Your Questions
Your Questions
Q: Dr. Eppley, I had a sliding genioplasty 7 years ago and have had tightness for years and recently figured out I have adhesions under my chin. I had an area of hair loss under my chin in the beard where there are adhesions. However, with massage of the area for the last few days I’ve noticed the adhesions seem to be improving and also the beard hair is growing back (after years!). Is there any utility in PRP/steroids/5-fu or is just continuing to massage the area best. I also was going to look into surgery but think now perhaps that’s not necessary.
Appreciate your help.
A: There is certainly no harm from massage or any injectable therapy around or into the sliding genioplasty site. Time will answer the question about their long term effectiveness.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, For a forehead, supraorbital implant, how do you prevent the raising of the eyebrows that occurs with this augmentation?
Ive had a brow bone implant and took it out because it made my eyebrows very high due to the lift and push up and out effect.
Is there anyway to fix this?
A: That is not an eyebrow effect that I have ever seen from a custom forehead-brow bone implant. That sounds like a placement/implant design issue. Unless one has a lot of experience it is very easy to get a brow bone implant placement too high (inadequate supraorbital release) or have an implant design that does not get the brow bone effect low enough.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a moderately recessed chin and my bite is class 1. What I noticed on my lateral cephalogram (and by felling the chin) is that my soft tissue pad is very thin. The bone is more or less normal size, but the thin soft tissue and thick lips make it look recessed even more.
Is it possible to bulk up the mentalis muscle a bit to give the impression of a stronger chin? Or would it produce counter results – I read a study that found using Botox to relax the mentalis muscle actually made the chin look horizontally stronger.
Thank you and kind regards
A: There is no surgical or non-surgical method to make any muscle of facial expression bigger in size. I can not imagine the biologic mechanism by which Botox (which causes muscle atrophy) would make the mentalis muscle bigger nor make the chin look stronger by muscle relaxation. But I know one way to find out…do it and see what happens.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am now three weeks after my sliding genioplasty and jaw angle implants. I have more questions as I am starting to be able to chew and I’m stretching my mouth multiple times throughout the day.
My mouth feels dry all the time is that why my sutures haven’t fallen out yet? Should I constantly swish water around my mouth?
As I’m starting to eat more food I’m cautious to eat anything that could get stuck around the sutures. Could that cause an infection?
Is it possible to stretch my mouth so hard I mess up a suture?
Is there an estimate when my mouth will open up normally? I’m fitting about 1.5 fingers in currently.
Will my normal smile return? Is there an estimate time frame of that happening?
Can I chew mastic gum to strengthen my jaw back to normal?
Can I get a tattoo?
Can I resume allergy shots?
Can I start light exercises(push-ups, pull-ups, abs)
When can I start lifting heavy weights?
A: In answer to your post surgery sliding genioplasty and jaw angle implant questions:
1) There is no correlation between mouth dryness and sutures dissolving.
2) You are rightfully cautious about food getting stuck in the sutures in the first month after surgery.
3) Wide mouth opening does pull on the sutures in the lower vestibule.
4) Keep working on stretching and it will eventually return to a normal range of motion.
5) A full smile will return when the tissues in the chin heal and relax. This a function of tissue stiffness/stretch that is temporarily affecting a normal smile movement.
6) Now is not the time to be chewing gum.
7) A tattoo anywhere other than the face is fine.
8) You may resume allergy shots.
9)You can start light exercise any time.
10) I would wait to resume heavy weight lifting until one month after the surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Could you please check my case and tell me the best technique to reduce my ear size also and the expected vertical length after surgery nothing that the current length is 70 mm also I want to know the probability of both ears will not be identical after the surgery.
Thanks
A:Thank you for your inquiry and sending your picture. There are only two techniques for reducing ear size (vertical ear reduction), the scaphal flap for the upper half of the ear and earlobe reduction for the lower half of the ear. Maximal vertical ear reduction occurs when both are done together, if indicated, which in your case they are not. You have a normal earlobe size which means only the scaphal flap technique would be used. As a general rule your vertical ear height would be reduced from 70mm to 63/64mms maybe more.Provided that the ears are not significantly different in shape/size now I would expected there not to be any significant asymmetry afterwards.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have always been super self conscious about the width and size of my back. I lost weight and my back is just huge and I’ve realized no weight loss will create a feminine look of my back. I’ve always wanted a smaller back and didn’t know if there are surgeries to reduce the width and size of my back. My broad shoulders look beautiful in the front because I am 5’7” 131 pounds. Just in the back it makes me look chunky and less feminine and very boxy. I just want to be able to have to have a smaller frame and more delicate look. I always get confused because I take pictures like this and my back looks massive and makes me look large and I take other pictures and it looks like my back is super skinny and contoured. Through other people taking my picture I have seen more that my back is just super wide and i just am looking for a way to reduce that upper and mid section of my back I feel like my arms stick out like a triangle. I hate this and would love to fix it at some point.
A: Thank you for your inquiry and sending your picture. There are not any surgeries specifically for reducing the width of the back. The only operation that may affect the width of the back is shoulder reduction combined with upper liposuction but i don’t think that would have much effect on where your specific concerns are. (see attached imaging)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a double jaw surgery with genioplasty and rhinoplasty six weeks ago. My lower and upper jaws were advanced and my chin was made too pointy (width was decreased in an attempt to make it V-shaped) and increased vertically as well. I don’t think there’s any way to increase the width of my chin anymore, but I want to at least reduce the vertical height and also slide it a bit back. It was advanced 15mm vertically and 10mm horizontally. I want it reduced full 15mm vertically (or at least 10mm) and 5mm horizontally too. How long should I wait for that ? Considering I also had double jaw surgery and rhinoplasty in my surgery. Also, is it possible to increase the width by placing the bone in the space so created in genioplasty, and thus aligning it with the bones of previous chin. I feel that if it is done now maybe the width can be regained if complete reversal of genioplasty is done.
A: While I would have to see some postop x-rays to answer your question in a more fully informed manner, the chin bone movements as you have described seem plausible but a bone graft would be needed for the widening effect. (the vertical reduction is not going to create the graft needed as that is just a space that is not filled in with bone). You make these chin changes when you are certain that they needed to be done…which most patients know when they are 6 weeks out from surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’d like to know if this kind of facial look could be achieved through osteotomies and/or fillers. Or maybe osteotomies plus fillers. I’m a bit scared about the implants infections. The first two photos are about me, the third photo the model look I’d like to achieve, augmenting jawline and zygos (ogee curve). I’d like also ask if my face/midface could be shortened.
A: Since you have provided only a front view the most major change appears to be that of the jaw angles. Short of implants temporary injectable fillers would be the only option to widen your jaw angles or augment the cheeks areas. Short of a subnasal lip lift (which you do not need) there are no midface shortening procedures.
The one caveat would be that of the zygomatic sandwich osteotomy (ZSO) for the cheeks. But there is no osteotomy to widen the jaw angles.
Dr. Barry Eppley
Indianapolis, Indiana
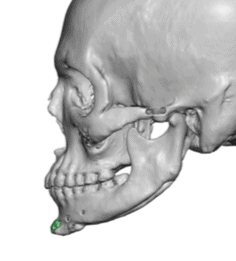
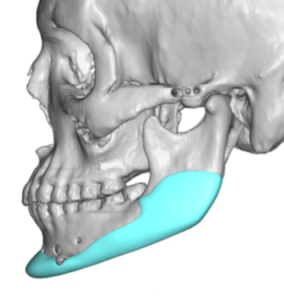
Q: Dr Eppley, Attached are before and after photos of me having received chin filler. I am seeking a permanent solution and I am possibly interested in setting up a virtual consultation and traveling to you as it seems you specialize in this procedure. Could you provide me information on your pricing?Do you feel I would need just a chin implant or if there is a different procedure you’d recommend? How long I would be out of town for? And would I have to wait for my filler to dissolve before getting treatment? My desired results are those from the first screenshot with the pink blush.
Thank you! I look forward to hearing from you.
A:Thank you for your inquiry and sending your pictures. By looking at the chin filler change that appears to be about a 5 to 6mm horizontal advancement change. I even did my own imaging of what the type of chin augmentation change I think you are looking to achieve. Given this modest amount of change I would go with a chin implant as opposed to a sliding genioplasty. You would not have to dissolve your filler before having the procedure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a prospective patient (male) who is interested in minimally invasive jaw defining procedures, namely the removal of the buccal fat pads. I am interested in learning more about this procedure as well as the potential range of costs for this procedure.
I look forward to hearing back from you!
A: I am not sure I would call Buccal Lipectomies as ‘jaw defining’ as that is over stating what the procedure can likely achieve for most patients. In addition most buccal lipectomies need to be combined with perioral liposuction for a more complete thinning effect between the superior cheekbones and the inferior jawline.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I sent two photos … one for my head from its right side and I like it but the other one from left side there is huge elevation like rock in my occiput … is it possible to make the left side like the right and how ?? also I want to know how the procedure get arranged and how much does it cost??
Thanks in advance
A: Thank you for your inquiry and sending your pictures. It appears to make the left side of the back of your head look like the right this will require bone reduction to do so. The amount of reduction to achieve that change sees to be within the amount of bone that can be safely removed. But ideally one should have a CT scan to measure the actual differences in bone thickness.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’d like to ask you a question.This year I’ll do an Ilizarov surgery to lengthen my right leg. I know that Ilizarov could cause infection, but you can cure it with antibiotics. If I get from you a custom wrap around jawline implant fBEFORE the Ilizarov treatment could an Ilizarov infection cause the infection to spread to the jawline implant?
Thank you so much
A: I know of no infectious correlation between a jawline implant and a lower extremity device procedure regardless of the order in which they are performed. Specifically do I think that a bone infection from limb lengthening procedure could cause a delayed infection in a well healed previously placed jawline implant…I think that would be very unlikely.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, I had a sliding geniolplasty of 8mm forward and 4mm vertical increase 6 weeks ago. I absolutely hate how it has made my chin pointy and my face too long. I believe an advancement of 5-6mm initially would have been perfect. I would like to know what the differences are beween a primary and secondary genioplasty, and how accurate a second procedure would be as well as the risks/complications. Will the skin sag/ change? Will the bone heal completely after a second procedure? Is there any reason to have it done sooner rather than later or vice versa or not at all? Would decreasing the vertical height by 3mm and forward projection 2mm be sufficient? I’m sorry I have a lot of questions as I am incredibly depressed at my current look as I had a really nice face before and have made it worse. If you could help me with these questions I would be more grateful than you could ever know.
A: In answer to your secondary sliding genioplasty questions:
1) You perform a secondary sliding genioplasty to change the chin bone position when you are certain you are looking at close to the final result and you know what specific dimensional changes need to be done to make it look better. Usually patients have as very good idea around the 6 week after surgery time period.
2) A secondary sliding genioplasty is essentially the same procedure as the first one. The same bone cut is followed as the first time. It is usually less traumatic to the patient the second time as the patient already knows what to expect.
3) The risks and complications are theoretically the same as the first time…although the aesthetic risks are less since you have a known dimensional change and you know exactly how it looks.
4) If the original movements were 8 forward and 4 down then it would seem logical that less of each would be an improvement. At the least it would seem halving each one, 4 forward and 2 down, would be a good aesthetic compromise that is more than you had initially (there is a reason you had the procedure) but less than what you know you don’t like. However I would need before and after pictures to provide a more qualified dimensional change recommendation.
5) The bone will heal just as well the second as the first time.
6) There are no concerns about loose chin tissue in a setback of this amount.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have an idea of how to get smaller waist in addition to rib removal, lipo etc… Dont know if it would be possible..
Do you know if it would it be possible to draw the lower parts of the sides of the rib cage closer together to form a wasp V shaped tiny waist? Would the ribs be flexible enough to be drawn closer? Instead of wearing a corset for 3 years to form some sort of V shape, would it be possible in one go to draw them closer in a plastic surgery procedure? Using a resorbable material in the middle, to hold the sides together, yet at the same time be able to breathe perfectly fine?
From pectus escavatum videos it seems like the ribs are movable to a certain degree…. as long as its possible to squeese the ribs sides closer this should be possible? I mean women centuries ago wore corset all the time and ribs got shaped… to form a wasp waist… I don’t know of any plastic procedure to create a wasp waist other than ribs removal… yet I am looking for an even more extreme V shaped waist. I don’t like wearing corsets, so Im looking for an other way.
Also… would it be possible to have an internal corset made of a biocompatible reabsorable scaffold under the skin, in addition to rib removal, and ribs set closer together? I just think tiny waists are so beautiful:)
Thanks
 A: Thank you for your inquiry and putting forth your idea on a method to make the waistline smaller. Unfortunately the attached ribs are not particularly flexible so they can not be bent inward during surgery or held in such a fashion by any internal support means. There is also the issue of acute compression on the lung space (which is not affected when they are expanded outward like during the Nuss procedure which actually improves the lung space) Corseting works because of very long term pressure molding…somewhat similar to how orthodontic appliance pressure is able to move teeth through bone.
A: Thank you for your inquiry and putting forth your idea on a method to make the waistline smaller. Unfortunately the attached ribs are not particularly flexible so they can not be bent inward during surgery or held in such a fashion by any internal support means. There is also the issue of acute compression on the lung space (which is not affected when they are expanded outward like during the Nuss procedure which actually improves the lung space) Corseting works because of very long term pressure molding…somewhat similar to how orthodontic appliance pressure is able to move teeth through bone.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, How can the occipital implant be fixed in the head?
A: The fixation any skull implant is by both screw fixation and the tightness of the tissue pocket in the short term and by tissue ingrowth through the implant in the long term. (through the created perfusion holes in the implant)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, I am interested improving my jawline. Ideally, I would like to have a stronger and more chiseled jawline. I would like to have a wider and more angularity to the mandibular angle. I look forward to hearing from you.
A:Thank you for your inquiry. There are three methods to enhance your jawline; 1) standard chin and jaw angle implants, 2) custom jawline implant and 3) sliding genioplasty with custom/standard jaw angle implants. Each one has their own advantages and disadvantages.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question about forehead width. I have quite prominent contours at the borders of my frontal bone which are wide at the top but then taper down to become very narrow at the bottom, where they join with my orbits. I am wondering if there is a way to build up these contours to make my forehead appear slightly broader/squarer as oppose to triangular. I have attached a diagram of a random skull below, to illustrate the area which I would like to augment, and the desired effect. (Red is original border, blue is desired outcome).
I also have a question about the materials. I would ideally like to use a bone cement for this procedure as I believe it might be cheaper and I am comfortable with a larger incision if it would save costs. Would this be possible? Or would the only way to do such an augmentation be to use custom silicone implants? Thank you for your help.
A: When you expand the lateral border of the temporal line of the forehead you have to have the implants placed on top of the deep temporal fascia, not underneath the temporal muscle. Thus this can not be accomplished by bone cements as they simply can not be put on top of the fascia without a full coronal incision and would have an abnormal edging to them. You can’t hand make such a shape very predictably and have it also be perfectly symmetric.
Besides the aesthetic issues and need for a coronal scalp incision, it is also not less expensive. While the cost of the raw materials does differ it also takes 3X as long to do a bone cement forehead augmentation as does a custom forehead implant….which more than wipes out the lesser cost of the PMMA bone cement. (HA bone cements can not be placed on soft tissue as they crack and break apart)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi, I have what is referred to as a “buffalo” hump, aside from the obvious cosmetic worries it has also begun to the limit the range of motion of neck, contribute to serve neck/upper back pain, headaches, and difficulty sleeping. I have tried the more conventional methods including exercises to strengthen my back and chests muscles to no avail. I am a fairly thin individual to begin with so diet and exercise has done little to help. I was curious what your thoughts were, if this is achievable, and the cost of such a procedure.
A: Thank you for your inquiry and sending your picture. Small buffalo humps can appear even in thin people as this is a residual area of brown fat in babies. Brown fat is resistant to conventional methods of fat reduction as it is very different metabolically from all other fat. It can only be removed by small cannula liposuction.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I recently got a chin implant along with mandible implants. I am 9 days post op and have huge swelling. My face looks like a complete square at this point and I am worried if it will stay like this. Do you have any suggestions to help with this swelling and edema.
A: This is normal at this early time after surgery and the resolution will be more healing time, Your surgeon should have educated you about this degree of swelling and it will take 2 to 3 months for all of it to go completely away.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Good morning. I have a question about trichophytic incisions. After a procedure, roughly how long does it take hair to grow back through a trichophytic incision back to it’s regular density?
I had surgery with a coronal incision 3 months ago, and although the hair is growing through it still is not back to its regular density. Will it probably take a little longer?
A: Time will tell but I would not expect it to grow back through the scar in the same density that existed in the scalp area before even if a trichophytic incision was used.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, The top back of my skull is depressed due to surgery as an infant. The depression is deep, wide and long so if plastic surgery was performed it would need to stretch skin or need a skin graft. I’m not sure of your capabilities but has your practice dealt with the issue described. Thanks.
A:What you are suggesting is the possibility of needing a first stage scalp expander procedure. (not a skin graft) That is a procedure I do regularly when more stretch of the scalp is needed for the amount of skull augmentation required.
Dr. Barry Eppley
Indianapolis, Indiana
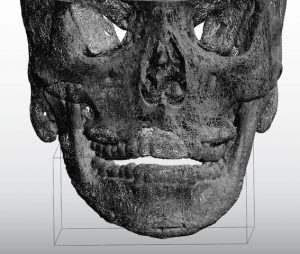
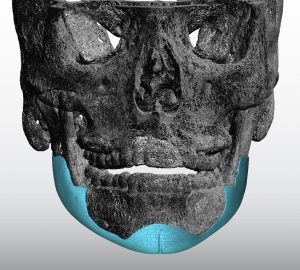
Q: Dr Eppley, Thank you so much for replying to my question about v line reversal implant surgery! May I ask how high the infection rate is for a custom silicone implant as that is a problem I am scared of having. Also since I had a sliding genioplasty. to make the new custom jawline implant that wraps around my whole lower jaw would I need to reverse the sliding genioplasty to put the implant in or would it be okay to leave at where it is at since my chin still does not have enough projection and it was moved foward 10mm. Thank you!
 A: In an
A: In an
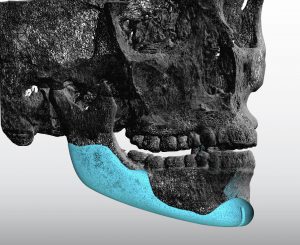 swer to your v line reversal surgery questions:
swer to your v line reversal surgery questions:
1) the infection rate in custom jawline implants is in the 3 to 4% range.
2) the sliding genioplasty stays in place and you build around it.
3) the attached images may be helpful in understanding how the implant works in v line surgery reversal.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had jaw reduction surgery along with a sliding genioplasty however, the surgeon over reduced my lower jaw and I developed step-off deformity from sliding genioplasty. The lower half of my face is over reduced and smaller than the upper part making my face look off-balanced. I would like to rebuild my entire lower jaw. Would I need jaw and chin implants or would I have to get a custom jawline implant? Would bone cement be okay for an implant or is silicone better? Would bone grafting work? What are the pros and cons of bone cement/silicon implants and bone grafting?
A: Over reduction from vline surgery is actually very common and is just the nature of how that surgery has to be done. When it comes to rebuilding the inferior border of the lower jaw (which is what is now missing and is what is the cause of the notch deformity from the sliding genioplasty) this can only be done with a custom implant approach. Bone cements, standard implants and bone grafts are not going to work and will just make matters worse. Besides the fact none of these can stick and create a new extended jawline border out into ‘space’ they will be associated with a very irregular/asymmetric jawline result…which will be worse aesthetic problem than what you have now.
 One can have debate about the use of silicone or Medpor custom jawline implants (PEEK is not commercially available in the US for jawline implants) but economics will end that debate for a custom silicone jawline implant in most cases.
One can have debate about the use of silicone or Medpor custom jawline implants (PEEK is not commercially available in the US for jawline implants) but economics will end that debate for a custom silicone jawline implant in most cases.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have mandible implants sized 11mm and chin implant sized 9mm ( all silicone) I am now3 months post op and am planning on getting them all removed. Will my face go back to the way it was? If not how close will it be? I’m 23 years old and I have thick skin according to my last surgeon.
A: The key question is if you knew your face would not go completely back to the way it was….would you still take out the chin and jaw angle implants?
The point being is that no one can predict precisely what will happen when they are removed. There are always going to be some aesthetic tradeoffs from removing them because of the stretched/expanded tissues. The only question is whether those aesthetic tradeoffs are better than living with the way you look now.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have done a CT of my face and my Dr left me know that my right side of face is around 5 millimeters more retruded so the other side is 5 mm more forward. I know there are implants for that purpose but I want to try with own materials
So do you think it is possible to move forward the midface more than 5 mm including: FRONT OF ZYGOMA, MALAR AND CHEEK BONE up to around the nose and infraorbital area. This is my concern how much can be forward midface on one side but no jaws not necessary pnly face: front of face : zygoma, infraorbital malar…( Augmentation)
How would you perform that please. Through osteotomy forwarding or in combine with bone grafts but remember please it is necessary for 5 or 6 milimeters augmentation for that i need to know how can be done this without implants.
And please dear sir what you think is it possible to gain a very good symmetry with both sides through osteotomy and using bone grafts.
You are very experienced surgeon and you may know how much symmetry can be achieved
Many thanks
A: The dimensions of the bony augmentations of the midface you seek are anterior and can not be done by any type of osteotomy. (bone movement) Your only autologous option is onlay bone grafts which will not provide a smooth contour and will likely undergo some resorption…and perhaps even complete resorption over time.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a young male in my 20s. My right shoulder is shorter than the left since I was born. It is genetic. My father has the same condition. No problems except cosmetic reason. My right clavicle is more curved than left.
I want my both shoulders equal and identical. Is it possible Sir?
A: Thank you for your inquiry and sending your pictures. It appears your right clavicle is shorter than the left one, perhaps by about 2.5 to 3 cms. Conceptually the right clavicle can be lengthened by the placement of an interpositional fibular bone graft of that length. The key question is where on the shaft of the clavicle should that be done. It appears that the inner third of the shaft would be the best location for the osteotomy and graft. Although a 3D CT scan of your shoulders would show the clavicle anatomy in detail and would be very helpful in making the decision for the best osteotomy location.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi, as you can see on the images in the file I look a LOT better on the right. They were both taken today, the only difference is that I bite together on the left picture which in my opinion looks horrible. On the right I jut the jaw forward and downward. (I think my whole lower jaw is too short as well)
I’m going to have double jaw CCW surgery in a while for health reasons, but when it comes to aesthetics I’m not sure it’ll do the trick.
As you may understand, my dream look is on the right, how do I achieve that in combination with double jaw in the best way? Hope you understand what I mean.
A: Thank you for your inquiry and sending your pictures. While such a facial change as you have illustrated is possible it can not be done at the same time as orthognathic surgery. You need first to get the skeletal foundation functionally corrected and then you can build off that to augment the remaining missing contours. Orthognathic surgery will provide some sagittal forward jaw movement but not any width or angular contours This is going to require a custom jawline implant AFTER your orthographic surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have very noticeable bumps behind both ears. I had a scan a few years ago and it is due to unusually large mastoid air cells. Can something be done about this? I’m 38 and get made fun of wherever I go.
A: Enlarged mastoid processes can be reduced. The key is knowing that these are air cells so in their reduction the mucosal lining needs to be removed and covered in hydroxyapatite cement to prevent postoperative infection.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, What I’m confused about is I also consulted with another surgeon. He suggested a 9 mm silicone off the shelf without wings. He’s not reshaping it, implant as is so yes the implant is round. I held it. While your imaging suggests a 4 to 6 mm size, at least the ones that are appealling me. So are you under projecting or is the other surgeon’s size is big?
I included the other surgeon’s imaging if that helps.
A: Based on your response to the larger imaging 9mms would be too big for you. That is my opinion as I would never place a 9mm chin implant in you or almost any female if they don’t like the predictive imaging.
The concept you have to grasp in that such implant selections are not an exact science and, even you the patient, don’t know how you will really respond to any size implant placed in you. Up to 1/3 of all facial implant patients ultimately change the size of their implants in a secondary procedure for a variety of reasons. That is the nature of facial reshaping surgery and the unpredictable psychological response of patients to changing the shape of their face they have looked at their entire life.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Could you ask Dr. Eppley how many millimeters is added to the chin on the first set of images and the second set of images? And how many millimeters you think is perfect in my case? I just want an idea. I feel better with the second set of images.
And whether the silicone he plans for me is the extended anatomical silicone that goes up my jaws or without wings.
During the consultation he said it’d be a v-shape silicone that he’d have to shave it into.. too much to ask but would he happen to have a picture of someone he did the same to?
I know you secure your chin implant onto the chin bone with a metal screw. If I ever need to do an MRI for whatever reasons, will that metal screw be a problem?
A: In answer to your chin implant questions;
1) Computer imaging is not really done by known millimeter increments. It is done by general ranges of changes. For example, the first set of imaging was probably in the 6 to 8mm range while the second imaging was in the 4 to 6mm range.
2) The perfect amount of advancement is the one that you like the best….which is why two different types were provided.
3) Most women do not like chin implants with extended wings because it makes their chin look wider from the front view. This is why for most women, unless they specifically request a wider chin, I use the anatomic style chin implants.
 4) All anatomic chin implants are a bit round by today’s female desires so I usually reshape that into more of a V-shape.
4) All anatomic chin implants are a bit round by today’s female desires so I usually reshape that into more of a V-shape.
5) Any screws used are made of titanium, a non-ferromagnetic metal. So it has no interference with MRI studies.
Dr. Eppley
Dr. Barry Eppley
Indianapolis, Indiana