Your Questions
Your Questions
Q: Dr. Eppley, I am looking for a consultation on breast augmentation. I have asymmetry issues and would be curious about not only evening out, but enlarging both breasts from a small B to a full C. I am not familiar with what a price would be for such a procedure, but I would appreciate a range/estimate to know what I’m getting into.
A: Breast asymmetry comes in many forms but your description suggests that it is a volume issue as opposed to one breast being smaller and sagging as well. (which poses different considerations) If it is a pure volume issue, then breast augmentation surgery alone may suffice…just using different implant sizes to make the mound ssomewhat more symmetric. While one can never achieve more symmetry or evening them out perfectly, breast enlargement with two mounds that are more symmetric is possible. This, then, other than having two different sized implants is a straightforward breast augmentation procedure. The cost of breast augmentation is dependent on what type of implants are used. (saline vs silicone) and not on the implant size so knowing your implant choice would be helpful in answering the cost question.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, if I get silicone breast implants will I be able to breastfeed? If I get pregnant after breast augmentation should I first check and see if the implants are ruptured before breastfeeding? If the implants are ruptured can I breastfeed or do I need to get the implants out immediately or can I let my son self wean??
A: You taken taken the classic ‘can I breastfeed with implants’ question to every conceivable scenario. Most breast implants today are placed under the pectoralis muscle well below the glandular breast tissue. As a result there is no interference with milk production or breast feeding. If you have no symptoms suspicious of an implant rupture (pain, change in breast shape) I see no reason to get an ultrasound, mammogram or MRI before breastfeeding, In addition, the implants are contained within a surrounding scar capsule so even if there was an implant rupture there should be no silicone in the milk ducts. However, in the event that you have a rupture and are breast feeding, I would suggest that you do not breast-feed until you have had the rupture evaluated by a board-certified plastic surgeon.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a breast augmentation three weeks ago. I am no longer worried about any particular problems at this point as they look great. What I wonder is if the heat from a hot tub can weaken the implants in any way or cause them to prematurely break down and leach out the silicone material.? Could it weaken them in any way? I have read that it is ok to swim after they are healed but can’t find anything about what happens if they are immersed in temperatures above body level like 104 or 105 degrees. How heat resistant are these materials?
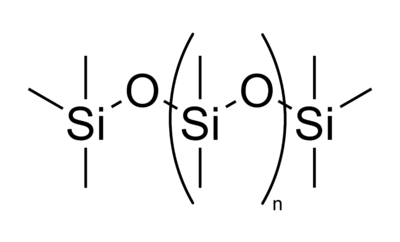
A: The answer to your question comes from the Periodic Table of Elements. Breast implants are composed primarily of silicon-based materials. Silicon is a metalloid element (#14, atomic weight 28) that is very stable and non-reactive. (it is actually less reactive than carbon) When combined with oxygen, a wide variety of polymers are created which are used to create elastomers (rubber-like materials) which make up breast implant shells and the internal gel. They are very resistant to degradation including a high heat resistance and are structurally stable from temperatures ranging from -55 degrees to 300 degrees F. Thus a hot tub poses or even a sauna that reaches air temperatures of 150 degrees F or higher poses no risk of causing any implant-related issues. This is not to mention that they are also protected by your body tissues which would suffer a burn injury far sooner than your breast implants ever would.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in breast augmentation and possibly breast lift. I live in Minnesota but my best friend lives in Indianapolis and she suggested you. I am wondering is I were to come to Indiana for the surgery if I could have a consultation with surgery the following day. Also, being from out of town, how often would I need to be rechecked?
A: There would be no problem with scheduling surgery and just having a consultation the day before. That is a common occurrence in my practice as we see patients from all over the world every week. To make that happen effectively there are certain breast augmentation questions that should be answered in advance. They include the following:
1) Are you interested in saline or silicone breast implants?
2) Are you interested in round or shaped (anatomic) implants if you prefer silicone?
3) Do you have an incisional preference for placing the implants of lower breast fold (inframammary) or axillary (armpit)?
4) What size result do you want? (pictures are helpful here of breast augmentation results you like)
5) What is your height, weight and current bra size?
6) Do you have any breast sagging? (this is a very important as if so a breast lift may be needed with the implants)
If you have the ‘perfect’ breast for augmentation (no sagging, nipples locate well above the lower breast fold) then presurgical photos may not be necessary. But if your breasts may be less than perfect or have known sagging, please send me some pictures of them so I can know in advance as to what you exactly need.
As for follow-ups, I like to do phone, Skype or Facetime conversations to accomplish that for my far away patients. Between pictures and e-mail communications, all the follow-up that is ever needed can be done at a distance. From these we can make the determination if you ever need to come back and be seen by me in person.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I reviewed some of your work and like what I see. Does breast augmentation affect nipple sensitivity or the ability to be erect? Where are the scars located? What is average cost of the procedure?
A: The potential influence of breast augmentation on nipple sensation and erection is always a possibility in this surgery but the incidence of it occurring is very low. Various studies have shown that the incidence is around 1% to 3% regardless of the differing incisions used for implant insertion. (under the breast, the nipple or the armpit) The choice of incision location is somewhat dependent on what type of breast implant is chosen. (saline vs. silicone) Silicone implants can now be placed through the armpit using a funnel insertion device but there are size limitations which are usually less than 400cc to 450ccs in implant volume. Any size saline implant can be placed through the armpit since they are inflated after they are put in place. The cost of breast augmentation is affected by the implant type with saline breast augmentation being less costly than that of silicone breast augmentation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I wanted information about getting breast implants for my wife. How much do they cost and what are the payment options? What size is better for her? How long does it take to do the procedure?
A: The first question about breast implants is what type does your wife want. That is an important decision for various reasons and one of them is cost. Saline breast implants will cost less than silicone breast implants. The size of breast implant any woman wants is a personal one and I can not tell any woman what size breast implant she should have. I can guide her with her decision but she will have to provide some input. The best way to do that is to look at before and after breast augmentation results and show me some of the results that she likes. Otherwise, breast implant surgery is done under general anesthesia and takes one hour to perform.
The typical full cost of breast augmnetation is $4700 for saline implants and $5800 for silicone implants. The most favorable and convenient formk of financing is through Care Credit.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am going through back problems at the moment but didn’t know if it was still ok to get breast enlargement and a tummy tuck. I am already on all kinds of medicines and have back pain but I think I am getting to the end of this, finally. I had worked out and walked four miles a day to loose weight and quit smoking then my back started acting up the tummy tuck and breast enlargement is something I have wanted since I had my three kids which I love dearly but ruined my body. I would like to know how long I should wait, I also have a hernia that they said unless it didn’t hurt all the time then don’t come back until it did . I’m sorry but I just feel like my life is on a complete hold while still wanting to look better and feel better about myself. I have to be at the mercy of all of these other problems before I can have my life back and have these things done to make me feel better about myself. Please reply with an honest answer all of what I am going through now is very heartbreaking so a reply soon would be greatly appreciated. Thank you.
A: While breast and abdominal reshaping can make some dramatic changes in any women who has been through three pregnancies, I have numerous concerns in your case if this is appropriate. Your history and ongoing back pain are concerns as well as what medications you are on. Breast augmentation and a tummy tuck are not a cure/treatment for back pain and may well make it worse in the short-term after surgery. I would imagine that some of the medications you are on are for pain relief, which would make any narcotics needed after a breast augmentation and a tummy tuck less effective. A detailed medical and medication history would have to be assessed to see if such body contouring would be advised. In addition, your hernia repair history is also significant for consideration for tummy tuck surgery. Your surgical records for this procedure(s) would need to be reviewed to determine what type of hernia repair was done and if there is any synthetic mesh in your abdominal wall.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m 25 and have one child, I would like to have breast implants but I’m afraid the cost and recovery time is too long. Can you give me any advice and info on the payment plans and the recovery times. Thank you.
A: Cost and recovery are always the biggest issues when any women is considering getting breast implants. So every potential patient has to contend with these issues so let me discuss the facts on both of them. The recovery from breast augmentation is really a physical therapy one since the implant is placed under the muscle. (in reality, partially under the pectoralis muscle) So how does one recovery from a muscular injury…use it! I place all patients on arm range of motion exercises the night of surgery and no physical restrictions thereafter. The more you use your arms (within reason) the quicker you will recover. With there be discomfort after surgery…absolutely, but most patients do not find it severe enough to be very limiting for very long. I would have to know what type of work you do to better answer how many days you would need to return to it. From a cost standpoint, the issues are the type of implant where does one get financing to do it. Saline breast implants are the most economical and we have all of our patients use Care Credit for financing. They are a national company that we have found to be the best to work with and has the greatest option of repayment plans.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am curious to the cost of Botox in specific areas on my face. My biggest issue is my eyes as I am only 31 and am very attractive and often to I don’t look my age but I’m feeling as though I’m beginning to these days :-(. Also, am interested in the cost of breast augmentation. Thank you
A: Thank you for your inquiry. When it comes to Botox, the cost is completely related to the number of units delivered. Such units are usually very consistent for the area treated and so the cost can be well estimated. For between the eyes (glabella), which is the most popular area on the face for Botox injections that will take 20 units with a cost of around $300. For the crow’s feet area (beside the eyes) the number of units usually needed is 16 with a cost of around $225. When the two are done together, the total units can be reduced to 30 with a cost of around $425. For breast augmentation the cost is completely related to the type of implant used. Total surgical costs for saline breast implants is around $4700 while that of silicone implants is around $5800.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am looking to have breast implants, rhinoplasty and mentoplasty. (no implant) Do you offer mentoplasty? If so would I be able to do these 3 procedures at once or if not I would wait to do the implants. I can send some detailed pictures if needed.
A: Thank you for your inquiry. You certainly can do breast augmentation, rhinoplasty and chin augmentation all during the same surgery. When you refer to a non-implant mentoplasty, I assume you are referring to a sliding genioplasty in which the chin bone is moved forward. That accounts for about 25% of all chin procedures that I do so it is a chin augmentation technique in which I have great familiarity.
To help prepare accurate quoting, please send me some pictures of these areas so I can see exactly what needs to be done and the time it takes to do it. This is most relevant for the nose as there is great variability in rhinoplasty surgery depending upon how much of the nose structures need to be changed.
Once I have received the photos, I will do some computer imaging for the nose and chin and have my assistant send you a collective cost quote.
Dr. Barry Eppley
Indianapolis,Indiana
Q: Dr. Eppley, I am interested in getting breast implants. I am trying to find out pricing on getting implants and to see about payment. Most offices require full payment, however, I have heard of a few that will do payment plans. I didn’t know if this office was one of them?
A: When it comes to elective cosmetic surgery, including breast augmentation, you will find virtually no plastic surgery practices that take payment plans. A plastic surgery practice is not a bank or a credit agency that has any ability to finance and ensure that payments are received over time on a non-returnable service like surgery once it is provided. Full payment is required in advance of the actual surgery date. However, every plastic surgery practice recognizes that many patients can’t pay the full fee up front and work with independent loan agencies that do provide financing. One of the most common cosmetic surgery financing companies is Care Credit. You can go online with the amount you need to finance and apply and qualify. You can choose from a wide variety of terms up to 36 to 48 months. Many patients opt for the interest-free financing which extends out to 6 or 12 months. Our office has worked with many lending institutions over time but have found none that are as easy to work for our patients as Care Credit.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am getting breast augmentation next week and I can’t decide between two breast implant sizers. I am 5’ 6” and weigh 135 lbs. I am currently an A cup but lost much of my original volume due to children so they are flat with some loose skin. I am torn between 450cc or 500cc silicone gummy bear breast implants. They are going under the muscle so I am wondering if more volume is needed because they will be covered by more tissue. I don't want to look too big in my clothes but do want to have a wow factor without my clothes 🙂 Also, I hoping to achieve close to a full size D cup and I know if 450cc or 500cc will get me closer that. What do you think?
A: The difference of 50cc between breast implant sizes in the 500cc range is very small as that constitutes less than a 10% volume difference when you do the mathematical ratio. That is barely if at all visible. But in the debate between these two sizes, you have stated several important factors that make it clear to me as to which is best for you…the desire for a full D cup, wanting a wow factor and the very fact that you are asking this question. These suggest that you are afraid of not being big enough. In addition you have a lot of loose skin on your breasts of which it always take more volume to fill them out. Therefore, between those two sizes I would opt for the slightly larger one and choose the 500cc implants.
Dr. Barry Eppley
Indianapolis,Indiana
Q: Dr. Eppley, I am wondering if I should be at my ideal weight before having breast augmentation?
A: In regards to getting breast implants and your ideal body weight, I think that answer depends on how much weight loss you are anticipating and what your breasts look like now. If you plan to lose a lot of weight (greater than 20 to 25 lbs) and you have some significant breast sagging, then you may be wise to wait until you achieve that weight loss. You do not want to put in implants that will later develop additional breast sagging as the weight loss may cause the breast tissue to slide off of the underlying implant support or ledge, maing the sagging look worse. Also additional weight loss may tip the balance between a marginal breast lift candidate with their implants versus someone who definitely needs a lift with their implants. If the breasts have little to no sagging and the desired weight loss is fairly minimal, then you could proceed with breast implants at any time.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am 5’9” weigh 146 pounds and am a 36D. I had breast implants that were placed three years ago and were 500cc moderate silicone gel implants. Although I like the size, they look flat to me. My breasts are very wide and require a push up bra, otherwise they look flat in my shirt. They have given me reasonable cleavage but they are just so flat. What is the best way to improve their shape? What type of new implant do I need?
A: Moderate projection/profile implants have the lowest projection and widest base of any of the breast implants. Because they are so wide, I actually never use in my breast augmentation patients. Changing breast implants to a more narrow base with higher projection seems logical. It would also be important to go up in volume somewhat so you get more outer and upward push of the breast mound. Therefore I would change to a high projection implant with a volume of 600ccs. This will provide more upper pole fullness and may even narrow your existing width somewhat. With your body frame, a 600cc implant would not be much bigger than your existing breasts…just more towards the shape you want.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like a consultation for a breast augmentation. I have pectus excavatum and didn’t realize this until early adulthood. At this point in my life I would prefer cosmetic surgery as opposed to a more invasive surgery to correct my deformity.
Thank you and I look forward to hearing from you!
A: Breast augmentation can do a good job of masking/hiding minor to moderate degrees of a pectus excavatum deformity. When the chest plane is fairly flat with minimal breast mounds, a inward curvature or depression of the sternum (pectus excavatum) can be very noticeable. One would think that increasing the size of the breast mounds would make the sternal depression more obvious…but it doesn’t. Conversely it has the opposite effect and makes it ‘disappear’. This is because enlargement of the breast mound with an implant pushes up the inner aspect of the breast mound and part of the skin that makes up the edges of the pectus deformity. With two mounds emerging right next to the sternum, the deepest part of the pectus deformity now creates a natural cleavage effect and the sternal depression has now ‘disappeared’.
Dr. Barry Eppley
Indianapolis,Indiana
Q: Dr. Eppley, I came across your site, and was looking through the breast augmentation surgery, the results look really great. I’m a transsexual, I do have some breasts after being on hormones for about 4 years, and I was wondering would it to be too hard to do breast implants to someone who doesn’t have a whole lot of breasts?
A: If you look at a lot of breast augmentation results, it will become apparent when seeing before photos that many patients have little to no breast tissue. In fact, many of the best breast augmentation results come from those that have little breast tissue and nice taut skin. In such patients the resultant breast mound from implant placement attains a nice round shape. As long as the implant size chosen is not too big, the breast shape will not look unnatural.
In short, it is not difficult to place breast implants when there is little breast tissue present. This is what is commonly seen in many patients. The partial elevation of the pectoralis muscle with the overlying skin provides adequate space for almost any breast implant size. The limits of breast implant size is the base diameter of the chest/breast. As a general rule, it is good practice to match that diameter with the base diameter of the implant in each patient.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have interested in getting breast implants and have been researching the topic for the past six months. I have been to several consults and received differing opinions as to breast implant size. One surgeon even showed the result of an ‘extreme breast augmentation’ which frightened me. I take pictures of what I want into the consults but how do I know that is what implant size they will use? Some seem to listen to me while others I don’t think are and I am afraid they will just put in what they want.
A: Every plastic surgeon has their own approach to choosing breast implant size. Presumably the size selection should be what the patient wants. In my opinion, within reason, one should try and get as close as possible to the patient goal by using pictorial help. In the end it is not really about volume in ccs or bra cup size but what breast look the patient wants. With few exceptions, just about any implant size can be put in most patients. I find pictures very helpful as I use them in the OR as a visual guide with the initial placement of sizers, only pulling the sterile implants once the breast looks like the pictures with the sizers in place.
There is a definite trend today, used by some plastic surgeons with great rigidity, that they will not place breast implants ‘that exceed the tissue support to sustain them’. That is a bit of a subjective assessment but what it means for some patients is that they will get smaller breast implants than they really want. While smaller breast implants are often associated with fewer long-term problems than larger ones (tissue stretch and sag), it can be a delicate balance between meeting the patient’s goals and keeping the implant size from stretching the breast tissue too much. I would sit down with the plastic surgeon in which you are most comfortable and put your objectives and concerns on the table for an open discussion.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have been researching doctors for breast augmentation this fall. I am interested in breast augmentation and was wondering what your philosophy is about going big enough but not too big for your body. I am an A cup and would like to be a D cup. Another doctor told me a DD would put my body at significant risk for re-operation. My biggest fear is a doctor not letting me go as big and I would like or not setting the limits for too big and my body being injured. Thank you for your time!
A: Selecting breast implant size is, by far, the most discussed patient issue in the breast augmentation procedure for understandable reasons. The whole purpose of the operation is to get a larger breast size. I do not choose what size implant any patient should have, I merely help the patient select a volume that matches their desires. There is no absolute science to selecting breast implant size but through experience and the use of shaped sizers, I found that the desired result is obtained in just about every patient. I personally have never had a patient who has undergone a reoperation to get a larger breast implant size because they didn’t get what they wanted the first time. Conversely, I have had a few patients that opted for bigger implants but it was because they chose a smaller size initially.
When it comes to size selection, here is definitely a growing trend and philosophy amongst many plastic surgeons to place implants whose size stays within the existing breast base diameter and does not exceed the ability of the breast tissues to support it long-term. When you look at the relatively high rate of breast implant revisions (nationally around 30% in the first three years after augmentation…my practice revision rate is less than 10%) it is understandable why a more conservative size approach has become popular. While the need for revisions comes from a lot of different reasons (infection, hematoma, implant failure, etc), very large implants potentially contribute to these causes. ( e.g., due to bottoming out, asymmetry, symmastia, breast tissue thinning ,etc)
What defines a large breast implant size or too large of a breast implant for the patient is going to be different based on each patient’s breast anatomy and chest/body size. For most patients, I would not think that going from an A to a D cup would constitute in my mind an implant that is too large or, more relevantly, places the patient at a substantially increased risk of subsequent breast tissue support problems. But that would have to be determined by an actual physical examination of the patient.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a breast augmentation done seven years ago. Just last week I had a deflation and went back to my plastic surgeon. I am having both redone due to wanting to go fuller. I was an A cup before first surgery and now a C cup using a 350cc MP saline implant. I want a full D and he suggested a 550cc HP saline implants. I am m looking for a much fuller breast with less sagging. I want to make sure that when I go through this again that I get what I want. Does this size implant sound like enough?
A: When changing breast implant size to go bigger, you want to make sure that you are getting at least a 30% to 40% increase over your prior implant size. Anything less will likely not be that visible. That means going from a 350cc implant, you need to go at least 150cc bigger if not more. Thus the 550cc implant size sounds good to me. I have no doubt you will be visibly bigger and rounder. Whether your sagging will be improved to your liking, however, may be a different matter. Getting bigger does not always mean your breasts will be more uplifted, as defined by the nipple getting higher and more centered on the breast mound. Make sure you discuss this with your plastic surgeon beforehand to be certain you may not simultaneously benefit by some form of a nipple (areolar) lift with your breast implant exchange.
Dr. Barry Eppley
Indianapolis, Indiana
Q: I am interested in getting breast augmentation. At 25 years of age with one child I have a height of 5’ 3” and a weight of 137 lbs. What size breast implants do you think I need? I have attached a picture of my breasts to help you decide.
A: In looking at your breasts, your most important decision about breast augmentation is not what size implant should be used. You have a moderate degree of breast sagging, meaning the position of your nipples is at or below your lower breast fold. Contrary to the perception of many, breast implants will not have a breast lifting effect. You are in need of some type of a lift if you are going to get breast implants. With implants alone your sagging breasts will be pushed lower, a look that I doubt you will find as an improvement. All breast lifts result in some scarring, a definite cosmetic liability. Whether larger and more uplifted breasts are worth the scars as a trade-off is what you need to think about first and foremost.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am going to get breast implants and have had several consultations. One confusing point for me is whether the implants should be above or below the muscle. Of the two consults I have had one says above the muscle and the other is adamant that they go below the muscle. What do you think?
A: There are is no absolutely best position for breast implants in any particular patient. There are advantages and disadvantages to both approaches. The vast majority of patients today have implants placed beneath the muscle for better pocket stability, a more natural look (upper pole shape), better tissue coverage, a lower rate of rippling and less interference with mammograms. The one downside to under the muscle is that there will be animation deformities, meaning the implants will be pushed to the side unnaturally with pectoralis mucle contraction when the arms are extended. The one benefit to an implant being above the muscle is when there is some breast tissue sagging, it can fill out the sagging tissues better. The other under the muscle benefit is for someone who was looking for less recovery time and pain and could not avoid adjusting their fitness regimen or someone who has to have the procedure done under local anesthesia for medical and fear of anesthesia reasons.
In the end, one has to weigh these advantages and disadvantages from the perspective of their own breast anatomy and shape. As a general rule, always remember that any implant in the body always does better in the long run (i.e., less complications) when placed under a thicker soft tissue cover particularly when under well-vascularized muscle.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 38 year old mother with 3 children. Needless to say, three pregnancies and breastfeeding them all has taken qute a toll on my body. It looks like the proverbial life has been sucked out of me. My breasts are flat and droopy, I have a small skin amount of belly skin that hangs over my waistline and I recently found out that I need a hysterectomy due to chronic bleeding. Other than these issues, I am actually in good health. Since I have to have a hysterectomy anyway, I thought that getting breast implants and a tummy tuck at the same time would be a good idea. It would be great to get a while new body along with fixing my gyn issues. Do you think all of this can be done at one time and is it safe?
A: Combining breast augmentation and a tummy tuck with a hysterectomy procedure is perfectly safe provided you are in good health and have no significant health risk factors such as smoking, diabetes, or high risk for blood clots. Tummy tucks and hysterectomies are very commonly done together as it provides unparalleled access for the Gyn doctor to do the hysterectomy and provides solutions to many body problems in one operation. Adding a breast augmentation to this combined abdominal procedure does not add significant operative time, risks, or recovery. This would be the ultimate ‘Mommy Makeover’, correcting all issues that are associated with one’s pregnancies. Your most challenging aspect in getting this done is to be able to coordinate a plastic surgeon and a gynecologist’s schedule as well as the economics of doing it in a hospital environment.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, when I was a kid I had a problem with my blood platelets. The same thing happened after delivering my first baby and then with the second one nothing happened. Do you think that having breast implants will affect my platelets? If yes, by how much percent? Thanks.
A: Without knowing what your exact platelet disorder is or was, I can’t say with any certainty. You will need to better describe medically what your platelet problem was. There is a big difference between too many platelets, too few platelets, and platelets which just don’t work well as it relates to undergoing.The only thing that really matters with breast augmentation, or any surgery for that matter, is whether you have adequate clotting capability. If there is any question (and it sounds like there is) you should have a bleeding time, PT, PTT (or INR) and platelet count checked before surgery. Given that you had some type of ‘platelet problem’ as a child and after your first pregnancy, you should have a coagulation work-up before any elective plastic surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a breast augmentation done in November last year. Initially I was very satisfied with the results but now they are starting to sag and I need a breast lift. I remember that I had a discussion with my plastic surgeon before the surgery about doing a lift at the same time as my implants but I decided against it because of the scars that would result. Now that I am ready for a breast lift will I have to have the implants removed, have the breast lift performed, and come back at a later date for new implants? Or can the lift be done with the breast implants in place that I have now?
A: Many times modestly sagging breasts get by initially with implants alone. But when the breast tissues relax after being pushed outward, they slide off the implant creating ptosis off of the edge of the implant. If you are happy with the size of your implants and they are in good position, I see no reason why you can’t proceed forward with the lift with the implants you already have in place. Most likely, you will need a vertical breast lift to get the breast tissues up in proper position over the implants. While it is never a pleasing revelation that you will need a second surgery to get the breast result you want, take solace in the fact that a breast lift is much easier to go through than the initial breast augmentation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello! I am 31 years old and I used to be 375 lbs until I had gastric bypass surgery two years ago. Today I weigh 157 lbs, but now I suffer from loose skin on my abdomen, arms, buttocks, and thighs. I have a “skirt” of abdominal skin that reaches down to my groin area, and I suffer from irritation, yeast, and sores due to this excess skin. My breast size also went down significantly. I currently am on Medicare and Medicaid, and I was wondering if you offer a procedure that can remove this abdominal “skirt” that is covered by Medicare. Furthermore, I am also interested in getting a breast augmentation, and was wondering if my Medicare will cover it if it will cover the “tummy tuck” surgery. Thank you, and I look forward to your response!
A: Thank you for your inquiry. While you would do well with a circumferential body lift or even a frontal abdominal panniculectomy, I am not a Medicare provider so I can not be of assistance to you.
While there is the chance of some coverage by Medicare for an abdominal panniculectomy, there is no chance that they would ever cover a completely cosmetic procedure such as breast augmentation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in breast augmentation. Iwant fuller breasts to eliminate the stretch marks and I would like to go one size bigger. I am a size B now. I have attached pictures so you can see what you have to work with.
A: Thank you for your inquiry and sending your pictures. I can see your concern about breast size and there is no question that implants would be beneficial to get you from a B cup to a C cup. However, no amount of increase in breast size will eliminate your stretch marks. With the expansion of skin from breast implants, stretch marks may become somewhat less noticeable as they are pushed out and stretched flatter. But the concept of stretch mark elimination should be erased from your mind as an expected outcome. The one concern that I have about your breasts is what degree of sagging they may have. The pictures are taken with your arms up which artifically lifts them and may camouflage the actual amount of sagging. Breast implants do not lift sagging breasts which is a common misconception. So whether you may or may not need some form of a breast lift with your implants remains uncertain. When you have the amount of stretch marks that your breasts do, this adds to that concern. If you can send me some new pictures with your arms at your sides, that would help answer that question.
Dr. Barry Eppley
Indianapolis, Indiana
When the subject of breast implants or breast enlargement surgery comes up, many people immediately think about size. Large breasts that create eye-catching cleavage are what comes to many minds, a concept that has not been helped over the past two decades from celebrities ranging from Pamela Anderson to Heidi Montag of more recent note.
The reality of breast implant surgery, however, is far from this image. There are certainly a minority of women who do want this look. But the vast majority of women who choose to have breast implants are much more interested in finding the right size for their body and not to have overpowering breasts that become the focal point of their appearance.
Most breast augmentation patients are average women who simply want to look good in clothes and sport attire. I have seen many women who have told me that they are embarrassed to wear a bathing and won’t go to the pool or beach with their family. While breast underdevelopment is the most common motivation for getting implants, there are numerous other reasons. These include such breast conditions as postpregnancy sagging, asymmetrical breasts, body proportioning, breast asymmetry and reconstruction after mastectomies.
Pregnancy and nursing can have an adverse effect on a woman’s breast shape and size causing sagging and, almost always, a change in the amount of breast tissue. Many women are unaware that it is completely normal to lose breast tissue after pregnancy, a phenomenon known as involution. For some women who have had multiple pregnancies, they lose all of the breast tissue they originally had. When combined with stretched out skin, the change in a woman’s breasts can be deflating for their self-image as well. These are women who simply want to return to their pre-baby size and shape.
There are many women who have breast asymmetry where one breast is larger or different in shape than the other. In some cases the breast size difference can be as much as a cup size, sometimes even more. For women so afflicted, finding a bra to fit comfortably and properly is not as easy as going to Victoria Secret’s and pulling a good fit off the rack. Often they are forced to add padding to create a more even look in their clothing.
One of the most recognized and easily understandable reasons for implants is in breast reconstruction. The physical and emotional devastation of going through any form of a lumpectomy or mastectomy procedure can be softened knowing that an immediate or even a delayed reconstruction can be done. While numerous forms of breast reconstruction exist, including flaps that form the breast mound out of your tissues, implants remain the backbone of how most breasts are recreated.
Dr. Barry Eppley
Indianapolis, Indiana
A common question that some women face today is…are they for real? With more women than ever undergoing breast augmentation, this is not a far-fetched question. It may be inappropriate to ask but the statistical reality is one may be more right than wrong many of the times. According to statistics from the American Society of Plastic Surgeons, the number of women who have had breast augmentation had risen nearly 40% over the past decade. In 2010, nearly 300,000 American women received cosmetic breast enhancement.
One other trend in breast augmentation is a noticeable size difference. Many plastic surgeons have commented that women are asking for bigger breasts than they were a decade ago. Historically women would usually ask to go a cup size bigger. Today it is not uncommon for a women to want two or three cups bigger, particularly the younger they are. Women state they want to get a good value for their investment and they want to make a noticeable difference in their clothed appearance.
What accounts for these trends in breast augmentation? By far I would say that it is simply more accepted than ever before. As we enter the upcoming decade of 2010 to 2020, this is the beginning of the third generation of women who have had access to breast implants for cosmetic enlargement. It is a normal part of society now and younger women’s mothers and soon grandmothers will have had the procedure.
Breast augmentation has a track history of safety as well as effectiveness. Despite the hullaboo of what transpired in the early 1990s, the procedure has been proven to cause no medical problems or makes people systemically sick.. While it is far from a perfect procedure, because after all it is an implant in the body, its complications are local in nature and often aesthetic in significance.
The social trends of today play a major role in its popularity as well. Just go through the checkout counter at the local grocery store and the magazines are full of articles about celebrities who have had or are assumed to have had some form of plastic surgery. Many of these are women actors and performers who have enhanced their top half. The influence of these magazine, TV shows and now the internet have made it seem that having breast enhancement is now the new norm.
There are more choices in breast implants today than ever before. Since 2006, both saline and silicone implants are available in not only differing sizes but projection and styles as well. With the potential for gummy bear breast implants to be available perhaps later this year, increasing implant options appeal to an even broader spectrum of women. Just like the many aisles in a drugstore, multiple options for a single product line result in more sales.
The rise in breast augmentation is a result of greater societal acceptance, safety of the devices, influence of famous people, and a wide variety of implant options. I suspect the upcoming decade will see the number of implanted women continue to rise.
Dr. Barry Eppley
Indianapolis, Indiana
Q: I am going to get a breast augmentation next month. I am 23 years old. My plastic surgeon never mentioned or suggested about getting a mammogram before surgery. I have read that some plastic surgeons require it while others do not. What is your recommendation?
A: Whether a mammogram is needed before breast augmentation has no uniform answer. Every plastic surgeon has a different perspective on this issue. My practice is to not get a mammogram under the age of 35 unless there is a family history of breast cancer or a history of breast problems such as cysts or fibromas. While breast cancer does rarely occur in younger patients, the statistical likelihood of a young patient having it is so low that I do not feel that the extra expense and radiation exposure justifies the effort. After age 35, I follow the recommendations of the American Cancer Society in regards to a baseline mammogram and subsequent studies. Some plastic surgeons routinuely get mammograms regardless of age before breast augmentation and this is a perfectly valid approach as well. You need to discuss this issue with your plastic surgeon and reach a mutually acceptable approach to the need for this presurgical breast screening study.
Dr. Barry Eppley
Indianapolis, Indiana
Q: I would like to know some information for breast augmentation. Specifically I need to know about the recovery time as well as any long term problems associated with breast implants.
A: Depending upon what kind of work you do affects recovery time after breast augmentation. For a less active sit-down occupation, one could return to work with 5 to 7 days. For more physical or strenuous activities, it may take 10 to 14 days until one is completely comfortable with those efforts. There are no restrictions after surgery other than one’s level of comfort. I place my patients on range of motion arm exercises beginning the first night after surgery. The more and the sooner you move your pectoralis muscles, the quicker you will recover and feel better. Breast augmentation is essentially two big pulled muscles. Like rehabilitation from any muscular injury, early active range of motion is important.
While breast augmentation is exposed to all of the traditional risks of surgery (infection, bleeding), those risks are relatively small. The biggest concept to grasp about breast augmentation is that it is an implant-driven operation…meaning that most of the risks long-term are related to having an implant. One has to recognize that the implant is not going to last forever, they will eventually ‘fail’ and need to be replaced. This is not a maybe, it is a certainty. It in just a question of when it will occur. On average, many patients experience 10 to 20 years of use before replacwmwnt of one or both becomes necessary. So one needs to bear in mind that all breast augmentation patients will over their lifetime have more than just the initial placement surgery.
Dr. Barry Eppley
Indianapolis Indiana