Your Questions
Your Questions
Q: Dr. Eppley, I am interested in total jawline augmentation. I can show you the change that I am looking for when I jut my jaw down and forward as shown in the attached picture. Do you think this type of jawline change is possible?
A: In looking at your own prediction imaging by moving your jaw down and forward, it creates two artifacts that will not happen from a surgical procedure like a custom jawline implant for total jawline augmentation.
First, the depth of the labiomental fold will not be pushed forward or become more shallow. The depth of the labiomental fold can only be changed by bring the teeth forward (lower jaw advancement) not by any jawline implant augmentation. It sits above the level of the bony chin so any form of chin augmentation will not change it and may make it a bit deeper.
Second, the jaw angle area will be come more obvious or angular with implant augmentation. Jurtung the jaw forward actually blunts the jaw angles as they come down and forward. An implant will actually make the jaw angle more pronounced or stronger as your ideal pictures demonstrate.
I have attached an adjusted imaging picture which I think is more realistic of the actual result in profile view.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am considering chin implant revision. I got an Implantech medium anatomical chin implant through a submental approach six months ago.
Before I list my questions/concerns, I would like to say I’m extremely happy with the way the implant looks and prefer to keep it than to remove it but the tightness on the right side of my lower lip is very bothersome. I received a few doses of Botox to see if it would relieve the tightness and it has but I’m afraid this is only masking the feeling and not really taking care of the problem. I would love to think it would solve the problem with the tightness but I know Botox is only a temporary fix. And I wouldn’t want to wait too much longer as I feel my nerve might be compressed and have some hope perhaps I could get some feeling back and relief of the tightness if I were to remove it. The reason I think I’m hopeful on my nerve having some feeling back is because when I stretch my mouth downward (as if I were yawning), I feel immediate relief. Also, when I push the right side of my lip outward with my tongue, I feel lots of tingling on my right lower lip as if there was still some nerve messaging going on there.
This is why I needed a second opinion on what I should do. I’ve heard of numbness sometimes being permanent but is this true with tightness as well? If I were to remove the chin implant, will the recovery be as when I put the implant in? Can tightness still be a problem even after removal? Does scar tissue cause problems after removal?
Thank you for your time and consideration as this has been an emotional rollercoaster for me. I don’t think I can go through a revision either as I have heard that those who have had it done usually opt to remove it anyhow due to other issues. I appreciate any guidance.
A: Thank you for supplying your additional information. The most important thing to know with your symptoms and considering a chin implant revision is what is the actual position of the implant on the bone. Is the implant placed symmetrically? Is an implant wing up against the mental nerve? Are your symptoms due to the implant position or just from the soft tissue alone? Your symptom description implies the former.
Tightness issues can be different than nerve issues but it is important to know where the implant is actually sitting on the bone which can only be obtained from a 3D CT scan. If you didn’t like the aesthetics of the chin implant then such a study would be irrelevant. But since you do, first establishing that the implant is in a good and symmetric position and its wight wing is not compressing up against the mental nerve would be a critical piece of information in how to proceed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a middle-aged male and I recently noticed that I have bulging temporal arteries (can feel a pulse) on both temples, which look like squiggly worms from my ear arcing up to my (receding) hairline. These arteries are visible at rest but really ‘pop’ when I get hot, drink alcohol, or workout. I did not have these (or at least they were not noticeable enough) several months ago. I went to a Rheumatologist, who ruled out GCA/temporal arteritis. I am now exploring options to reduce the visibility of these, one of which is arterial ligation and I have a few questions:
1) In lieu of GCA/temporal arteritis, what causes the temporal artery to suddenly swell and become permanently visible (I’ve read about others who have experienced the same thing)?
2. How many of these temporal artery ligations have you performed? How many needed follow-up procedures?
3. My biggest fear by far with this procedure is damaging the facial nerve, which from pictures I’ve seen, runs extremely close to the temporal artery. I know plastic surgeons study where the nerves are but I assume the location of the facial nerve differs in everyone. Any damage to this nerve would becatastrophic and would be 100x worse than the bulging temporal arteries. How would you respond to this?
4. How do you ‘map’ these arteries to determine if there are ‘feeder branches’ that would circumvent the ligation – do you use some type of ultrasound?
5. Could ligating the temporal arteries cause the arteries that run from the eye to the hairline (or other facial arteries) to swell and turn into the ‘squiggly worms’ (I read about a guy who this happened to 3 years after he got a temporal artery ligation).
6. Which arteries would supply the scalp / forehead if the temporal arteries no longer function?
7. Does the temporal artery supply blood to anything else (besides the scalp / forehead)
8. How big are the incisions? \I’ve read that dissolving stitches leave a bigger scar than removable stitches – is this true?
9. Do you tie off the arteries or sever them? I read that you don’t drain them – how does that remove the bulging effect as the blood would be trapped within the temporal arteries (I picture a water balloon – you can tie off the end but all that does is trap the water in, making the balloon swell).
10. I assume it is local anesthesia, correct?
11. What is the recovery time? What is expected post-op as far as swelling / bruising / scarring / time until return to work / exercise / etc?
12. Do you perform this procedure on Saturdays for out-of-towners?
A: In answer to your temporal artery ligation questions:
- It is unknown.
- I have performed over 50 temporal artery ligation v]cases which has resulted in about 10% to 15% needing a touchup for additional ligations.
- The frontal branch of the facial nerve is not in the same areas as the ligation points
- Visual and digital assessment is the method used to map out the arterial patterns.
- This is not something I have seen. With multipoint ligation this risk is lowered significantly.
- There are many other arteries that supply the scalp.
- No.
- 5 to 6mms for the incisions size. Dissolveable sutures do not leave a bigger scar.
- The arteries are double tied but not cut. The blood is stripped between the ligation points to prevent postoperative bulging.
- Local anesthesia is correct.
- There is very minimal recovery time, no real recovery actually
- I only operate during the weekdays.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,I’d like your opionion on having a chin prejowl implant, or just a pre jowl sulcus implant. My concern is not the anterior projection of my chin, but the verical height. I think an implant that can add around 3 mm of vertical height below my chin, and widen or treat the prejowl area (maybe make it more square, as well) would be my best option. My goal with the implant is to disquise my double chin line underneath my chin (already treated with liposuction and Ulthera), and maybe to improve jowling if I have it. Of the off the shelf implants, what would be my best choice? Thank you very much!!
A: Thank you for your inquiry. If the vertical height is the main objective with your chin augmentation, with the addition of some squareness, no standard chin implant has those dimensions to make those changes. Certainly a chin prejowl implant can not accomplish those changes. That would require a custom chin implant design. In addition your neck should ideally be treated with a submentoplasty as your main problem now is the fat that lies below the muscle, that combined with some muscle tightening will take the results of the prior neck liposuction to another level of improvement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in plagiocephaly surgery. I was wondering what procedure would be better to reshape the plagiocephaly of my head. I have seen that there is a procedure done in South Korea where they use bone cement to remodel the shape of the head. I was wondering what opinion you had about that procedure or the use of an implant. what are the pros and cons? I really appreciate it and thanks in advance Dr. Eppley.
A: A custom skull implant is almost always better than bone cement for almost any form of skull augmentation for the following reasons:
1) it can be put int through a smaller scalp incision,
2) it can cover a broader surface area in a smoother fashion,
3) the shape of the augmentation and all of its details is determined before surgery and is not left up to the ‘artistry’ and hands of the surgeon,
4) it has a much lower rate of revision due to inadequate augmentation, irregularities or visible implant edge transitions that are far more common with bone cements, and
5) it is very easily reversible if needed. A silicone skull implant be fairly easily removed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in Chinese rhinoplasty surgery. I would like to schedule a consultation regarding the removal of a dorsal hump on my nose. I am Chinese and feel as though the bump does not look normal. I have attached side profile pictures for your assessment and recommendations.
A: Thank you for sending your pictures. In the Asian nose a dorsal hump often occurs because the radix (the height of the nose between the eyes) is low. Thus a pure hump reduction may make the nose look flatter and wider particularly in the frontal view. Conversely augmentation of the radix with less of a hump reduction keeps the nasal bridge higher and may create a better look. I have attached some imaging which shows the difference between these two different approaches to managing the nasal hump in the Asian or Chinese rhinoplasty patient. Consideration must be given to how the nose will look in the front view as well when taking down a nasal hump
Most Asian rhinoplasty surgeries are more about augmentation than they are about reduction of nasal heights. Bringing out the midface in general is often an overall facial goal.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in lip reduction surgery. However at rest my lips are parted and my mouth is open slightly. I’ve read this is normal but also have read that it may be minor lip incompetence. Would a lip reduction be contraindicated in this situation until I have the incompetence addressed? I’m worried about having my mouth look even more wide open and apart with a thinner upper lip and having to strain more to keep my lips together and mouth closed. I am planning to have a sliding genioplasty at some point. Is it best to wait on the lip reduction surgery until after the sliding genioplasty?
A: The answer to your lip questions is very straightforward:
1) Lip reduction, particularly upper and lower lip reduction, will exacerbate a lip incompetence issue.
2) A sliding genioplasty should absolutely precede any consideration of lip surgery.
That being said your description of your ‘lip incompetence’ seems questionable that it may really exist to any significant degree. Usually significant lip incompetence is associated with some degree of mentalis strain with underlying lack of adequate chin projection. But it would still be advised to have the chin procedure first before any lip surgery is done.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I do have a few questions concerning the lower third of my face which I hope you can answer.I am interested in perhaps vertically lengthening my chin since I think my chin and lower facial height is vertically deficient. If I understand correctly a sliding genioplasty is the best option for achieving vertical chin length. I am also hoping that the genioplasty can contour my chin to create a smoother transition from the chin to the jaw. My main concern regarding the sliding genioplasty is that I don’t want to add too much length since my jaw is quite narrow. I already have a narrow face and I think if I were to add a substantial amount of vertical length to my chin this would only serve to accentuate my narrow face. I would end up with a long, narrow face, which often does not look appealing.
My questions are:
1. Do you agree that my lower third + chin are indeed vertically deficient?
2. Do you think I could benefit from vertical chin lengthening?
3. Looking at my face, what facial type do I have (narrow, long and narrow, oval etc…)?
4. Looking at my pictures + x rays, do you think that my lower jaw width is indeed too narrow for my face?
4a. Follow up question… what is the ideal width of the mandible relative to the face (wider than the eyes, cheekbones, face)?
5. Will the sliding genioplasty create a longer, more narrow face?
6. Could you provide a bit of information about jaw implants and ramal augmentation (what material is used, infection risk, bone resorption, effects on soft tissue, long term risks/complications)?
Finally, a few things regarding my dental health. I have been told that I have a very thin biotype, in fact my periodontist told me I have some of the thinnest bone and gums he has ever seen. I have very little bone surrounding my lower incisors and from what I understand about the sliding genioplasty procedure, the incision is made very close to the lower incisors. I have also read about a case where the patient had significant gum recession following the sliding genioplasty procedure due to wound contraction. Is my thin biotype an issue when deciding whether I am a good candidate for the sliding genioplasty procedure?
Thank you,
A: In answer to your questions:
1) A sliding genioplasty is one method of vertical chin lengthening but not the only one. A custom made vertical lengthening chin implant can also be done and is the most assured method of a smooth transition from the chin to the jawline going back.
2) I do not have an opinion about your facial width or length. This is a matter of personal aesthetic judgment for which only you can truly answer that question. Ultimately that question is best answer by computer imaging so you can determine whether such lower facial changes are aesthetically advantageous.
3) Since I have not seen your intraoral anatomy or an x-ray of your jaw I can not comment on the state of your dental health and whether it would be adversely affected by an intraoral bony genioplasty. But the development of gingival recession from a sliding genioplasty is likely a reflection of surgical technique and is not a standard result from the procedure. It is not a postoperative finding I have ever seen.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I wanted to inquire about how you perform an upper lip reduction as I am looking to get this procedure done for my naturally full lip. There seems to be a lot of variability in the shape of excision that surgeons use – some do an ‘infinity loop’ or ‘bikini top’ shape (two ovals joined by a central band), others do a trapezoid shape, and still others simply say they remove an undefined “wedge of tissue”. I assume the shape of excision impacts the final outcome, so am confused as to why there is such variability, and what approach you take and why.
A: The shape of the excision pattern in lip reduction does not really affect the outcome significantly. Lip tissue is very stretchy, unlike skin, so any pattern of excision will end up in a straight line that largely parallels the vermilion-cutaneous border. The most common excision pattern in lip reduction surgery is a crescentic pattern that is wide in the midline and tapers to the sides.
One should not become overly focused on the excision pattern. What is more important for the outcome is where on the lip it is located. The key to a visible lip reduction result is the removal of exposed dry vermilion rather than the wet flexible mucous of the lip.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a few questions about an image on your website from an orbital asymmetry correction procedure which you performed years ago.
The image can still be found on your website, and is viewable from the link below:
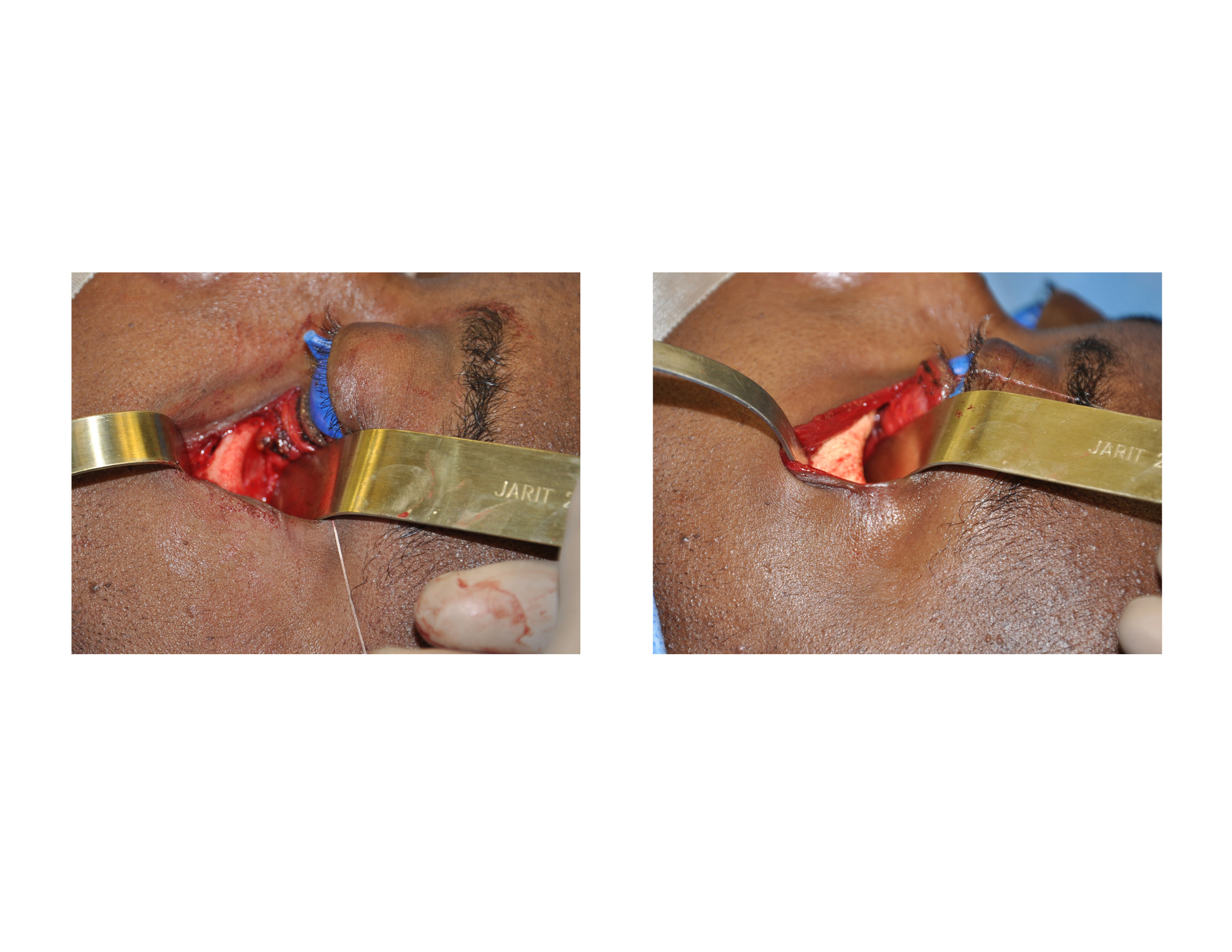{kind=link}
My questions are about the blue medical “gauze” which was placed between the patient’s eyelids and globes to protect his vision during surgery.
1. What is the technical name of this blue medical protective gauze? Or is it an invention of yours?
2. What is it made of, in terms of materials?
3. How much irritation is caused by its contact with the cornea?
I am concerned because, as someone who wears contact lenses, I have experienced how easily irritated or even scratched the surface of the cornea can become simply by contact with an insufficiently lubricated contact lens, whose composition is already over 50% water and is specifically designed for contact with the cornea.
I’m sure some level of discomfort/irritation is expected, being that it is part of a surgical procedure, but in your experience do patients experience any severe levels of irritation or scratching of the cornea after contact with such a gauze? Is it lubricated or treated with an antibiotic in some way to prevent adverse effects?
Thank you for reading my questions. I suppose I am overly protective of my eyes..only have two of them after all.
A: The blue eye gauze to which you refer is not gauze at all. Those are devices known as. corneal protectors which are rigid plastic covers designed for the eye for protection during any form of periorbital surgery. Lubricating ointment is first placed in the eye and then the corneal protectors are placed which have already been lined with lubricating ointment. These corneal protectors are used injections all surgery around the eye for the express purpose of eye protection.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a custom skull implant replacement. I am a patient of yours from 2014. You performed a successful skull implant surgery on me and I am extremely grateful. There certainly has been some improvement in my life – it usually takes a bit less time for me to get ready, etc. However, as I know that you offer 2 stages of the custom implant – one which entails using a spacer to enlarge the implant area, and I opted for the one-time only option, I was wondering if there is any ability to have a second surgery? I guess I am wondering if the first implant itself might have acted as a spacer of sorts, creating more room for a larger implant now? I truly don’t mean to sound vain or ungrateful, as the first implant surgery has absolutely helped! But I am still struggling more than I would like… I understand if this is not an option or simply a procedure you do not perform, but I thought it was worth asking before I gave up. I am not a body dysmorphic person or someone who will continue to seek the “next thing.” It’s really just that I am still relatively young, and with the efforts I am still having to make with my hair, to get ready, go swimming, etc, it makes me sad to think of spending the rest of my life this way. I was hoping to achieve (if possible) another few mm at the top and upper sides of my head. Thank you for your time, Dr. Eppley. I know you are very busy and I hope this email doesn’t find you rolling your eyes at someone who is ungrateful. Please know that is not the case.
A: Good to hear from you again. Your supposition that an indwelling scalp implant can act as a spacer or tissue expander is completely correct. A second skull implant (custom skull implant replacement) can be placed that is usually double the thickness of the first one (9 to 18mms in your case) as the scalp has had time to stretch and relax to accommodate its volume. Placing the second jmplant is usually a bit easier on the patient since much of the pocket (separating the scalp from the bone) has been done from the first surgery. As you may guessed, this is not the first time I have had this request so there is no eye rolling occurring. In reality this is just a different form of a two-stage skull augmentation approach…it just occurs over a longer period of time. And the good news is that I have not yet had anyone want to go on to a third skull implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: D. Eppley, I have some technical questions about custom jawline implants. The implant looks like solid silicone. Do you divide it in the midline for insertion? Do you use any screw fixation or just close the periosteum over these implants? Is your incision strictly transcutaneous or do you incorporate buccal incisions as well?
A: In answer to your questions:
1) All custom jawline implants require a three incision placement technique. (2 posterior vestibular and 1 anterior, submental or intraoral) It is a biggest facial implant that can be placed and requires multiple incisions to be inserted.
2) If the implant has large jaw angles, it needs to be divided in the midline and inserted in a posteroanterior approach to eliminate the risk of mental nerve injury. The key to a single for split custom jawline implant is the size of the jaw angles and how easily they can be folded during insertion.
3) If the implant has smaller jaw angles that can be easily folded it can be inserted as a single piece in an anteroposterior method.
4) The implants are placed in a completely subperiosteal pocket.
5) A three point microscrew (1.5mms) fixation is used at the chin and jaw angles.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in getting a second custom jawline implant. I should have listened to you with my first implant when I asked you to reduce in surgery the size of the implant. I regret that decision now two months after surgery as what I have now is too small. I would like to potentially proceed with the procedure, but I have some questions first
1. What are some potential risks of doing a revision?
2. Is the risk of infection higher?
3. Is the risk of the surgical wounds not healing higher?
4. Are there any extra risks with nerve damage?
5. Do you remove the screws from the previous implant or do you leave them in there?
6. How much would it cost to remove the revision implant, clean and reinsert if I was to get an infection? And when this does happen, what are usually the percent chances that an infection happens again?
7. What is the recovery like for the revision compared to the initial procedure?
8. Are there any permanent risks associated with doing a jaw implant or a jaw implant revision?
9. Would you consider a jaw implant revision easier or harder than on the surgeon compared to the initial procedure? And why?
10. Do you normally reopen the same wounds or create different wounds inside the mouth?
11. How long do you recommend waiting to let the initial wounds heal before doing a revision?
A: In answer to your custom jawline implant revision questions:
1) The surgical risks as identical to the first custom implant procedure as it is the same operation.
2) The risk of infection is the same as the first time.
3) The risk of intraoral wound dehiscence is the same as the first time.
4) No
5) The screws are removed as they have to be to remove the implant.
6) The risk of facial implant infection is around 2% to 3% every time one is inserted.
7) The recovery will be identical to the first time.
8) A custom jawline implant revision surgery incurs the identical risks as the first time, they are no higher or lower.
9) It is the same surgery so it is equally ‘hard or easy’ as the first time. This is not a surgery I would ever consider easy no matter how many times it is done.
10) The same incisions are used the second time as the first time.
11) I advise 3 to 4 months before proceeding with any secondary implant surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in lip reduction surgery. In your experience, what is the revision rate for lip reductions done on natural (no foreign material) lips? One office I called gave an estimate of “1 in 4 (25%)”, which I think is shockingly high! What has your experience been, and what is the most common reason a revision is requested by patients?
Also does the lip’s overall shape change much with the surgery? I would like mine to be more M-shaped and curvy, as it’s currently lacking any definition. Or does that require a different procedure entirely?
Thanks.
A: The revisions rate for lip reduction at 25% to 33%, which I consider to be a very realistic and honest number, may seem shockingly high to you but that is the reality of doing aesthetic procedures on the lips. The most common reason for as revision is the desire for more reduction that can be achieved in a single procedure or some minor issues with the scar. In male lip reduction patients, which make up the majority of lip reduction procedures, I would put that revisions rate of 50% or higher. Young male face patients, of which my practice has an enormous experience, are the most challenging and particular of all aesthetic surgery patients.
A lip reduction is a debulking/volume changing procedure not a lip reshaping one. It can not or should one expect any shape change in their lips.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had jaw surgery and genioplasty almost a year ago to correct my recessed upper and lower jaw, which was fairly successful. However I still have a few remaining issues. One being that I have pretty significant notching along my jaw line where the cuts were made (14mm advancement). I also need to add length and width to my ramus. I figure I would have to go the custom route due to the asymmetry I have and large notching from my sagittal split jaw osteotomy.
A: Deformities of the mandibular ramus are not uncommon after sagittal splits osteotomies particularly large advancements. By your description a custom jaw angle implant would have the best success rate insect cases of jaw asymmetry. The first place to start is to send me some pictures of your face for my assessment and I will have my assistant contact you to schedule a virtual consultation time. Ultimately a 3D CT scan will be needed to not only show the anatomy but it designing the custom jaw angle implants for insertion. The 3D Ct scan can be done where you live and I can place the order for it.
Dr. Barry Eppley
Indianapolis Indiana
Q: Dr. Eppley, , I am interested in doing a scrotal lift procedure. I am 32 years old and I have family genetics with large scrotums unfortunately. I want to know the risks for having this procedure.
A: The scrotal lift is am aesthetic genital procedure that tightens and lifts the scrotal sac through a midline excision of tissue along the raphe. Such a reduction lifts the lower edge of the scrotum by a wide removal of scrotal skin and deeper tissues that raises the level of the bottom hang of the scrotum. It leaves a fine line scar that often looks just like the raphe itself. The scar is really the only ‘risk’ of a scrotal lift other than standard ones like infection or hematoma which are very rare in this type of surgery. Because the tissue excision is in the midline it has no impact on the function or position of the testicles which are to the side of the midline
.The aesthetic ‘risk’ is the outcome of the procedure which is obviously important. There is always the question of whether the degree of improvement (reduction and lift) meets the aesthetic expectation of the patient. In my experience it is a highly satisfying procedure and the revision rate is very low.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Thank you for all the info you generously gave me on midface implants. I came across this image on your website. I wonder if it’s a combination of premaxillary implant and cheek implant. In addition, I feel a bit nervous about having this surgery. It seems like you are the only doctor who talks about it. When I look up premaxillary implant, there is a poor amount of info found on Google and all that info are written by you. I found absolutely nothing else other than the posts you wrote, not the info nor any before-and-after photos. I tried to search in a different language too but nothing. Other doctors seem to work on only cheek implants. Did you ‘invent’ this surgery? Or does this surgery go by another name? Or is it just that this surgery isn’t popular?
I honestly feel weird about this and feel more anxious when no info can be found on the internet. On one hand I really want to improve my appearance, on the other hand, I can’t just have a surgery if i don’t feel well-informed. Is there anything about this you can tell me?
A: The custom implant image to which you refer is a total midface implant that covers the paranasal, premaxillary, anterior cheek and infraorbital rim areas. Implant augmentation of the base of the nose (premaxillary-paranasal region) has been around for decades. It is not ‘popular’ because it is not commonly requested and almost all surgeons have no experience with it. In my experience midface implants have moved beyond trying to use various implant materials not specifically designed for it to try and make it work. The use of custom implants designed and fabricated from the patient’s 3D CT scan allows for midface augmentation results around the nose that have previously been unattainable in any other reliable way.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, regarding jaw angle reduction or removal (traditional jaw angle amputation) where the surgeon cuts off the jaw angle at the mandibular ramus. Will the masseter muscle also be cut? (looks like the masseter muscle covers this area of the bone) If the masseter muscle gets cut, then what will happen and what will be the potential consequence?
A: In jaw angle reduction surgery the masseter muscle is first lifted off the bone through subperiosteal dissection. Then the bone is cut and the muscle falls back into place during closure. Thus no muscle is cut unlike that of the bone.
While no muscle is cut during jaw angle reduction surgery, the muscle will retract upwards to the new lower border of the jaw angle when it is amputated or removed in an oblique full thickness bone cut fashion. This does not affect its function or mouth opening/closing. But between the bone removal and muscle retraction the shape and support of the soft tissues will change over the angle area. Facial width will definitely be less and hopefully there will be no soft tissue sag as a result.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I wrote to you before about my chin implant removal problem but I wanted to wait a little bit more to have a surgery. I am 22 years old and had a bad chin implant surgery six months ago. The chin implant was the extended anatomical type, Implantech brand, small size 5.5mm. The incision was submental and implant stayed in only 2 days and was removed due to not liking it at all. It was a big mistake for my face. Its been is months and even though it improved with time, its not exactly how it was before both the shape and size of my chin. My chin is wider, longer, and bigger than before and it feels squashy inside and not tight as before. But now I see that,my jaw is also larger. My jaw was never touched in the surgery but somehow it effected it too. My jaw is obviously larger than before and its square. My jaw used to be V shaped and my face is now more square. My lower face looks heavier and not lifted. What can be the reason for my jaw to be larger? Is there a solution for that? Since you are one of the most qualified chin surgeons in the world, i thought maybe you know why and maybe you have seen something like that before. I am sending my pictures. Thank you so much.
A: I do remember your chin implant removal case and patients have come forth before with similar findings. While not common it results from the tissues being lifted off the bone for implant placement and they never reattach like they were before the implant. It should not have affected your jawline per se since those tissues were not lifted off of the bone as the wings of the implant does not go back that far. But that is the effect of the tissues along the chin and backward having an inferior descent creating the change the shape your jawline from the front.
Options for improvement are either a submental chin tuck, a jowl tuck up or a combination of both.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 30 year old male and have been debating about a skull reshaping procedure for the past five years. Attached are some profile pictures of my head shape and two pictures of my expectations. I was hoping to round out the back of my skull and shape it in a way that makes my jaw line more prominent/visually appealing. I’m sitting here wondering about the following factors:
1) Are my expectations reasonable/attainable?
2) Am I even a good candidate for this?
3) Is the scarring blatantly noticeable?
4) Will altering the back to improve the profile affect the frontal view (eg…head on)?
A: Thank you for your inquiry and sending your pictures. In answer to your skull reshaping questions:
1) The morphed images of the back of your head are fairly realistic, being able to achieve 80% to 90% of that change as a one stage skull augmentation procedure.
2) One is a good candidate for this surgery if their expectations are in line with what can realistically be achieved.
3) The implant is placed through a small horizontal incision low in the occipital region. This is a scar that is barely detectable without hair and undetectable with hair.
4) Changing the back of the head will have no effect on the front of the head/face.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I thank you for your pre surgery notes in relation to the psychological effects of living with a new jawline implant have become apparent this weekend. I think the initial panic set in and I’ve had to take a step back and think about your comments again. I think the initial feeling is that the implant is way to big – but again I’ve taken onboard your comments around swelling and the amount of time that should be allocated to allow this to subside. Aside from this I’d like to ask a few questions:
1) Can you advise how long I should wait to shave the area under the chin – where the stitches are placed (these dissolve naturally right?)
2) Will I have a noticeable scar from the skin were the stitches are?
3) If after a number of weeks the implant still looks out of proportion and I decide to have it removed what are the implications? Would the current implant cause a permanent change to my facial features?
4) How quickly could we move from making the decision to remove the implant to actually removing it ? (i’m not suggesting this at this point, I’d just like to understand the process)
A: in answer to your custom jawline implant recovery questions:
1) It is important to realize that you are just less than 4 days after your surgery…when things look their worse. A lot will change in the next 2 to 3 weeks when you will feel much more comfortable with the way your face will look.
2) Having done hundreds of custom jawline implants there is no way this design would ever be considered too big. Conversely, in a month or so you will likely feel the other way….thinking maybe I should have gone a bit bigger.
3) You may shave under the chin at 7 to 10 days after surgery.
4) Implant removal will likely have no adverse effects on your preoperative facial shape, particularly when it is this small size.
5) Any removal of the implant before 8 weeks after surgery, when you have had time to fully see the actual facial changes and adjust to them, would be capricious.
6) Implant removal could happen within a week if one decides to do so.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in facial implant revision surgery and fat grafting.Three months ago I underwent surgery with the following facial concerns/objectives, a weak chin (needed more projection and wanted in squarer in appearance), a weak jawline (wanted very strong, defined jaw line), hollow eye area and wanted slightly wider mid face. For those concerns I had a Terino Square – Style I chin implant, buccal fat reduction and fat grafting to under eye area and temples.
Although I can see an improvement in the projection of my chin in side profile I would have liked the chin to be wider. The chin implant alone has not provided me with the jaw line enhancement I wanted – disappointed with the results. The fat grafting carried out in the eye and temple region was very conservative and provided minimum results/very subtle improvements and my understanding is that the areas treated could further diminish as the fat reabsorbs. However I am happy with the buccal fat reduction.
After evaluating the outcome of my procedures and completing extensive research (including your website and case studies) I feel I have a much better understanding of what I want to achieve and treatment options available. I I would like my chin to be slightly wider in front view and feel that the going up a size (Terino Square Chin – Style I – large) could achieve this effect. I would like a much stronger and more defined jaw line. I feel my jaw angle is very high and that I have a vertical deficiency. I am very interested in the Vertical Mandibular Angle implant. I am open to custom implants if it will provide me with a better outcome – I am seeking a straight line back from the chin to the jaw angle point and after reading some of your articles understand that the potential dipping between implants needs to be considered. I would like to add more volume and increase width slightly through implants or fat injections. For the temples, I feel my head is narrow and would like it to be fuller and wider (smooth surface with gentle curves). I think further fat injections could help.
A: Thank you detailing your recent lower facial surgery history as well as your objectives. In reading through them I can make the following comments:
1) A Style 1 square chin implant lacks adequate width (45mm) for most men that seek a more square chin look. It almost has to be out to 50 to 55mms to have a more square effect.
2) A chin implant by itself is never going to create a jawline effect as the chin is but one-third of the total jawline.
3) Fat grafting in younger men of average or thin body frames rarely has much persistence and, at best, produces subtle/minimal results.
4) The only way to have a straight line from the chin back to the jaw angles is with a custom jawline implant.
5) I would have little confidence in fat grafting to the temples. It is a broad area and requires a lot of fat just to have just a little result and would not likely ever end up ‘fuller and wider’. Temporal implants are far more effective and have an assured volume augmentation result.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m not sure if I’m a candidate for a custom jawline implant. If I have symmetrical jawbone structure I don’t see why I should need it. In addition, I don’t have the capital for custom one. From my point of view, I have a very weak lower jaw, my chin is very behind plus it is narrow, as you can see from my smiling picture it looks like I have no connection between my ramus and my mental protuberance. In addition, my jaw is narrow as well plus it is not prominent at all since the whole jaw is short. What I’m looking for is both horizontal and vertical improvement in my jaw with non-custom jaw implants that will bring balance to my lower face. I’m not worried about my chin at this moment because I don’t have the resources.
A: Based on your initial stated objectives of improvement, you are speaking to a total jawline approach. You can’t bring the chin forward, length the jaw angles and make the jawline wider all at the same time unless it is a total wrap around jawline implant.
The most common reason for a custom jawline implant is not asymmetry, it is primarily used when the patient’s dimensional jawline needs exceed what standard implants can achieve.
Standard vertical jaw angle implants are an option if you just want to limit the change to the back part of the jaw only. (jaw angles) But with a revision rate of over 25% using standard jaw angle implants, it would be important to only consider this surgery if your resources are sufficient should the need for revisions surgery arise.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question, and it involves customized facial implants for the cheeks and chin/jaw. In college I played for the football team and and broke my face. My nose was shattered with an effort made to fix it several times. My cheeks and jaw were damaged and there is a lack of harmony between these facial features (cheeks, jawline, chin) that they once had. That may have gotten worse due to the fact that I was still growing. But I was wondering if these customized implants in both areas could “put me back together” and really give me more confidence. I know you place your cheek implants higher so as not to create a rounded face and to achieve angularity and do CT scans to create a perfectly conforming chin/jaw implant with the degree of jaw “flare” or width and verticality desired. I know very few people choose to have their photo put on the website, but with these tools is it basically possible to create the best/patient desired jaw angle/width and cheek implant/placement? Even “male model quality”? Because I know fillers are always another option but they are not permanent.
My last two questions are these:
1.Would a chin implant eliminate my chin dimple? I would not want that. If it was softened a little, that would be fine, but I wasn’t sure exactly where the implant was placed and how it would effect the soft tissue.
2. What is the infection rate on jaw implants? I know it is higher than chin implants, but thought maybe the CT used to make customized facial implants “custom build” would help reduce the instance of infection and subsequent removal. Thank-you for your time.
A: Thank you for your inquiry and detailing your facial concerns. First and foremost I would need to see pictures of your face for my assessment and computer imaging to see what may be possible. Second, while custom facial implants can be designed to any shape and dimensions, how to make those dimensions create any specific look is more an art than a science and is not a completely predictable process. Third, a chin implant will not efface or eliminate a chin dimple. Lastly, of all facial implants, any implant that involves the jaw angles has a high infection rate. While the overall rate of facial implant injections is around 1% to 2%, that increases to 3% to 4% in the jaw angle region.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had rhinoplasty done five years ago and developed a recurring abscess on top of my nose several years later. It was needled and cultures which turned out negative. I noticed a suture coming out but swelling with pus still builds up every week . I have been on Augmentin a few times but with no relief. What should I do? Is surgery needed?
A: Your descriptive history suggests that there is a foreign body in the nose that needs to be removed. Whether this is from a permanent suture or from an implant I can not say since I do not know what was specifically done during your procedure. If there was an implant placed in the dorsum of the nose then there would be no question about the source of the infection
But with recurrent swelling years after the original procedure and failure to resolve completely with antibiotics suggests that open exploration is needed to determine the source. Infection after rhinoplasty surgery are fairly rare particularly when autologous cartilage grafts are used. But sutures used inside the nose in rhinoplasty can be a known source of tissue irritation particularly if there are of the non-resorbable composition.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had spoken to you a few weeks ago about the tightness I had from my chin implant. You had recommended a 3D CT scan to make sure the implant was in the correct position. Before I could make the appointment, I started to carefully feel the implant and noticed that the right wing of the implant is heading up in the direction of the right corner of my mouth! This area is where I am feeling the numbness and tightness. I had put botox to relax the muscles but now that I have felt the position, do you recommend to remove the implant to help with the symptoms I have been having? I’m of afraid of another surgery to reposition it and having to deal with the long recovery again. I’m thinking the removal won’t be as bad as the implantation. Do you think the tilt in the implant is causing my symptoms?
Please respond when you can. I appreciate any help I can get and you seem to be the only one with the answers.
A: A malpositioned chin implant can certainly be the cause of various postoperative symptoms, which include tissue tightness. The way to answer the question of whether the implant is the source is to have it removed. On the other hand there is a reason you had the chin implant in the first place and it would be shame to abandon its original objective. (the argument for chin implant repositioning)
The best way to answer the question of chin implant malposition is with a 3D CT scan.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I started taking Accutane exactly one month ago – the dose is quite low, at 20mg once daily. I now have a problem / query. I realized I should have had surgery before starting on Accutane. I had an infected jaw implant removed earlier this yea and have terrible asymmetry as the jaw implant on the other side is still in place. I cannot wait 12 months to have this corrected (I say 12 months as the plan was to be on Accutane for 6 months followed by 6 months being Accutane-free)
My question is – how soon can I have surgery (custom wraparound jawline implant at least) seeing that I’ve been on 20mg Accutane daily for the last 30 days?
A: It has long been believed that wound healing may be compromised in patients taking systemic isotretinoin. The cellular basis of this potential adverse effect is that his drug affects the synthesis of collagen which is essential for normal wound healing. Despite this contention, animal studies have failed to show adverse effects in wound healing at doses of 4 mg/kg per day. Case reports and cohort studies looking at facial skin laser resurfacing, facial chemical peels, laser hair removal, rhinoplasty, tooth extraction and ENT procedures have failed to show any demonstrable or consistent increase in wound healing problems.
Does this mean that the purported adverse effects on wound healing by isotretinoin are a myth? It is fair to say that most of the clinical studies reported have very low numbers of patients which makes it difficult to really know if those findings are valid. Equally relevant, none of these clinical studies have involved the use of implants which have natural higher risks of complications and is always the ultimate test of wound healing.
Given that most of aesthetic facial surgery procedures are elective and there remains some doubt that isotretinoin has no adverse effects on wound healing, one should not have surgery while actively on the drug. If you stop the medication now, having been on it for just two weeks, the risks a wound healing problem from having facial implant surgery a month or two from now should be very low.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a sliding genioplasty several months ago and have muscle strain in my chin and my lower lip no longer functions the way it use to. My lower lip will not meet my upper lip without force and ends up tucking up under my upper lip when I chew, almost disappearing. My chin bunches up when I close my mouth and now I’m stuck with this open mouth expression all the time. My lower lip has also thinned and falls well below my lower teeth as if it’s being pulled down. My surgeon told me he projected my chin out by 4mm but not sure on the hight. I’ve read message boards of patients with the exact issues as me and say time has not corrected this. Is there anything that can be done to correct this Dr. Eppley? I asked my Surgeon to reverse or adjust my procedure but he will not. I am very distraught and not sure what to do.
A: To have such a cascade of perioral symptoms from a small 4mm horizontal advancement sliding genioplasty is very uncommon in my experience and is more likely with much larger bony chin movements. But that issue aside the question is why you have such symptoms…it is because of the bone movement or does it have to more with the soft tissue closure/adaptation to the new chin position? To give an informed answer it would be helpful to see before and after pictures of your face and any after surgery x-rays if your surgeon obtained them.
But in refractory cases like yours where the symptoms did not improve with time, a reversal procedure would be the most logical approach to improving your current symptoms.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question for nipple lift surgery. I am considering redoing my breasts implants. If I did, in what scenario could we use the gummy bear tear drop implant? Could it be the same 250cc or would we have to increase it, and by how much? Also, if we put in a new implant (I would prefer medium profile and I currently have high profile) would we have to use my armpit incision or could we use the nipple lift incision? And if we use the nipple lift incision, will it cause a worse scar? Please let me know, thanks!
A: If you were to replace your breast implants it would be possible to use your existing axillary scars, particularly if the implant size is not going to increase by any significant amount. While a tear drop shaped implant can be used, they are highly prone to rotate when placed into a pre-existing pocket. So their use in an existing pocket should be approached with that risk in mind. (the textured surface really only grabs fresh pocket tissue not that of a smooth capsular surface that has been created from an existing implant) You would be better served to use a lower profile round smooth which would naturally develop profile closer to that of. tear drop but with no risk of shape malformation with implant rotation.
The nipple lift incision is too small for implant insertion. And even if it weren’t it would end up with a worse scar than would be created from a nipple lift alone.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I started taking Accutane exactly 2 weeks ago – the dose is quite low, at 20mg once daily. I now have a problem / query. I realized I should have had surgery before starting on Accutane. I had an infected jaw implant removed in August 2017 and now, in my eyes, have terrible asymmetry as the jaw implant on the other side is still in place. I cannot wait 12 months to have this corrected (I say 12 months as the plan was to be on Accutane for 6 months followed by 6 months being Accutane-free.) My cheek implants are also contributing to asymmetry (they are visibly misplaced).
My question is – how soon can I have surgery (custom wraparound jawline implant at least) seeing that I’ve been on 20mg Accutane daily for the last 2 weeks?
A: It has long been believed that wound healing may be compromised in patients taking systemic isotretinoin. The cellular basis of this potential adverse effect is that his drug affects the synthesis of collagen which is essential for normal wound healing. Despite this contention, animal studies have failed to show adverse effects in wound healing at doses of 4 mg/kg per day. Case reports and cohort studies looking at facial skin laser resurfacing, facial chemical peels, laser hair removal, rhinoplasty, tooth extraction and ENT procedures have failed to show any demonstrable or consistent increase in wound healing problems.
Does this mean that the purported adverse effects on wound healing by isotretinoin are a myth? It is fair to say that most of the clinical studies reported have very low numbers of patients which makes it difficult to really know if those findings are valid. Equally relevant, none of these clinical studies have involved the use of implants which have natural higher risks of complications and is always the ultimate test of wound healing.
Given that most of aesthetic facial surgery procedures are elective and there remains some doubt that isotretinoin has no adverse effects on wound healing, one should not have surgery while actively on the drug. If you stop the medication now, having been on it for just two weeks, the risks a wound healing problem from having facial implant surgery a month or two from now should be very low.
Dr. Barry Eppley
Indianapolis, Indiana