian surgeon who has experience in correcting this issue?
A: A significant part of my practice are patients who do not live here. Most occipital plagiocephaly skull deformities are treated by building up the deficient side with a custom skull implant made from the patient’s 3D CT scan. I would assume based on your description that the same would apply to you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a weak chin and a jawline that while pronounced, is also quite steep. I had spoken with you through video consult previously in regards to a custom wrap around jaw/chin implant to fix my jawline along with a buccal lipectomy and perioral lipo to rid myself of genetic chubby cheeks.
My question is would the wrap around jaw implant alone make my face look chubbier than it already is or would it stretch out may face enough to where I do not have to worry as much about fat removal?
A: The tissue recruitment effect that a custom wrap around jawline implant has comes from the neck and not the face. Thus I would not expect a cheek reduction effect to occur as a result of it. But there is always one way to be certain of that effect…do the jawline augmentation first and see how you feel about the cheeks afterwards.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Can I fax your office operative notes to get your opinion on how complex my otoplasty reversal would be. Please
A:While I am happy to read the prior surgeon’s operative notes, and more information is never a negative, any form of otoplasty reversal comes down to the same two principles…..adequate cartilage/soft tissue release and an interpositional cartilage graft to hold it. These same two intraoperative techniques must be done regardless of how the ears were pinned back.
Dr. Barry Eppley
Indianapolis, Indiana
Q:Dr. Eppley, I would like to know what procedures/implants are required to achieved hollow cheek like those male models. I know body fat plays a big role but besides that if any implant is needed about how much mm is needed?
A: You are correct in that one needs to have very little facial fat to achieve that hollow cheek look. But when it comes to midface implants achieving that look it is far more about the implant’s shape and surface area coverage than it is about millimeter’s of implant thickness.
Dr. Barry Eppley
Indianapolis, Indiana
Q:Dr. Eppley, I have a question about skull reshaping. In the attached pictures you can see I have two bulges on my forehead, while the one on the right is more prominent than the left one. I think it is bone, as I had this head shape since I was a young boy, but the bulges seemed to grow more throughout puberty. I’m now 22 years old and guess, that they won’t grow much further. Anyways they really disturb me and I don’t feel comfortable with them being so large.
Do you think this is something you can correct?
A: Thank you for your inquiry and sending your pictures. You have the classic forehead horns of which your history of them is also classic….grew bigger after puberty. Such forehead horns can be completely reduced by burring. Their method of elimination is straightforward and 100% effective. The vexing question, however, is how to get there and not create scarring that might be considered just as aesthetically disturbing as the horns themselves. This is a common issue in males with higher hairlines of indeterminate long term stability. (indirect hairline incisional approach) The direct forehead wrinkle line approach subverts this issue but then one has to ponder how well the wrinkle line scar will do.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was wondering if I would be a good candidate for a buccal lipectomy, perioral liposuction and/or buccinator myectomy. I’m 26, 5″6, and weigh 115 pounds yet my face has always seems bloated because of fat cheeks genetics and probably thick skin. I was hoping that maybe with these 3 procedures would a be a good start to get rid any facial fat and have the more concave look in the mid-face. Thank you for your time.
A: Thank you for your inquiry and sending all of your pictures. Certainly you already have some slight concavity to your midface so I think the three procedures you have mentioned would go a long way in helping you maximize that potential type of facial change. The other procedure that you didn’t mention which will really help is a chin augmentation, particularly a sliding genioplasty. As the chin bone moves forward that helps provide an upper facial slimming effect as well. This would also helps your facial proportions as lower third is smaller compared to your larger cheekbone structure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am looking to have facial surgery. I know I definitely want rhinoplasty, but I also want to look similar to a particular celebrity. I have attached pictures and would love to know what you think changes can be done. The first pictures are me, and the other pictures are Saweetie. The picture of her in the black blazer is the nose that I want. I hope to hear from you soon!
A: Thank you for your inquiry and sending all of your pictures. While I think it is good to have a very specific goal it is always fair to say one can never be made to look exactly like someone else’s facial feature. I do not consider your goal wildly unrealistic but in rhinoplasty it is all about how the skin will shrink down around the reshaped bone and cartilage framework. Thicker nasal skin is more unpredictable in that regard.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Thank you so much for the quick response. I can have the previous surgeon send my records, as I’m confident that he didn’t reduce the size of the extended wings of my Medpor chin implant, and only the main portion of the chin.
If that’s the case, I’d prefer to just have the wings altered since I’m happy with the rest and really want to avoid a complicated/risky procedure.
Please let me know if that’s an option. I hope it is, as I’m terrified to have another procedure and will likely only pursue a mild alteration than an entirely new implant.
A: What I am trying to say is that with a Medpor chin implant you can’t just trim the wings in place. The tissue ingrowth that this material creates makes that very difficult and dangerous to the branch of the facial nerve which crosses over the tissue right above the implant. It has to be completely extracted to safely do so. And getting it out will likely result in it being removed in pieces. This is the downside to have an implant that has vigorous tissue ingrowth. It is only great if you never need to modify or remove it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I underwent a cosmetic surgical procedure roughly 2 months ago. It was a forehead contouring surgery to reduce the prominence of my forehead and eliminate the “bony horns” to give it a smoother and less bulging appearance. Since I am a male, it was decided to go with a bicoronal incision from ear to ear instead of a hairline incision just in case if I experience a receding hairline down the road. They used the trichophytic suturing technique so that way my hair can grow back through the incisions and it would be virtually unnoticeable. Well, as I stated it’s been about 2 months and there are still patches of the scar where I see no or very limited hair growth and when you look at my head from the side, you can see a clear line in my hair where the scar is. I attached some pictures and was wondering if you can give me some feed back and tell me what you think.
A: I am not exactly sure what commentary you are seeking. To perform that forehead procedure I would have never used a bicoronal incision in a male as that is exactly the scar outcome I would have expected. Bicoronal incisions notoriously become visible in the temporal regions no matter what technique is used to close them. They do much better across the top of the head between the temporal lines but always widen below that line on the sides of the head. (and hair is not going to grow through the scar) That is why a much more anteriorly based scalp incision that does not go below that line is always a better scar risk. At some point scar revision is in your future for any improvement in its appearance.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Over two years ago I had chin reduction surgery. The surgery went without a hitch; however, my results were mixed. My chin is now asymmetrical, though probably not because of bone. Right below my chin are what I call “pockets of fat” that stick out, making my chin appear asymmetrical. I don’t believe the raised skin is caused by fat—I just don’t have another word for it. I’ll provide pictures and you can judge for yourself. My goal with this message is to find out what is causing my asymmetrical chin and what actions I can take to fix the issue. Hopefully with you as my surgeon. I am hoping I don’t have to go under the knife but if that’s required then so be it.
Picture 1: Sorry for the stupid pose. As you can see my chin sticks out at the bottom and causes an impression on one side of my chin and jaw.
Picture 2: From this angle you’re able to view the “pockets of fat.” Rather than a flat neck the fat sticks out casting a shadow, even. Right under my chin in full view.
Thank you for reading, doctor.
A: Thank you for your inquiry and sending your pictures. While you did not say what type of chin reduction procedure was performed I assume by the scar under the chin it was a submental chin bone shaving procedure. While it would take an x-ray (panorex) to demonstrate that there is or is not any bony chin asymmetry, the most likely culprit is redundant soft tissue. When you reduce bone there always the need to reduce/redrape the soft tissue chin pad as well. That is the trickiest part of the procedure partly because of the need to limit the extent of the submental scar. It is not rare, even when one thinks enough soft tissue has been removed, that it becomes evident later when full soft tissue contraction occurs that there are remaining redundancies. What you most likely need is secondary submental tissue excision.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am looking for advice about getting a forehead implant (and heightened nose job to match) on my very flat and wide Asian face. Could you tell me what order makes more sense to do the surgeries in—find a forehead shaping surgeon first to get my forehead implant in (likely bone cement or maybe Goretex), and then find a rhinoplasty specialist to do my nose to match, or should I do this the other way around?
I also plan on getting chin implant or genioplasty with chin liposuction but I don’t know what order makes the most optimal sense from the point of view of the surgeons being able to optimize ratios.
A: Ideally you should have the forehead and nose done together so the design of the custom implant can be used to also help create the nasal shape as well. But if done separately the order really doesn’t matter, it would be personal preference.
You would definitely do the chin augmentation and submental/neck liposuction together. There is no reason to ever separate these two completely synergestic procedures.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m quite unhappy with my lower eyelid shape and sclera show. Naturally I did some research and checked my options including canthoplasty which brought me to your homepage (very informative). with interest I read the following article of yours:
Case Study – Lateral Canthopexies for Changing The Corner Of The Eye
The following questions occurred to me:
1. do you offer this surgery and do you also treat foreigners?
2. how long lasting will the result be? i heard that canthopexy is opposite to canthoplasty and isn’t really permanent?
3. can you specify what do you mean with ” A lateral canthopexy technique is less likely to round out the eye shape and shorten the horizontal length of the lower eyelid.”? Does that mean the whole eye will get shortened horizontal and the palpebral fissure length will decrease when i would choose a canthoplasty?
4. is there a way to actually increase the palpebral fissure length? if yes, do you offer such surgery?
Best regards
A: Thank you for your inquiry regarding lower eyelid reshaping surgery. In answer to your questions:
1) I do not write about procedures I do not do. About 15% of my prepandemic practice was from outside the US.
2) Canthopexy can be permanent based on how it is performed and secured to the lateral orbital rim.
3) By definition either a lateral canthopexy or canthoplasty derounds the lower eyelid through altering the position of the junction of the upper and lower eyelids at the outer corner of the eye to a higher position. This does not constitute increasing lower lid length.
4) There is no effective procedure for increasing the palpebral fissure length as you can’t pull the lid corner away from close contact to the eyeball. That tight relationship is of critical functional importance.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a Medpor chin implant that I’ve been unhappy with for years. Approximately a year after the initial surgery I had the same doctor shave it down and it’s better but still too masculine. I’m desperate for a slight alteration to narrow it a bit, if possible. Please let me know if I can schedule a virtual consult. Thank you!
A: If you had it shaved down in place then those results are going to be very limited. As a female if you are trying to get rid of the extended wings (which many females are as that style of chin implant is usually not appropriate for most women) it is much better to extract the implant and replace it with a better implant style. This is the more assured corrective approach.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, The back of my head is small and narrow. The front too is narrow. It doesn’t look good when I tie my hair in the lower back of my head. Can an implant be placed at the sides as well as at the back bottom of the head?]I feel like the top of my head is really flat making the hairline flat and the upper back of my skull feels elongated. What corrections would you suggest, please?
A:When designing a head augmentation implant consideration must be given to how much the scalp can stretch to accommodate it. Thus you can’t cover all sides of the head and the front and back unless one has a first stage scalp expansion first. By your description you have essentially described the entire head as deficient. For a one stage skull implant you must keep its coverage to just three sides of the head.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m looking for several implants for my future surgeries and was wondering if you would be able to help me. I have some questions.
Can I order cust9m facial implants in advance for when I am able to have the surgery? Or would it be best for them to go directly to the surgeon.
How much would it cost me for the following masculine implants:
Square Chin Implant
Jawline Implant (Squaring the Jaw)
Brow Ridge Implant (to make it more prominent)
A: In answer to your facial implants questions:
1) Either standard or custom facial implants are shipped to the surgeon, not the patient.
2) Both jawline and brow bone implants are custom designed and made off of a 3D CT scan of the patient.
3) Custom implants can be designed and manufactured (without having a surgery date or paying the fees to install them. (which I think is the question you are asking) You have to pay, of course, the design and manufacturing costs to make them. This is not an uncommon request.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I spoke with you earlier regarding my daughter’s issue with her jaw. You could see it’s protruding and too prominent for her face. We would like to see what her options are. Her teeth are straight but we don’t know if it would help with her bite and jaw structure m, if she would get braces. We did have a consultation here and they recommended she get braces to align the bite and then proceed with jaw reconstruction but we don’t know? She’s 18 and I don’t want her to go through the extremities of this particular surgical procedure. We took her to a plastic surgeon and that’s when the doctor referred me to you.
A: The major consideration you have at this point is whether you are going to treat the facial skeletal disharmony (which is really a combination of upper jaw deficiency AND lower jaw excess) with 1) orthognathic surgery (upper and lower jaw surgery which requires before and after surgery braces….braces alone are inadequate) or 2) a facial camouflage technique of chin reduction and midface implant augmentation.(with or without rhinoplasty) There are arguments that can be made for either approach. Because she is so young this is the time to conclusively rule in or rule out the orthognathic surgery approach.
I can’t see her bite but, more importantly, you have seen an orthodontist who has. It will be helpful to see the digital records that they have taken.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, How realistic would getting the measurement for both ears at 2 inches exactly be? I do understand that extra unilateral scapha underneath the helicle rim could be removed, but would reducing the lobe so that it connects with my skin be a complexity? (as seen in demonstration with hand) Appreciate your time.
A: The question is not whether you can remove essentially the entire earlobe (which is devoid of cartilage) but whether the small vertical scar line that will result is an acceptable tradeoff. Because you have an attached earlobe (as opposed to unattached) any reduction of earlobe length will leave a vertical skin closure line beneath it.
Dr. Barry Eppley
Indianapolis, Indiana
 Q: Dr. Eppley, I am looking for an implant to get the High prominent male model cheekbone, must of them have a flared out look on the sides of the ears and creates a hollow cheek look . With a custom cheek implant with the right size and a long zygomatic arch extension can create that look? Also I heard removing bucal fat is not recommended for young people because ageing we lose face fat and we can end up really thin afterwards but is it necessary to create this look.
Q: Dr. Eppley, I am looking for an implant to get the High prominent male model cheekbone, must of them have a flared out look on the sides of the ears and creates a hollow cheek look . With a custom cheek implant with the right size and a long zygomatic arch extension can create that look? Also I heard removing bucal fat is not recommended for young people because ageing we lose face fat and we can end up really thin afterwards but is it necessary to create this look.
A: The custom infraorbital-malar inplant is the only method I know that can potentially create that type of midface high cheekbone look as you have described and shown. Whether a buccal lipectomy would offer a benefit towards achieving that goal depends on what your natural face looks like. I assume none of the pictures you have attached are you so its necessity in your case remains indeterminate.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 25 year old man and I believe I had scaphocephaly as a kid that wasn’t noticed or treated. Regardless, I have some temporal and prominent forehead. I would like my forehead to be smoothed or shaved down. The temporal narrowing bothers me but not as much as my forehead. What would the price range be and what’s the recovery time? Please get back to me asap.
A: Thank you for your inquiry and sending your pictures. I don’t think you have form of scaphocephaly to account for your temporal/forehead concerns. While temporal narrowing can be improved with subfascial implant augmentation in a virtual scarless manner, such is not teh case with forehead reduction narrowing. While that can be effectively done the exposure to do so requires a long scalp incision which ultimately has its own aesthetic drawbacks. I would question in a young male like yourself the wisdom of that aesthetic tradeoff.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was just wanting to confirm whether jaw implants were available to fix asymmetry in the jawline? I have been to see an maxillofacial surgeon who has advised me that one side of the jawline is “shorter”.
I am hoping to avoid double jaw surgery as I am in my mid 20s and I have been told it is a very invasive procedure which has not been recommend to me for my slight asymmetry.
Thanks
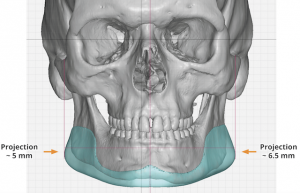 A: Custom jawline implants are done all the time to fix vertical length jaw asymmetries. (see attached) That can be done alone or often as part of an overall jaw enhancement as well.
A: Custom jawline implants are done all the time to fix vertical length jaw asymmetries. (see attached) That can be done alone or often as part of an overall jaw enhancement as well.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 40 year old female born with a weak chin. I had a chin implant placed ten years ago, which was removed 2 or 3 months later. I waited for another year to get a sliding genioplasty to pull my chin forward.
What I DO like about my current chin:
1height and width from front view. I think it’s proportionate to my face. I don’t want my face to be any longer or my chin to be more pointier.
What I DO NOT like about it:
1From side view, it’s apparent that it’s still a little recessed.
2Slight asymmetry and irregularity. It seems that there is a “ball” or soft tissue sag underneath. I am hoping to “tuck in” the chin and increase the horizontal projection by 3 or 4 mm.
I wonder if you would recommend another chin implant or a revised sliding genioplasty?
Thank you very much!
A: Thank you for your inquiry and sending your pictures. Since you like the current height and width of your chin, it would be hard to justify a repeat sliding genioplasty for a 3 to 4mm horizontal increase. (unless you are opposed to an implant) Thus a small anatomic chin implant can be used with the only debate as to whether this is placed intraorally or from below.
The other issue of irregularity and asymmetry of the chin has to do with the prior sliding genioplasty in how the bone was set into position and how the overlying soft tissues have adapted to the advanced chin bone. This is probably not completely correctable by adding an implant onto the chin bone unless a custom designed chin implant was used. (which I don’t think you can justify the cost for that type of modest improvement)
If the chin implant is put in from underneath such access provides the opportunity to ‘tuck in’ the overhanging/redundant soft tissues.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, You are the most experienced and informed regarding facial implants in my opinion. Do you know if one can receive ECT (electroconvulsive therapy) if they have chin and jaw implants? Thank you for your time. Best regards
A: I know of no contraindication to receiving ECT with facial implants in place. The implant material is not a conduit or block of any electrical current.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to fix the natural look of my face. I removed cheek implants ten years ago and my face and smile have never been the same. I am assuming that there was residual scar tissue build up that remained and made my cheeks puffy.
A: Your altered facial appearance has little to do with scar tissue. When you take out cheek implants the support is lost for the tissues that were initially elevated to place them. Thus the cheek tissues drop down to a lower position than existed before. There is no assured way to lift those cheek tissues back up, short of providing some implant support to do so.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am 26 years old and want to have surgery to reshape the skull, and I have deficiency in the anterior sides, and the head back from the top. (scaphocephaly) What is the best type of implant to do so? Plus what is the life span of the implant and the recovery time from the surgery. And what is the possibility of it moving or falling out of place. And knowing the scar, will it stay visible for a long time?
A: Thank you for your inquiry. In answer to your skull implant questions:
1) The first place to start is to see some pictures of your head to determine its dimensional augmentative needs. Very often in adult scaphocephalic skull shapes a combination of sagittal ridge reduction with parasagittal-temporal augmentation is needed.
2) The type of implant material is one that can be designed from a 3D CT scan, can be placed through the smallest scalp incision possible, and is gentle on the oveyling scalp/hair follicles….the only material that meets all these needs is solid silicone in my experience..
3) Such skull implants last forever and can never degrade or breakdown.
4) Recovery time is about the resolution of swelling which takes about 2 to 3 weeks to largely appear more natural in appearance.
5) Placing such skull implants actually adds a layer of protection to the skull when exposed to trauma. Such implants can not be displaced or dislodged from almost any form of trauma to the head.
6) The scalp incisions used for skull implants are often fairly small and heal well with limited visible scarring.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I wanted to get your recommendation about what surgeries should i get to enhance my appearance but stay natural at the same time .
what i think i need:
1. lower lip reduction
2.filler or implant for chin
3.filer or implant for jawline (i dont want to widen it just want some bone to appear on the gonial angle
4.filler or lipofilling for sunken upper eyelid hollow (do you think i have protruding eyes ?cuz faceapp filters always make my eyes smaller)
5.treatment for dark circles (it’s genetic hyperpigmentation) it seems that there are no guaranteed and effective treatment for this problem
6.what hair style more suitable for my skull and facial features?
A:Thank you for your inquiry and sending your pictures. In regards to your questions I can say the following:
1) Part of the lower lip position is due to the short chin but there is no question that the lower lip is disproportionately big and could benefit by reduction.
2) Your chin needs a sliding genioplasty, not filler or implant. It will help with the lower lip support.
3) Since your jaw angle goals are to just make some evidence of a jaw angle presence, I would go with standard vertical lengthening jaw angle implants.
4) You have a combination of an infraorbital rim deficiency and hyperpigmentation of the lower lids. It is a choice between lipofilling and infraorbital rim implants, each with their own advantages and disadvantages. I would probably opt for the imnplant because of the more assured smoothness that would result.
5) You are correct in that lower lid hyperpigmentation is a difficult problem to improve. But efforts using bleaching creams is a good place to start.
6) I have no expertise in hairstyling.
In conclusion a sliding genioplasty with standard jaw angle implants and lower lip reduction for the lower third of the face and standard infraorbital rim implants with pre- and postoperative bleaching creams for the midface
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 19 year old male, potentially looking to get a chin implant removed. The type of implant is a Terino square chin style 2, size L (attached picture of dimensions). The implant was placed with an incision underneath my chin. I got this implant placed into me this past summer. I was wondering if i get it removed, will my skin around the chin return to where it was before? I am mainly concerned with sagging of the tissue and also if there would be any loss of bone from resorption causing my chin to look more recessed than before implant.
And also would the scar tissue cause a permanent gain in augmentation after implant removal?
Since you say the tissue does not revert back with a style 2 chin implant after removal, would it be possible to make the tissue the same as it was before with something like skin tightening, or anything else if I decide to remove the implant sometime in the future?
And in case there is any resorption like in attached picture, would it be possible to fill in the area with bone graft to permanently fill the resorbed area?
Thanks
A: In answer to your chin implant removal questions:
1) It would be fair to assume that removing your chin implant is not going to allow the chin soft tissues to completely return to their preoperative state. While they have a good ability for substantial shrinkage you can’t release all the ligamentous attachments to the front of the chin and place a big implant (which a style 2 large chin implant is) and expect everything to go back exactly to what it was. The question is not whether there will be some changes but how significant they will or will not be.
2) Any residual scar tissue is not going to create any really visible chin augmentation effect.
3) Certainly device-driven forms of tissue tightening will not hurt. But in the end it is largely about how much soft tissue shrinkage your soft tissue can do on their own.
4) The best approach for such bone recontouring is hydroxyapatite cement not a bone graft.
Dr. Barry Eppley
Indianapolis, Indiana
What Should I Replace My Submalar Cheek Implants With To Give My Face A More Masculine Angular Look?
Q: Dr. Eppley, I’m a 45 year old male that had submalar implants placed about eight years ago in hopes to give my face a more masculine angular look and help my nasolabial fold area. I feel they are preventing me from smiling fully and created an “overfilled”and feminine look. I think I’d like to remove them and change to something more lateral like a malar implant . I do not want the scars of a mid facelift but would like to improve the nasolabial area in another way with implants if possible.
A: You have unfortunately discovered that most standard cheek implants (technically all of them) feminize the male face. Men need a high horizontal line of augmentation along the cheekbone and zygomatic arch, not the anterior fullness created by current malar and submalar implants. The only question is whether you want to modify a standard malar implant or use a semi-custom vs custom cheek implant approach to replace your existing cheek implants. Such cheek implant replacements are not going to reduce the depth of the nasolabial folds which require a bone-based implant underneath them to help in that regard.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a fat transfer under my eyes to help correct hollowness and dark circles but unfortunately, I am left with an overfilled sausage like mound under my right eye and lumps under my left eye. The mound and lumps are soft. How can the mound and lumps be removed so that the area under my eye is smooth again?
A: One of the real problems with fat injections to the lower eyelids is the unpredictability of volume retention and smoothness. The thinness of the lower eyelid tissue is very unforgiving of any contour irregularities. To reduce overfilled lower eyelids this would require an open lower blepharoplasty to remove some of the fat transfer…or at least the largest lumps/mounds.
Dr. Barry Eppley
Indianapolis, Indiana