Your Questions
Your Questions
Q: Dr. Eppley, I managed to take a very symmetrical picture of my face and it shows that I definitely have vertical orbital dystopia, and not just facial asymmetry like I used to think. I have for a long while been conscious about my eye asymmetry so I’m wondering what the treatment could be? Thank you for answering.
A:To determine if and what surgery may be effective for VOD the workup includes a true straight on facial picture (not with the head bent slightly down) and a 3D CT scan of the face. Until then only the general concepts of VOD surgery can be discussed but not if it would be effective for you.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have large conchal bowl on both ears and this is something I don’t see many surgeons can correct, I believe it is because that scar it will leave due to the wedge resection. I don’t know how else the conceal bowl can be reduced but I wanted to see if the doctor could help as this is a concern that I’ve had for many years. I’m not sure if the photos show it but in person my conchal bowl is very large compared to the rest of my ear.
A:You have correctly surmised that only a mid-ear wedge resection can reduce the size of the concha and that the resultant scar to do so may not be a good aesthetic tradeoff. And should one find the scar undesired there is no going back as it is irreversible…so it is a big aesthetic gamble.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had 2 questions regarding the CMA and WMA implants. I was wondering what your thoughts on the CMA vs the WMA mandible angle implants were; I see they were both designed by you, however I saw previously you say you favor the WMA, and was curious as to why?
Secondly, when comparing both these implant types, which do you think offers more vertical projection? I know that these implants focus on the lateral projection, but that a small amount of vertical projection comes with horizontal focused implants. As such, would be curious as to which would help the vertical projection as well.
A:The two fundamental jaw angle implant styles are for different aesthetic effects, one for widening and one for vertical elongation. So it is not an issue of surgeon preference, it is an issue of what fundamental jaw angle shape change does the patient need/desire.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am from the UK you are the only surgeon I have found that thoroughly explains the different types of chin surgery and have so many amazing testimonials.
I am looking to horizontally reduce my chin protrusion. I especially don’t like how long it gets when I smile and gives me some chin ptosis.
Would I need: Submental technique for combined excision of horizontal bony excess and redundant soft tissue chin pad. With chin ptosis tuck
I worry that it will make the chin ptosis when I smile worse as I saw you mention that the chin ptosis tucks don’t always give long lasting results, so can it come back?
I also of course want a rhinoplasty, but don’t want this before I can get the chin reduction as my side profile would be off balance and it’s much harder to find a credible chin surgeon as it is less practised.
I have attached lots of photos. On the ones with before and afters I have edited the after images to give an idea of the desired result I would be looking for.
A:You have correctly surmised that most chin reductions, and particularly a significant horizontal reduction requires management of both the excessive bone and soft tissue chin pad. Thus only the submental chin reduction approach be effective.
I am not familiar with the statement ‘you mention that the chin ptosis tucks don’t always give long lasting results, so can it come back?’ as I am sure I have never said that. What I undoubtably said was when doing the soft tissue reduction it is impossible to know whether one is taking enough soft tissue off. Thus in 50% of the cases a secondary chin tuck and/or scar revision is needed to maximize the result.
I have attached your imaging that I think is reasonable and the other image which is not realistically obtainable.
It is also true that the nose and chin are linked. It would be aesthetically hard to just reduce one since the reduction of one makes the others prominence even more so. Whether they are staged or done together is a matter of personal preference.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Will implants give me a more defined look than the fillers I have used for jaw augmentation?
A:Fillers create soft non-defined soft tissue augmentations. Implants augment the bone, are deeper and are firm creating more defined external results. The effects of any facial augmentation depends on the materials used and their anatomic location of placement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m wondering what kind of surgery I should get regarding the “dent” in my forehead? A surgery that can totally remove it or reduce the “dent”
A:The dent in your forehead is caused by your very large brow bones, making the forehead above it appear deficient or indented. The question then becomes do you augment the forehead above the large brow bones or do you reduce the size of the brow bones. That would be up to our aesthetic preference and it requires side view picture imaging of both types of forehead changes so you can see what looks better to you
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have several lip and nose surgery questions.
Lips:
I want a lip lift upper and lower ones so they can look bigger because in real life they are so dry and they look small and the most important thing i want my mouth a bit wider than that because my mouth look so small in real life And please i want it to look natural just a bit of lifting so they can be a bit bigger and the most important thing wide lips and natural look
Nose:
My goal is i want to fix my nose but i want it to look masculine and natural . I want to remove Droopy tip and remove this one but pls i want an natural and masculine transformation
A:The key to any facial procedure in looking natural is to not overdo it. In regards to surgical lip lifts and advancements a few millimeters of skin removal creates improved vermilion show (fullness) without looking overdone or unnatural. With tip ptosis and a less than 90 degree nasolabial angle your nasal tip needs to be lifted to the 90 degree angle range, correcting the sagging tip but still looking like a male nose.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I am interested in getting surgery on my whole face so I can have the same facial features as the photo of that guy with earphones. The first photo is a photo of me and I have also attached a photo of the same guy wearing a suit which is what he looks like before surgery and I am trying to do surgery on my eyes, nose, jawline, cheeks and chin so I can look the same as the photo of the guy with earphones.
A: In terms of face makeover I would be cautious about using the term ‘look like someone else’ …as that can never happen exactly as the starting points are different (your face vs the model) and the model face as the advantage of a photoshopped professionally done image. So the question is not whether surgical face changes can be done but whether an approximation of that type of facial shape can be achieved. The challenges as I seem them in that regard in so doing is in the eye area.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is it possible to move the inner corner of the eye without orbital floor augmentation? I think my asymmetry is the most noticeable with the right inner corner being higher than the left. Also is the orbital floor augmentation safe (no risk of going blind)?
A: Inner eye corners can be lowered or raised using a Z-plasty tissue rearrangement technique.
There is no risk of blindness with anterior orbital floor augmentation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Attached are the pictures that you requested of my hips. Please let me know if it would be possible to get the customized hip implants placed in. I was wondering if the doctor can have them plunged into my thighs as far down as possible to give me fuller legs as well.
A: Thank you for sending your pictures. Some basic concepts to be aware of with hip implants is the following: Hip implants have a fairly high rate of complications due to the more superficial tissue location in which they have to be placed so patients have to be selected very carefully to try and lower those risks. There are two major risk factors, 1) thin patients with little subcutaneous fat (inadequate soft tissue cover) and 2) implants that are too big. (too thick for the tissues to adequately support them) Both of these hip implant considerations are judgment issues with no absolute measurements to them.
As this applies to you….1) your hips appear to have a fairly thin subcutaneous layer despite the thick muscles of your legs. So unless the amount of hip augmentation is small there will eventually be issues with implant show. 2) Hip implants can not be extended into the thighs as those are two independent tissue planes. This is why hip and thighs implants are separate implant sites. 3) When a patient speaks oif having fuller legs this indicates to me their augmentation goals are not modest and, as a result, a high risk implant patient.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a Lefort 1 surgery which advanced my upper jaw forward by 7mm. This surgery made my midface soft tissues sag and feel empty. I suppose this is because the cheekbones were left behind.
My questions are : a) in order to fix this issue will cheek implants of 7mm thickness would be sufficient?
b) Generally, should the amount of augmentation in the cheekbone area be exactly the same as with the movement of the maxilla from the orthognathic surgery in order to fill out the midfacial tissues?
Thank you
A: In theory the augmentation of the cheekbones should be similar to the amount of LeFort I advancement…although remember that the maxilla is a pure 2D horizontal movement while the cheek is more of a 3D structure that is rarely changed as a pure horizontal augmentation. As a result the correlation may not be exactly 1:1.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m wondering if you can advise or assist with an enquiry regarding forehead bossing. My daughter has been to see a professor in Harley st London as she has forehead horns which we were hoping would be able to be bossed as unfortunately they are a little prominent. She had a CT scan and as a result of those findings the conclusion was as follows:
Professor said there is an inner table defect of the calvarium at the centre of the area of bossing on the left side. The bone has thickness of 2mm while most of the bony lump is the adequate thickness of bone
He therefore told us he was unable to proceed with any procedures.
We were wondering if you think there is any way that you could offer an opinion as to whether there are any other avenues or ways forward with regard to this.
A: In my experience most forehead horns can be reduced and I have never gotten a CT scan beforehand. But since she has a scan it would be useful to see it to provide a more qualified opinion as to their reduction potential.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can you make my face more symmetrical? Specifically, the lower left side of my face is much less full than the right.
A: You have an inferiorly-based left facial asymmetry, which means the entire left side of your face is verticallhy short than the right with the jawline being the most affected. This extends up into the cheek and eye area but at that level it is very slight. (see attached grid)
Such lower facial asymmetries are treated primsrily by a left custom jawline implant to match the right side. There is a soft tissue component in the trampoline area (between the cheeks and the jaw) as well which can be treated by fat injections at the same time.
But the first place to start is to get a 3D CT face scan to see how different the two sides are from a bony standpoint.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am 6 weeks post-op following a 6mm sliding genioplasty. I think the swelling has almost completely subsided and I’m thrilled with the result. I saw literature online suggesting however that there can be a relapse of on average 1.5mm over the first year due to bone remodelling. I’m now worried that my chin will get much smaller (if I’m losing ~20% of the advancement within a year). Am I worrying about nothing?
A: You are correct…this isn’t a potential issue of which you should be concerned.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I was wanting to get an FUT hair transplant in May, then potentially do the type 3 brow bone reduction in November. If I did that, would it be a problem? For example, is it possible to get the incision site for the type 3 brow bone reduction to be behind my hairline?
A: It would be far more prudent to do the brow bone reduction first then the hair transplant…that way the hair transplants have no risk of being adversely affected and they then can more judiciously into and around the brow bone reduction scar.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have heard that the increased volume on the side of the head causes a negative canthal tilt. Is it true?Will my eye shape change after a head widening implant?
A: That I have never seen nor would it be anatomically possible. Whomever made that statement has absolutely no idea what they are talking about.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I did an implant on my back of head in 2017. Can you please check for me, is it a silicon implant that I have?? Do I also have two screws in there?
A:You are correct on both counts. You had a solid silicone skull implant placed back in 2017 which was secured with two titanium microscrews as seen both intaoperatively as well as on a postop 3D CT scan.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, When you say that the clavicle gets lengthen 20 mm does that mean that you are gaining 20 mm on the outside as well? If my shoulder width measured deltoid to deltoid is 47 cm does that mean that after the procedure my shoulder width would be 49 cm? I’m askin because I heard from another surgeon that you can lengthen the clavicle 2 cm but you only get 1 cm visually on each side.
A:That would be correct. It is not a 1:1 relationship as the surgery is performed on the inner 1/3 of the clavicle and the effect is sought at its outer third. The exact correlation is not known but it is fair to say it is better than 1:0.5, more likely 1:0.8.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I was wondering if you could help me find an answer to this question that I’ve been having. I’m going to need double jaw surgery at some point in the future to address my short face and bite. I have inadequate upper tooth show, and to fix this problem I may need a maxilla downgraft of around 4-5mm. My question would be is it possible to instead opt for a much larger downgraft (around 8-10mm) for aesthetic benefits? My midface is incredibly short and I’d assume a larger maxilla downgraft may help alleviate this issue. Id be willing to have a gummy smile if it meant lengthening the midface. If this isn’t possible, do you have any insight on future surgical methods to lengthen the midface? Thank you.
A:The accurate answer requires a full orthognathic surgery workup. But it would be fair to say that an 8 to 20mm vertical maxillary lengthening is unstable and would have other adverse effects on the positioning of the mandible.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I did an implant on my back of head in 2017.Can you please check for me, is it a silicon implant that I have?? Do I also have two screws in there?

 A:You are correct on both counts. You had a solid silicone skull implant placed back in 2017 which was secured with two titanium microscrews as seen both intaoperatively as well as on a postop 3D CT scan.
A:You are correct on both counts. You had a solid silicone skull implant placed back in 2017 which was secured with two titanium microscrews as seen both intaoperatively as well as on a postop 3D CT scan.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can you design a custom hydroxyapatite forehead implant? I need a bio scaffold type implant.
A: That can not be done in a satisfactory aesthetic manner (will have a lot of visible edging since HA can not be made with 0.2mm feather edges) nor can it be surgically placed unless a full coronal ear to ear scalp incision is made.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am from Poland and I am interested in rib removal surgery. I read about different methods and wanted to ask which one you recommend in my case. I am 29 years old and a woman, but I have always had a very boyish body type. In addition, I have mild scoliosis. I’ve had two breast implant surgeries, but they still separate slightly from side to side. The doctor said it was the chest.
It is also important for me to know what the scars look like before I decide to undergo surgery – can you send photos? and the price of the treatment.
Please let me know what you recommend in my case.
I also saw hip implants in your offer, which made me curious because I had never heard of it – would you recommend it in my case? Is it safe? What do the scars look like?
My hip circumference is only 80 cm
A: 1) I would need to see pictures of her body to do some imaging to have her see what type of waistline reduction change is possible.
2) I would go to www.exploreplasticsurgery.com and search under rib removal where extensive informatiomn about rib removal surgery can be found in over 100 writings on the topic, including the incisions used and scars.
3) But the attached two pictures are representative outocomes from the incisions used for Type 1 rib removal surgeries.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can I get custom jaw angle implants after failed jaw angle implants after V line surgery?
A: In my experience with V line surgery correction the ostectomy lines on each side are rarely symmetric and more commonly asymmetric. Given that what is really missing is vertical length from the amputation of the jaw angles it is best to use a custom implant approach to get a stable and symmetric result. While your initial effort at that resulted in a wound dehiscence and subsequent implant removal without custom implants the aesthetic result may have ended up unsatisfactory anyway.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
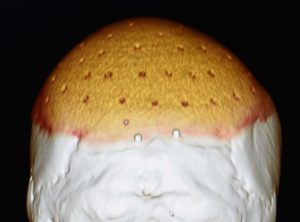
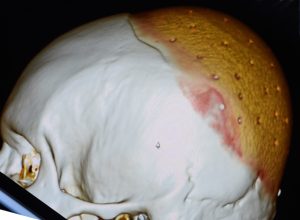
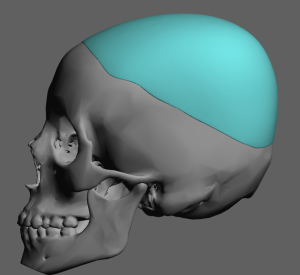
Q: Dr. Eppley, I am in need of a custom skull implant. How much time do I need for this process and recovering? Do you think 3 weeks are enough? Also, If I come to USA, how long it will take to prepare a skull implants for me..
I took some pictures. It is almost impossible to understand unless you touch it. I had fillers before. In my researches at that time, that doctor was the only onewho did skull filling in Turkey. He was terrible. He used kind of bone powder I guess.. I It was a dough and he inserted it under my head skin and the dough has hardened. But he couldn’t succeed. Failed to place the filling evenly on my head. In the pictures, everything looks normal but in reality it is not. There are a lot of depressions on my head and it hurts me when I sleep, brush and touch my head. I marked the that areas with red pen in the pictures.
Thank you so much for your attention!
 A: This appears to be a classic attempt at croewn of the skull augmentation using bone cement which, besides the limited result, often ends up very irregular and uneven in shape. The bone cement should be evident on thje 3D CT scan but teh images attached are of limited views so it is not seen.
A: This appears to be a classic attempt at croewn of the skull augmentation using bone cement which, besides the limited result, often ends up very irregular and uneven in shape. The bone cement should be evident on thje 3D CT scan but teh images attached are of limited views so it is not seen.
What you are now seeking is a better skull augmentation method using a custom skull implant. To answer your logistical questions:
1) Custom skull implants are made off of the 3D CT scan so I will need the actual disc of that scan. Such implants are made well in advance of the surgery as that process takes about 3 months to complete. You come here only for the surgery, appearing one day before the surgery. Your implant design would be very similar to that which is attached….likely just a bit smaller in size of the implant footprint.
2) Your stay here would be short, returning home no more than 4 to 5 days after the procedure.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am writing to inquire about the best approach for reversing a cheekbone reduction procedure given my situation. Could you please inform me about the costs associated with Cheekbone Reduction Reversal surgery?
Additionally, could you provide an overview of potential solutions in the event of an infection, whether it pertains to my custom jawline implant surgery or the cheekbone reduction reversal surgery, and give a rough estimate of the total cost for revision surgery in case of an infection?
A: Cheek bone reduction surgery could consist of an implant overlay or a reverse cheekbone osteotomy with interpositional graft. Eachj has their advantages and disadvantages and the aesthetic outcomes between the two are slightly different. This is a personal choice so I would have to know which you prefer.
In the infrequent occurrence case of an implant infection I remove it at no charge and as soon as possible. Most implant-based infections do not resolve otherwise.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
 Q: Dr. Eppley, Can I be like someone by getting facial reshaping implants (celebraty). Indeed, there is a similarity between us, but I want to be a copy of him. The celebrity is Zayn Malik.
Q: Dr. Eppley, Can I be like someone by getting facial reshaping implants (celebraty). Indeed, there is a similarity between us, but I want to be a copy of him. The celebrity is Zayn Malik.
A: No one of course can be made to look like someone else….unless they re very close initially and the feature differences are structural in nature.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had been perusing through your impressive website about cosmetic and reconstructive facial implants. Some of them seem rather large.
If you have time, would you be able to give me feedback on these topics that your plastic surgery website inspired?
1) For your larger complete mid-face “mask”, how do you secure each piece to minimize movement, migration and possible extrusion?
1.5) In the case of customized implants – for any part of the face – how is the height of each part of the implant measured to ensure that the lift or elevation afforded by the implant is optimal but also not too exaggerated. Is there a biometric baseline used? Every face is different; men and women, people of different ethnicity, people who are middle-aged or very advanced in age and some people are heavily affected by social media’s standards about what is trending or currently considered “hot” which means they have different facial surfaces and want different potential results. How does the customized implants production account for all these factors in determining the most ideal heights, surface relief, etc.?
2) With such a large silicone implants, how does the inner skin tissue (above implant) and the bone underneath deal with this interruption in the strata of delicate tissues that the implant(s) now wedge between and the wedging encompasses a significant surface area? Even if a capsule is formed from the natural immune system trying to isolate this large foreign object, doesn’t the significance interruption between health inner skin and muscle/bone interface over a large surface create other complications?
3) Do these large implants cause restrictions for future cosmetic facial procedures? Take the mid-face mask with or without cheekbones involvement in the implants. Would a future plastic surgery such as a deep plane face lift or rhinoplasty, for example, be made impossible to do or with severe compromised aesthetic results?
4) I read in several medical journals that the mid-face, especially the region where the cheeks meets the mid-nose and the piriform apertures – suffer the most wearing away of the bone with the natural aging process. It makes individuals in their 60s and 70s look very gaunt and deflated in the face. (But it’s natural, so I am not implying that Father Time is evil.) So if a man or woman gets anyone of your customized implants in these vulnerable areas, with time, wouldn’t the foundation on which the implants sit on be so fragile when the patient reaches age 70 or 80 that it might fracture the natural aged bone foundation underneath? The bone tissue thins out over time but the implant remains hard, unyielding and applying a downward force and tension/stress on the bone underneath.
Help educate me in the event I might invest in your artistic and technical precision at Eppley Plastic Surgery or just to help me because more information about these exciting elective procedures. If you do not have time, that’s okay. Any clarification or education will be warmly appreciated.
Thank you for your time.
A: In answer to your custom facial implant questions:
1) All facial implants are secured with titanium microscrews.
1.5) The design of any custom facial implant is an artistic endeavor more than some scientific measurements which don’t exist for it. Experience is another major factor knowing the effects of a implant design to its external aesthetic effecvts.
2) It does not. It merely sits there passively.
3) They do not.
4) That is not a risk. That theoretical biologic sequelae is not a reality.
Dr. Barry Eppley
World-Renowned Plastic Surgery
Q: Dr. Eppley, I received a custom brow/forehead implant as well a total midface implant four years ago. Ever since the surgery, my left temple has always felt a little different than my right. Closer to the time of surgery, I would occasionally get sharp twinges of discomfort around the left edge of the implant. I haven’t felt that discomfort in a long time, but that area will sometimes briefly itch for seemingly no reason. That area also feels a little more sensitive than the same spot on the right side, even years later. All of these sensations can be traced back to the time of surgery. The left side was also the side that experienced more significant bruising.
This is not a serious issue by any means, but I want to check in to know if there might be anything I should keep in mind going forward. I am extremely happy with my implants and want them to stay healthy for the rest of my life.
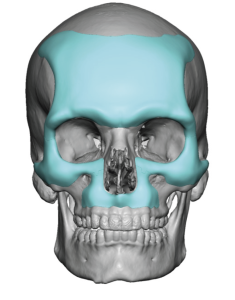
 A: Good to hear from you after our surgical adventure from 2020. Those left-sided symptoms suggest a more neurologic basis as abnormal sensations from one of the lateral branches of the sensory supraorbital nerve which could have been more stretched form the greater swelling/bruising on that side. That is what itching would indicate as opposed to a problem with the implant. Such small terminal branches of a sensory nerve are either trying to recover or just exhibit an abnormal sensation from time to time given the stretch injury. When we look at the rather ‘extreme’ nature of the augmentation (implant surface area) and the periorbital incisions needed to do it it is probably surprising that is the only relatively minor sequelae from the surgery. Whether that will ever change over time remains to be seen.
A: Good to hear from you after our surgical adventure from 2020. Those left-sided symptoms suggest a more neurologic basis as abnormal sensations from one of the lateral branches of the sensory supraorbital nerve which could have been more stretched form the greater swelling/bruising on that side. That is what itching would indicate as opposed to a problem with the implant. Such small terminal branches of a sensory nerve are either trying to recover or just exhibit an abnormal sensation from time to time given the stretch injury. When we look at the rather ‘extreme’ nature of the augmentation (implant surface area) and the periorbital incisions needed to do it it is probably surprising that is the only relatively minor sequelae from the surgery. Whether that will ever change over time remains to be seen.
Attached is an endoscopic picture from your surgery showing the left supraorbital nerve and vessels as they exit from the brow bone and the dissection needed to make the space for the brow bone implant. So it is easy to see how small nerve branches can get severely stretched.
Dr. Barry Eppley
World-Renowned Plastic Surgery
Q: Dr. Eppley, I have a question. I want to do shoulder width reduction. And that I want my shoulders to be lower and more droopy like these two examples. It is possible ?
A:In clavicle reduction osteotomies it pulls the shoulders inward and down a bit…which I believe is what you mean by ‘droopy’. How significant that effect is depends on the patient’s individual shoulder shape. I don’t know the specific examples to which you refer but they probably are representative of the general effect of the surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I got mandibular angle implants and now have masseter dehiscence. I have no outward projection, and the sunken angles have made my face look round from the front. My masseter is noticeably high up. This is the opposite of what I wanted. I find almost nothing when I research this, but nearly everything I do see is from Dr Eppley. As of now, is the surgery to reattach the masseter still likely to fail? I really do not want to use filler, so what would be my best course of action?
 A:This is classic masseteric muscle dehiscence in which you have correctly assumed that actual muscle repositioning usually is unsuccessful. The most effective approach I have found is a graft (Alloderm,- cadaveric dermis) or soft tissue implant augmentation method done through a small direct incision (1 cm) right behind the jaw angle area.
A:This is classic masseteric muscle dehiscence in which you have correctly assumed that actual muscle repositioning usually is unsuccessful. The most effective approach I have found is a graft (Alloderm,- cadaveric dermis) or soft tissue implant augmentation method done through a small direct incision (1 cm) right behind the jaw angle area.
Dr. Barry Eppley
World-Renowned Plastic Surgeon