Your Questions
Your Questions
Q: Dr. Eppley, Was curious if high scrotal is possible compared to mid raphe for same low hanging effect, I heard high scrotal has low pain after and fast recovery. Whichever has lowest extrusion rate and least pain is preferred, other than inguinal.
Also, can you ask implantech for durability testing data? I’m curious how resilient the shape of these are after being compressed I am extremely active. This is important for me to know for peace of mind.
A: When it comes to an incision, not matter where it is placed, what is done inside remains the same. Thus an incision is a point of access and is not where most of the discomfort emanates.
The midline low raphe incision has the least discomfort and ensures the best chance for a desired low testicle implant position. I have never seen extrusion and would not consider it a likely risk. That would occur due to the combination of an inadequate implant pocket and poor wound closure techniques.
There is no biomechanical data that I am aware of that would provide what the required amount of compressive force that it would take for the implant to fracture/fail. But I would suspect it is way beyond twhatever force to which you are going to expose it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello My interest is about entire midface augmentation. My wish is to avoid implants. want to try with hydroxapatite. I want to ask 3 things:1. Is it possible to use hydroxyapatite cement to augment complete midface
2. Is it possible to insert around 4 mm in thickness augmentation
3. Does it last forever or will it shrink over time. How l8ng will it stay is there any research on that
Many many thanks
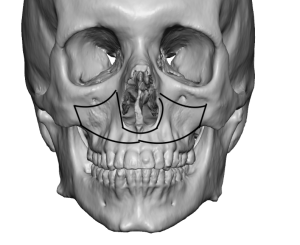 A: Hydroxyapatite (HA) bone cement can be used to augment the midface as long as one understands what its coverage and augmentation limitations are. (see attached) It is a difficult material to use in the limited access than the intraoral incisions provide being an intraoperative putty that must be allowed to be placed, shaped and given time to set which requires a completely dry environment. As a result it works best in concave bone surfaces where it is more contained. A 4mm augmentation should be able to be achieved in the deepest part of the augmentation over the face of the maxilla.
A: Hydroxyapatite (HA) bone cement can be used to augment the midface as long as one understands what its coverage and augmentation limitations are. (see attached) It is a difficult material to use in the limited access than the intraoral incisions provide being an intraoperative putty that must be allowed to be placed, shaped and given time to set which requires a completely dry environment. As a result it works best in concave bone surfaces where it is more contained. A 4mm augmentation should be able to be achieved in the deepest part of the augmentation over the face of the maxilla.
Also HA is a structurally stable material that does not shrink or change structure over time. There are certain types of HA that are resorbable but when made as a bone cement they are non-resorbable.
HA cement has appealing biologic properties but it does not have the same surface areas of coverage or increases in projection that implants do.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in clavicle shortening. However, I play ice hockey at competitive levels (no checking but certainly a lot of hard contact) and would be interested to know what would be the appropriate expectation in terms of how long it would take to be able to play safely again (if at all).
A: That is a good question and not one I have been asked before. My best guess would be 4 months or more after the surgery such sporting activity may be considered. With the plates in place it should take trauma just as well if not better than the natural clavicle.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have questions on rib narrowing. I saw you on the Doctor’s Show and you said u can take out #11 and #12 and 10# and 9#. If you take me on as a patient is it possible for you to remove #12 #11 #10 #9 ribs?
A: In rib removal surgery for waistline narrowing I always take ribs #11 and #12 and sometimes rib #10 if the pleura of the lung is not attached to it. But you can’t take rib #9, its is too far from the incision and almost assuredly has pleural attachments. That I have never done for waistline narrowing.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I think I do have the same case mentioned in this article. My brow bones did grow naturally but I think it has a trauma history that there was once a broken branch that hit my head near my eyebrow that caused that side to grow more. I’m wondering what could I possibly do.
A: I believe you are referring to a one-sided brow bone hypertrophy or protrusoin. This can be reduced using either a bone burring reduction or a bone flap setback technique depending on how thick the anterior wall of the frontal sinus is. But the first step is to get an x-ray to evaluate the frontal sinus development and the thickness of their anterior wall.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a 29 year old male interested in getting a surgery for skull reshaping + temporal reduction. The shape of my head has bothered me for over 15+ years now. I’m aware the trade off for such a procedure includes scarring and I’m perfectly fine with that. The width (shaped like a balloon), prominent sagittal raised area, and size of my forehead are the main concerns. My hair is thinning, which doesn’t bother me, and I have no interest in altering my hairline or getting a future transplant. I’m curious to see if this is something you guys can help out with or if I have unrealistic expectations of what can be done. I will keep this short until then. Thank you for your time and consideration.
A: Thank you for your inquiry and sending your pictures. The temporal reduction and sagittal ridge reductions are very straightforward, effective and will certainly be winners for you. (see attached) The more dubious one is that of the forehead. It is dubious as I am uncertain as to what exact aspect of your forehead you see as too big (upper bossing??) and, while you may have no concerns about scars at least for now, I do and I would be cautious about scars and their visibility when doing procedures are the forehead. Such forehead procedures in a shaved head are not as assured winners as the other ones where the scar tradeoffs are so negligible they are virtually irrelevant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Would a lateral commissuroplasty give me a better smile? I believe I have a forced smile because of my small mouth.
A: A lateral commissuroplasty or mouth widening procedure would certainly increase your mouth width which, when the dynamic action of smiling occurs, will give it a wider or more evident smile. It can also help turn up the corners of the mouth a bit which I think is what really makes a smile better more so than just width.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have had a flat head my whole life. It is really bad on the right side profile but on the left side it is a little bit better. Do you think that can get fixed? And if you put an implant will there be a scar on my head? Does the scar heal and the hair grows back to normal?
A: Asymmetric flat back of the heads are very common to which a custom made implant from the patient’s 3D CT scan works well to optimally address the problem. It does require a small incision to place low on the back of the head which scars very well and usually causes no problems with hair growth.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to have a consultation to reverse my genioplasty. I believe my face is too long now.
A: Your sliding genioplasty can certainly be partially or totally reversed. My questions would be:
1) How long ago was your genioplasty procedure?
2) What type of movements were done? (e.g., how far forward was it moved?)
3) Do you have any postop x-rays?
4) If vertical length is the issue but not the amount of horizontal projection then the vertical length may only need to be changed.
The point of #4 is I would be careful about fully reversing a sliding genioplasty as the chin is not going to return completely to what it was before the surgery. There are going to be some changes that will be the result of the stretched tissues. (e.g., increased submental fullness) As there was a reason you had the original surgery I would think about keeping the benefits and eliminating the liabilities. (vertical length)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a question about the sliding genioplasty. For a patient with no lower lip incompetence, can a large sliding genioplasty (12+mm and a few millimeters vertical) cause lip incompetence? Would a movement like that not stretch the skin and pull the lower lip down?
A: Such potential lip incompetence (lower lip pulldown) would not come from the bone advancement per se. But if the large bony stepoff is not grafted with the advancement there is a real risk of soft tissue contracture into the stepoff resulting in lower lip tightness and potentially lower lip retraction.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Do silicone implants for skull reshaping need to be replaced at some point? What is their longevity and advantages over using PMMA? thank you.
A: Silicone skull implants are permanent, do not fail and never need to be replaced due to any material problem. Bone cements for aesthetic skull augmentation as far as I am concerned are of historic relevance…they have poor shape control, can only provide a very limited augmentation effect and are impossible to revise should that need arise. Like any preformed implant they have numerous advantages over any implant material that has to be applied and shaped during surgery through a limited incision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello I wanted to ask you about a procedure and if you could do it. A reduction in the red marked areas of the pictures I will send.
I want to achieve a very small correction and reduction and to make them even. I read about zygomatic reduction but I dont want the ones that is popular in Korea where they cut the bone and reposition it.
I think only a shaving of Zygomatic arch is what I am looking for but I am not sure. I will attach some pictures for you to see. The red marked area is where I am talking about but more so the area between the Zygomatic bone and the ears which I think is the Zygomatic arch. That is where I feel it is a little wide and would want it to be more straight.
A: The zygomatic arch can not be surgically reached short of a full transcoronal incision…which no patient is going to do for aesthetic purposes. Furthermore the zygomatic arch is incredibly thin (1 to 2mms) so shaving of it is not possible. As a result the only way to move the zygomatic arch inward is by osteotomies which are done all over the world and not just in South Korea.
That being said when only a few millimeters of inward arch reduction is needed the isolated posterior zygomatic arch osteotomy done through a small sideburn incision works just fine.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Are there any damages of skull implants, do they make the hair sparse, this is very important to me.
A: I am assuming becaiuse you have provided side view pictures that your skull asymmetry is isolated to the back of your head??
Skull implants do not have any adverse effects on the skull nor do they affect overlying hair growth. It takes a very large skull implant to cause any increase in interfollicular hair spacing…an issue I have not yet seen or been reported to me.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, my forehead looks overly wide, compared to the bigonial width and the outer lateral orbital walls. From your experience (and I know it might differ for every human) what is the maximum safe reduction that can be done?
Also, from the side profile my forehead looks straight, from brows to the beginning of the hairline. Could the bony part right at the beginning of the hairline to be reduced as well? (downward direction)
A: The thickness of the bony temporal line is greater than that of the forehead bone between it….4 to 5mms can be easily reduced. The upper forehead at the transition of the forehead and top of the skull can also be reduced in the 3 to 4mm range.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, a general question possibly be answered before hand? Ive seen that you have performed submental chin tucks, but are you only able to achieve making the chin shorter, or can he also make it slightly more narrow? (Perhaps by extending out the incision?) I havent seen very many frontal views of these procedures he’s performed, mostly just side views so its hard to tell.
A: The chin can only be made more narrow by bone reduction. It requires a T-shaped submental excision pattern to have a soft tissue narrowing effect…which has its own aesthetic scar tradeoff.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, When do u put the device to hold the bone together in clavicle reductions for shoulder reshaping? Does it need to be removed or can it stay in for life?
A: The only reason to ever remove clavicle fixation hardware is if it becomes too visible over time (most common reason) or causes discomfort. (rare)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, do you offer custom pectoral implants?
A: For your left Poland’s chest deformity you would need a custom implant design which I have done many times. Most such implants are made from an external moulage technique which is done in the office. The other technique is to use a 3D CT scan which is very good for seeing the ribcage differences.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in a knee lift. Can the scar be hidden really well and made super fine? Do you have any photos of knee lifts after a year, after the scars fade? I always see pics with the scars red and the tissue swollen, I’ve never seen an actual year later or more pic.
A: While you are a good candidate for knee lift surgery (abundant suprapatellar loose skin that is thin) I would have concerns about the scar in your case. The patients who do best with knee lift surgery feel that they would rather have a visible scar than the loose skin…as opposed to a ‘hidden really well and a superfine scar’. The key is these decisions is while a beautiful barely seen scar is the goal in every patient such outcomes can not be assured particularly when the scar is exposed to significant knee flexion.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have recently received submalar implants in aim of more defined cheekbones, after which I recognized that a submalar implant would not achieve what I was looking for, after hearing about your work, I am looking to replace the submalar implant with a custom implant, I believe what I am looking for is something that defines the zygomatic arch and cheekbone. I would like to discuss this further with you to see if this is the correct path, hear your thoughts and find the best way to proceed.
A: If the goal is more defined male cheekbones, submalar cheek implants would definitely not be the implant of choice…nor would any standard cheek implant as that is not what they are designed to do. All of these implants are based one the historic approach to female cheek augmentation or an apple cheek fullness.
When it comes to custom cheek implants the first question is whether this is a cheek augmentation alone or a combined infraorbital-cheek augmentation. Since you havenot mentioned any issues relating to the undereye area I will assume until shown otherwise that it is the former. But pictures of you before your cheek augmentation as well as after along with pictures that show your ideal cheek augmentation shape goal will provide that clarification.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, What is the maximum size of custom jaw implants? How do the soft tissue in our face affect the size of facial implants?
A: This is not a question that can be answered in any meaningful general way. Such custom jaw implants are made individually for each patient, all of whom will have different dimensions throughout the implant design. As a result there is no way to describe them in sizes. Each patient will definitely have implant size limitations…but that has to be determined on an individual design basis and even then this is an estimate which can ultimately only seen when trying to surgically implant it.
The thickness of the facial soft tissiue will definitely influence how well the implant’s shape/features are seen. Thinner facial soft tissue thicknesses get better results in that regard that thicker fuller face patients.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi! I’ve been considering a chin reduction surgery for quite a few years now, but not sure what would work for me. I currently have a fairly defined chin, with a good shape EXCEPT for the vertical length. I used to have a very slight underbite as a child, but it was corrected early on so my bite is fairly normal however my chin is still a bit too long.
Im wondering if theres anything that could be done in my case to remove some of the vertical length. Im curious about how the procedure works, because in my mind, if you burrow down some of the bone, there should be an excess amount of loose skin that has been stretched to wrap around the original length of the chin?
Very happy to hear if any procedure could help me, what results i could expect, and how it would work.
A: The correct procedure in your case would be an intraoral vertical wedge reduction bony genioplasty. This technique which avoids the loose skin issue as the soft tissues remain attached to the inferior border of the chin and follows it up superiorly as the chin is vertically shortened.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can very high set zygomatic bones (pic) be achieved by combination of shaving off lower part of zygomatic bone and then placing infraorbital rim implant that extend into orbital rim(saddle). Also can zygomatic arch be made higher with custom implant?
Thank you
A: The zygomatic arch can be made wider but not necessarily higher… although an inverted tear drop shape to the arch component of the infraorbital-malar implant can probably achieve that desired effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Are there any dental concerns with a custom jawline wrap? From the photos of the wrap designs it seems like they are placed close to whether the tooth roots would be, could there be issues with tooth root damage, and if there is bone erosion will that be an issue with the teeth? Also where are the screws placed, would those be in danger of coming into contact with a root as as well? The same question applies to a sliding genioplasty, as the screws are placed close to the tooth roots, how do you make sure in surgery that the screw will not come into contact with the roots?
Ive also seen online that the jaw shrinks as we age, how would this effect the fit of a custom wraparound implant?
A: In answer to your custom jawline implant questions:
1) There are no dental concerns with such implants.
2) The tooth roots and most of the length of the inferior alveolar nerve lies within the mandiboe while the implant sits on the outside of the bone.
3) Bone erosion does not occur with jawline implants which is often confused with passive biologic implant settling. The tooth roots are not at risk.
4) Small 2.0mm titanium screws are used which penetrate 1 to 2mms into the bone, well away from the tooth roots and nerve.
5) The superior screws of a sliding genioplasty penetyrate into the outer cortical bone below the tooth roots of the incisors which have the shortest roots of any tooth in the enture dental arch.
6) The jaw only shrinks with age if some or all of the teeth are lost. It doesn’t lose bone mass because of age, it loses it because of loss of functional loading.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have just recently noticed that I have Plagiocephaly. From the research I have done it seems that I have a mild or type 2 form. I also have right-sided plagiocephalic head with slight difference in my forehead protrusion and cheekbone protrusion. The left side of my head is also a bit more slanted than the right. Firstly I was wondering If all these problems are fixable and how risky the procedure would be to fix this. Secondly I was hoping you could provide a cost range for this procedure.
A: All of the manifestations of plagiocephaly that you are describing which are common, mild as they may be, are improvable. When determining what should be corrected it comes to what are the most bothersome features of it. By your own description you have identified ipsilateral facial protrusion (with a flatter right back off the head) and a left forehead slant. The key question is not whether any of these features can be treated or that it is risky to do but which ones are most important. Patients rarely treat every aspect of their plagiocephaly but only the most significant features of them that bother them the most. Until I know what those features are in your case I could not say how it would be done or what the cost of such surgery would be.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Attached are various angles of my nose. The tip is what I’m really concerned with on how it arrows down- especially when I smile. Also I have a small hump in the middle to straighten. And from frontal view straighten a little as well.
A:The dynamic nasal tip ptosis occurs for two reasons, either one has a hyperactive nasals muscle and/or they have a natural 90 degree or less nasolabial angle nose to lip relationship. In your case that latter clearly applies making you more susceptible to a downward pull on the nasal tip.This is best treated by an open rhinoplasty where the tip position is rotated upwards a bit and supported by caudal septal resection and columellar strut grafting. At the same time the same nasal hump can be reduced.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello I was wondering about reduction of occipital area in the back of my head.I measured the area from top to bottom of the area I would like reduced and it measures 7 cm or 2.75 inches. I am aware you cant reduce much but if it can decrease it by a little I am happy.
– Do you think I would get noticeable results?
– Is it safe? Beside from infection whats the worst case that can happen?
– Can I do it and then go back home to Germany after 2 days?
– Will the scar be noticeable?
A: In answer to your occipital skull reduction questions:
1) You will get a noticeble change and if the goal is just to ‘reduce it as little’ you will definitely achieve that goal.
2) This is a perfectly safe procedure. I have never yet seen a complication from any autologous skull reshaping surgery.
3) You can return home after 2 days.
4) The small incision used to do the reduction usualy heals well and leaves a minimal scar.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,Among solid silicone, Medpor, PEEK, and titanium custom facial implants, which one can provide the most natural appearance?
A: All materials create the same external facial appearance. It is the design of the implant that will determine whether the change is natural or unnatural looking.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in getting custom jawline and midface implants with the aesthetic goals listed below. Are these goals feasible? Are there other procedures either instead of or in conjunction with custom implants that would better achieve these goals?
For context, I’m also considering septorhinoplasty at a later date to repair a deviated septum and resolve resulting issues with nasal asymmetry.
Midface
– Reduce dark circles and hollow appearance under eyes
– Correct negative orbital vector
– Augmentation of flat zygomatic arch with increased bizygomatic width (currently ~130 mm, ideally ~136 mm)
– Modestly increased malar projection
– Mitigate appearance of long midface and wide-set eyes
– Improve harmony with upper third (ideal bizygomatic width ~120% of bitemporal width)
Jawline
– Improved symmetry, correcting relative deficiency in right gonion (left side of the photo)
– Harmony with midface (ideal bigonial width 85-90% of bizygomatic width, currently 106 mm)
– Increased bigonial width with greater visibility of jaw angles
– Sharper, more angular, less rounded jawline
– A more square chin with increased width
– Marginally increased chin forward projection (ideally aligned with lips, currently ~3 mm behind)
A:While you list of aesthetic facial goals is long and comprehensive I don’t see that the majority of them could not be largely achieved with the use of custom midface and jawline implants…and that would be the only way to try to do so. The concept to the facial implant procedures is correct, its ability to achieve will be largely dependent on their designs. (shape, size and various thicknesses)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in a vertical lengthening genioplasty (vertical lengthening only). I’m including some photos of myself with notes.
Thank you.
A: Your chin is higher than your jawline because you have a flat mandibular plane angle. (or close to it) As you have drawn the vertical lengthening bony genioplasty is the correct approach to treat it. The only question is how much vertical lengthening is needed which in your case by your own drawing is in the 8 to 10mm range….which is best done by a vertical opening bony genioplasty.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I will be scheduling my surgery soon, but there is a question I had that came up. When you perform forehead reduction, will there be a chance for unevenness, or it is a smooth transition from the forehead bone burring to the rest of the skull? If my question makes sense.
A: Good question. Any form of skull reshaping (and the forehead is part of the skull) must be done with a smooth transition from one skull surface to the next adjoining one. This is important whether it is for augmentation or reduction purposes.
Dr. Barry Eppley
World-Renowned Plastic Surgeon