Your Questions
Your Questions
Q: Dr. Eppley, i lost my left testicle when i was three years old. At the age of 38 i decided to implant a testicular protesis, but with the result i am very unsatisfied. The protesis is to small and very hard, so the feeling is very unnatural. My natural right testicle is about 6cm long and 4,2 cm wide.
I am looking a long time for a prothesis with enough size so it fits better to my natural testicle. On your Home page i found a solution: “Solid Silicone Testicle Implants”.
I want to know, is it possible to buy this prothesis, so my german doctor can implant it? Or is it nessecary to travel to you to replace it? How much are approximately the costs?
Thanks for your reply.
A: I am not a manufacturer/seller of implants. I only make custom testicle implants for patients in which I do the implantation.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, My primary concern in pursuing shoulder narrowing surgery is that I do manual labor for a living and am worried about losing my range of motion as a result of this surgery. I’ve done research into successfully healed double-clavicle fractures where range of motion is maintained, which makes me feel better. Ultimately I’m at a point where some loss of range of motion would be acceptable in exchange for noticeable results.
A: Your concerns are understandable and common but in my experience to date I have yet to see any postoperative range of motion issues after surgery. Nor would I expect such to occur given the much larger clinical experiences in non-surgical and surgical clavicle fracture repair. (not an exact corollary but close)
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve had a lip lift about 4 weeks and even though the distance between muse and mouth is still almost as before the nostrils have been made wider and the base distorted
Will this improve in time or is thus the final result? I’ve added before and after photos
If this is the final result can a plastic surgeon narrow my nostrils to their original size and shape easily and if yes after how many months?
I’m very depressed as I had a beautiful nose by birth and now my whole face seems different and the nose too big for my face!
A: This is undoubtably at 4 weeks the final result as it related to the width of the nostrils…more healing time is not going to make them more narrow. A secondary nostrill narrowing proceduer can be done 3 months after the lip lift surgery.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have infraorbital rim implants already and am currently planning for double jaw surgery to correct bimax recession (I’ll be having lefort 1 and BSSO with counter clockwise rotation).
Is it ok that I have infraorbital implants so far as getting this surgery done? When I’ve seen diagrams for lefort 1 procedures, the screws and plates do extend up into the cheek area (though I don’t think they go quite as far as the orbital rim, but it seems in close proximity). I’m worried when I consult, the surgeons may tell me they need to remove the implants because they are in the way of where they need to secure the plates. However, I have seen that there are multiple variations in the sorts of plates used, with some that do not extend around this area.
A: With the use of standard infraorbital rim implants I don’t see any problem with the performance of a LeFort I osteotomy or the fixation needed to secure it.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, It indeed is possible to remove the existing silicone chin implant, perform sliding genioplasty (should there be a need to that, of course) AND insert a wraparound jaw implant (that would cover the chin too) in the same surgical procedure…(?). if so, wouldn´t that place too much strain on the chin, as it would take the biggest brunt of the surgery (implant removal, genioplasty + new implant)?
- If I gather correctly, wraparound implant can elongate the lower third of the face in the manner ChinWing can…(?).
- As for the fat along my jawline, it´s been almost a decade it has been injected, but it is still very much present and does mimic a facial implant to a degree (ca. 7ml of fat on each side) which is of concern to me for it may interfere with how the final result would look like. Hence my question: could that fat be take out – at least partially – either in a separate session under local anesthesia a few days before the main surgery, or under the same surgery…?
- Finally: silicone or peek custom implants? Which are preferable in terms of patient safety, avoidance of (delayed) infection, aesthetics and easiness of placement on the jawbone…?
A: In answer to your questions:
1) Removing a chin implant, replacing it with a sliding genioplasty and simultaneously placing a wrap around jawline implant does not place excessive strain on the chin. I have done it many times.
2) A custom jawline implant elongates the lower jawline more effectively than a chin wing osteotomy.
3) Once fat is injected in the face it is very difficult to remove. Attempts to do so would require a microcannula liposuction approach done months before the definitive jaw augmentation procedure.
4) A solid silicone jaw implant offers the easiest insertion/placement and eae of revision or reversibility.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I had a genioplasty of 6mm advancement 4 months ago and I still want to get it reversed. Is a full reversal too risky? Will it cause too much skin sagging. I am 19 years old and my first surgery was actually a success except the fact that I don’t like the results. The 3 first pictures here are the post-op 4 months later. Thank you for you answer!
A: I think the risk of any skin sagging with a 6mm sliding genioplasty reversal is fairly low. Skin sagging is more likely to occur from chin implant removal than a sliding genioplasty.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have a rather prominent zygomatic arch, it doesn’t really bother me or anything, but what really bothers me is the fact that my front part of the skull is quite narrow compared to the proportion of the zygomatic arch protuberance, which makes my face have kind of unevenly shaped, by starting wider and progressively narrowing as it goes, forming an irregular oval face, so my question is:
It is possible, through a cranioplasty intervention, to widen my cranial frontal laterals, in order to straighten the sides and muffle the protuberance of the zygomatic arch, following the same width or so, nothing too exaggerated of course, but making the change.
I uploaded 2 photo references of what I am trying to look after.

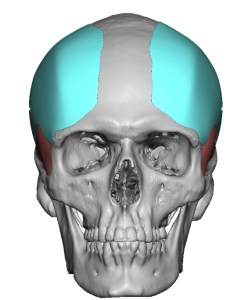
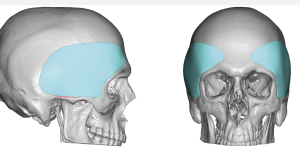 A: You are specifically referring to a family of head widening implants that I commonly perform that run the spectrum of standard anterior temporal implants to custom extended temporal head widening implants. (see attached implant designs) Based on your pictures and description of aesthetic needs it would probably be very similar to the anterior head widening implant design in the 3 to 4mm range of maximal thickness.
A: You are specifically referring to a family of head widening implants that I commonly perform that run the spectrum of standard anterior temporal implants to custom extended temporal head widening implants. (see attached implant designs) Based on your pictures and description of aesthetic needs it would probably be very similar to the anterior head widening implant design in the 3 to 4mm range of maximal thickness.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve been researching plastic surgery for the past couple of months and I’m considering getting several facial procedures done. Recently my eye was caught by clavicle lengthening. My narrow shoulders have been pointed out to me for as long as I can remember and have solidified themselves as a pretty big insecurity. I am 6′ tall with a shoulder width of 16-16.5″ bone to bone. In theory, it sounds amazing, but I have a couple of questions. Would I be able to reach a width of 18″? It’s a bit of an arbitrary number, but I feel like I’d be content with less , as long as I look more proportionate. Since a V-Taper is sought after in bodybuilding, could shoulder widening make it more pronounced? With the shoulder being formed by the clavicle and scapula, how does clavicle lengthening affect the scapula? Does it get pulled alongside the clavicle and could it look unnatural if it’s lengthened too much? Is the clavicles strength permanently compromised after the surgery?
A: These are all great questions in regards to the shoulder lengthening by clavicular expansion osteotomies to which I can say the following:
1) The average in shoulder width by lengthening osteotomies is about 1 ¼ to 1/1/2 inch collectively. (both sides) So going from 16 inchs to 18 inches is not going to occur from the surgery.
2) I think the primary effect of shoulder lengthening is that it makes the shoulders more square in appearance. That effect is more obvious than being wider.
3) Shoulder lengthenng is ultimately restricted by the scapula and its soft tissue attachments. Thus teh scapula is not lengthened or changed in position of any significance. It is the reason that shoulder lengthening can be more than it is.
4) Once fully healed the bone strength should be normal biut that takes a while to get there. (up to 6 months) Of course of one never removes the fixation plate the combined plate-bone unit is more resistant to fracture than the natural bone.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I came upon this website after searching for jaw implants. After seeing some of the custom jawline implants, I noticed one of the patients had a similar jaw issue that I have. I got an opinion from a maxillofacial surgeon locally that after seeing my x-ray he recommended jawline implants due to an abnormal growth of my left side of my jaw. I hope you can help.
A:Your 3D CT scan shows an overall right facial asymmetry (vertical underdevelopment) which is well manifested at the lower jaw. Only a custom jawline implant can make the 3D correction needed. The only question is whether this would be just for the right side or to wrap around to the left side as well if one desires some overall jaw enhancement and not just jaw asymmetry correction alone.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I suffer from nasomaxillary hypoplasia. I was informed that lefort III could fix my problem, and I have the recommendation of you as an excellent doctor. For that reason I’m reaching you to know if it’s possible to fix with implant instead of Lefort 3 and how much would you charge for that. I’m attaching my X-rays so that you could better see my skull.
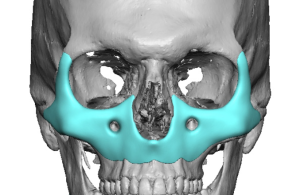
 A: While I would agree that a LeFort II procedure is the most ideal approach to your total midface deficiency, certainly a total midface implant would be a helpful alternative option as a caouflage approach. (treating the symptoms of the problem and not the actual problem) It would not change your existing bite relationship but would for everything above the level of your bite.
A: While I would agree that a LeFort II procedure is the most ideal approach to your total midface deficiency, certainly a total midface implant would be a helpful alternative option as a caouflage approach. (treating the symptoms of the problem and not the actual problem) It would not change your existing bite relationship but would for everything above the level of your bite.
Another variation to total midface augmentation is a combination rib graft and implant. Using the rib cartilage grafts to build up the entire base of the nose and use a custom designed implant for the rest of your face. Such rib grafts could also be used for concurrent augmentation rhinoplasty as well.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, How can my masseter muscle dehiscence be fixed after a custom jawline implant was placed?
A: What you really have is a combination of both masseter muscle dehiscence and, most importantly, what is known as implant reveal. (an implant design issue) Your jawline implant design was destined to have this problem as it violates the anatomic boundary of the masseter muscle. When you make the angle design of the implant go too far posteriorly it will stick out beyond the muscle. While the masseter muscle can elongate vertically you can not increase its width. Thus jawline implant designs that attempt to square out the jaw angle (which is anatomically unnatural) will create an uncovered area of the implant.
The relevance is that you can’t make the muscle go where it has never been. (muscle dehiscence repair) All you can do is volumetrically add to the overlying soft tissue in a camouflage approach. Whether that is best done by fat injections, alloderm sheeting or soft tissue jaw angle implants can be debated.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have a question that greatly confuses me. When I see you talk about implants, you often greatly emphasize that the thickness of the facial tissue has an immense impact on the outcome of facial implantation. I always took this to mean the amount of fat in the face; however, I seen you clarify that the thicker facial soft tissue is not fat.
My question is, if not fat, what makes ethnic soft tissue thicker than others, and is there anything that can be done to thin the tissue?
A: It relates to all components of the soft tissues the epithelium, dermis, fibrofatty layers and the muscles. Can it be substantially thinned…no. Can it be thinned a little by fat removal in selective places…yes. But an overall facial tissue thinness can not the obtained unless the underlying facial bone structure is expanded by osteotomies or implants which stretches it out.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I need your help. I got a facelift (deep plane) in another country. I like the lifting so far, but I ended up with pixie ear deformation. Could you fix my problem? If yes how it is possible? Usually I don’t want to lift again.
A: Pixie ears are a reflection of over tissue resection and/or poor suspension of the lifted tissues. There are only two methods to correct the pixie ear deformity. The simple method is a direct release of the earlobe and repositioning it higher by a V-Y advancement technique. While effective the tradeoff for this simple method is a visible vertical scar line down from the new position of the earlobe down to where it was originally. It may be simple but most patients usually do not want a visible scar. The scarless but more involved method is that part of the facelift needs to be lifted so the skin tucks under the released shortened earlobe position.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, My original right testicle was removed when I was 2 years old because it was not formed correctly. I had an implant put in 5 years ago and I hate how hard it is and would like more information on your soft implant. Thanks
 A: If the testicle implant feels very hard it is undoubtably a saline or older silicone style implant. That feel can be significantly improved by replacing it with an ultra soft solod silicone testicle. The only question is whether this woulkd be a standard implant (5 cms or less in size) or would require a custom implant. (greater than 5 cms in size)
A: If the testicle implant feels very hard it is undoubtably a saline or older silicone style implant. That feel can be significantly improved by replacing it with an ultra soft solod silicone testicle. The only question is whether this woulkd be a standard implant (5 cms or less in size) or would require a custom implant. (greater than 5 cms in size)
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I had a Lefort 1 osteotomy to correct an underbite a few years ago but I’m unhappy with the outcome. I have quite hollow under eyes and flat cheeks with a heavier puffy lower face and no definition. I would like to achieve a more slim and defined feminine look with more prominant cheekbones. I have been researching infraorbital malar implants and also types of fat removal and masseter botox. Would these procedures help me achieve my aim or should I consider something else. Thank you.
A: As can anatomically happen in some LeFort advancements the under eye and cheek areas get ‘left behind’ as the maxilla moves forward as this is a low midface procedure that does not affect the high midface area. Given that maxillomandibular position is now the foundation of your face it would make sense to augment the infraorbital-cheek areas. This will certainly improve the undereye hollows and augment the cheeks. The only question is whether this will have a slenderizing effect on the face…of which I am suspicious that it would. Some of your facial volume concerns comes from the now increased midface soft tissue fullness that is a sequelae of the midface degloving that is necessary for the Lefort I procedure. This is where buccal lipectomies/perioral liposuction/masseteric muscle thinning may have a positive role to play in your facial reshaping efforts.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I was hoping you could please help me understand what I can do to resolve the lower heaviness in my face. Despite being 5’11 in height and less than 135lbs, I still (and always have) carried a lot of weight in my face, which becomes particularly pronounced when I smile. I have had masseter reduction with Botox in the past, which has helped but it’s still not getting at the chubbiness at the front and lower sides of my cheeks. Is this buccal fat, masseter or something else? Photos attached.
A: While I have not seen a truly static picture of your face (all have various forms of smiling which naturally adds to the fullness of your face) your ‘problem’ is undoubtably multifactorial. (meaning the natural thickness of all of your overlying soft tissue…skin, fat muscle, fascia…all make a contribution to the fullness. Thus there is no single one procedure that addresses just one of the tissue components that is going to successfully provide a satisfactory facial thinning effect.
The reality is that the most successful facial thinning procedure I know is the one you would be least motivated to do and one that seems counterintuitive…. a cheek-jowl tuck-up. (a limited form of a lower facelift) This is the most effective approach for facial fullness reduction because it has a known facial sweeping effect, which for an older thinner person may not be a desirable facial change, but in the younger fuller face patient is a positive effect. By tightening the skin, underlying SMAS and removing some buccal fat the face becomes less full.
That being said every other procedure, stand alone buccal lipectomy/perioral liposuction and masseteric muscle/jaw angle reduction provides some modest improvement but never a really significant change.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, My breast implants were put in 1997, I am 64 now, never an issue, they are still soft and no pain at all..but want them out, but cant afford that. I believe they were 350cc. I need a mammogram but refuse the one where they smash you down! i am too afriad of that. Yes, they are old but intact for sure..if they were not intact would’nt my implants be totally deflated? they re still full and round! But if I do this mammo, and they smash em down—I may just invite issues for myself as they might burst…eeek! I cant do that. I read where you wrote a lady back as she had implants that were 31yrs old and you said the shell is not intact any longer anyway…..but….mine is intact or my implants would be deflated correct?
A: Are they silicone or saline breast implants? I assume since they were placed in 1997 they are saline implants. If so then of there was any loss of integrity of the implant shell they would deflate or be flat.
Dr. Barry Eppley
World Renowned Plastic Surgeon
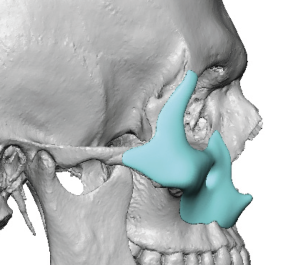
Q: Dr. Eppley, I am interested in tear trough infraorbital/paranasal implants post orthognathic surgery. My goals are : a positive orbital vector, elimination of dark circles, mitigate areas “left behind” after subspinal lefort I.
A: Most likely you are referring to infraorbital-paranasal midface implant design to fill in what the LeFort I osteotomy did not accomplish. The area of implant coverage is really determined by what you want to see augmented on the outside. The 3D CT scan is merely the platform on which the implants are designed but they don’t necessarily show the desired external aesthetic effects.
While the infraorbital region can be augmented it would be unlikely that the dark circles will be significantly improved….unless a major component of the dark circles is shadowing.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I have really close set eyes and I’d like to get them further apart. I want to get around 6-8mm of extra pupillary distance. Could this be achieved with some sort of implants in the eye orbits? Or in any way that doesnt involve a craniofacial surgery? Thanks.
A: Only orbital box osteotomies done through a frontal craniotomy can achieve that increase in interpupillary distance.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have been on testosterone replacement for ~25 years and have atrophied testicles. I was interested in the wrap around technique; however, after reviewing blog entries, due to the small size of my testes side by side implants would be appropriate. I would be surprised if my right, and larger of the 2, testicle is even 2.5 cm in largest diameter.
I am concerned that with the degree of atrophy that my scrotum has shrunk considerably as well which may limit the size of implants that can be used. I would want the largest implants up to 6 cm that could safely be used.
A: With your small testicle size you have correctly assumed that the side by side technique is the best testicular enlargement method. I see no problems with placing 6cm size implants as the scrotal tissues are very elastic. This procedure is done under general anesthesia.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am considering to do the mouth widening procedure that you offer but was wondering how much of the mouth can be widened? Can 8mm be taken by both sides? And can a corner of the mouth lift be done at the same time?
A: 8mms is too much per side and will lead to poor scarring. When doing a corner lift at the same time as widening the movement is at 45 degrees to the horizontal plane. But with the 45 degree movement the amount of horizontal widening will be a bit less.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, hello doctor, I would like to know if after a cheekbone reduction surgery it is possible to place implants, because my face is very wide, but the cheekbone does not project forward, only laterally, and I want to do both but I don’t know if that would be possible, I wait for your answer, thank you very much.
A: The concepts of cheekbone reduction and cheek augmentation, done concurrently or separately, is not incompatible. Cheekbone reduction involves narrowing the width of the cheeks only by osteotomies to bring in the width of the zygomatic arches. Conversely, cheek augmentation can be done on any aspect of the cheek which in your case needs to be done on the anterior aspect just below the orbital rim. As a result you can get anterior cheek projection while decreasing lateral cheek width.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I’m just wondering if you can rebuild jaw bone ? I don’t mean by adding jaw implants. My jaw bones are very thin and just wondering if he’s able to rebuild jaw bone back up?
A: The key question is why is the jaw bone thin? If it is naturally thin then trying to build it out even with bone grafts will fail/be absorbed. if it is thin by some process (was once thicker) than onlay bone grafts may be more successful.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hello I’m from Vegas, I came upon this website after searching for jaw implants. After seeing some of the custom jawline implants, I noticed one of the ‘skulls’ had a similar jaw and issue that I have. I got an opinion from a jaw surgeon here in Vegas after seeing my x-ray he recommended jawline implants due to an abnormal growth of my left side of my jaw. I hope you can help, take care and have a wonderful day.
A: Any time there is asymmetry of the lower jaw, a custom implant approach for augmentation would be the best approach….although a custom jawline implant is always the best approach regardless of whether asymmetry exists or not.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I hope this email finds you well. I stumbled upon your Instagram while browsing for possible custom facial implant surgeons, but unfortunately, you are in a different country than mine and I am unable to fly out, by any chance can you consult with me online and help design my implant and I will get the surgery performed locally? If that would be possible I would highly appreciate it. Thank you.
A: I only design custom facial implants for patients in which I also do the implantation. The success of any custom facial implant is a combination of a good design and proper implant placement. A good design becomes compromised if improper placement is performed…which is often what happens when a surgeon with no involvement in the design or experience in placing such implant designs performs the surgery.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am about ready to proceed with a consultation for Pec Implants. I was curious about the PowerFlex Plus Pectoral implants. I note that they are 15cmx19cmx3.9cm in a vertically placed position. Looking for the maximum augmentation, I believe this model/size in terms of projection would be ideal. However, I do not think my chest height could accommodate the 19cm height. Could the implant be place horizontally or could it be shaved to fit my dimensions? Thank you so much!!
 A: The proper orientation is as shown in the attachment with the vertical height of 15cm and the horizontal orientation of 19cms with the tail towards the axilla. While the implant can be cut to reduce its dimensions I generally try to avoid doing that unless absolutely necessary as have a cut edge of an implant increases the risk of a chronic seroma. (fluid collection) When very specific dimensions of a pectoral implant is needed, this is the role of a custom pectoral implant design.
A: The proper orientation is as shown in the attachment with the vertical height of 15cm and the horizontal orientation of 19cms with the tail towards the axilla. While the implant can be cut to reduce its dimensions I generally try to avoid doing that unless absolutely necessary as have a cut edge of an implant increases the risk of a chronic seroma. (fluid collection) When very specific dimensions of a pectoral implant is needed, this is the role of a custom pectoral implant design.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have a question on minoxidil topical solution and the implant placed in 2019. If you may share his thought on this, it would be really helpful.
With likely having male pattern hair loss condition, I apply minoxidil topical solution 5% (e.g. Rogaine) or sometimes 7% on scalp for stimulating hair growth. I applied the solution daily since 2015 and I am likely to continue in the many years to come.
I am not sure if this would be true but I would imagine long-term application like this, while some minoxidil topical solution (incl. active and other ingredients) is absorbed into blood stream or other via channels, certain amount would be left as residual and stay among the layers of scalp skin. If this makes sense, then when it happens, such residual may penetrate through the layers of scalp skin, and reach the bottom level of scalp skin. As this level of skin is in direct contact with the surface of implant, so do some topical solution residuals.
As I guess the implant would not absorb minoxidil, it continues to build up on the surface of implant.
I wonder if my understanding above is reasonable.
Then my question is whether such build-up of minoxidil topical solution under scalp skin (above surface of implant) would cause any health issue in that area. If yes. What should I do to avoid such issue or mitigate risks involved.
Any additional comments on this topic would be helpful.
Thank you for your kind attention : )
A: I am not aware that minoxidil builds up under or in the scalp. It is a vasodilator that is absorbed and eliminated after it has its effects.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Five months ago, I underwent double jaw surgery together with V line and cheekbone reduction surgery in South Korea. The result of the surgery was not what I expected, and I have regretted it since. My facial aesthetic appears to be much more feminine and much less attractive compared to pre-operation. I have been finding ways to see if it’s possible to reverse my surgery so I can look like my old self again. I’m planning to reverse my v-line and cheekbone reduction by using a customised silicone wrap-around jaw implant, and have the zygomatic body elevated back out /customised cheek implant after doing a revising double jaw surgery to push both my jaw back out. I have a few questions that I hope you can help me to address.
1) Do I need to visit you to check if I’m eligible for a customised silicone wrap-around jaw implant and customised cheek implant before I decide to do a revision double jaw surgery to push both my jaw back out?
2)Is there any chance I’m not eligible for a customised silicone wrap-around jaw implant and customised cheek implant after revision double jaw surgery?
A: I have done many patients such as yourself who are looking to reverse their V-line surgery. I have yet to see such a patient who could not have a custom jawline implant to reconstruct their jawline.The same would apply to the reversal of cheekbone reduction osteotomies. Such surgeries would, of course, await your revised double jaw surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,Hey, I read about your practice in a 2019 New York Magazine article… I’d like to get more information on the testicular augmentation “clam shell” implant — e.g., cost of procedure, recovery time, possible complications, detectability by others, effects on testosterone production, etc. Haven’t been able to find that info on your website. Thanks!
A:When it comes to aesthetic testicular enlargement there are two methods: side by side and the wraparound or clamshell implant approach. While the latter has a lot of understandable appeal it does have a significant rate of postop separation which, as a result, always makes it my second choice. I have yet to figure out as assured design that makes postop ‘disengagement’ a negligible or almost non-existant risk.
Otherwise either form of testicular enlargement has no adverse effects on testosterone production and is certainly not easily detectable in most cases.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I have just a major question for Dr. Eppley (maybe he can answer it on his blog)?
I am considering getting either orthognathic surgery (I have been given the option of DJS or LJS), which would be covered by insurance due to my mild sleep apnea and TMJ, or doing a genioplasty and rhinoplasty with you. I have a class 2 overbite + I don’t like my small chin, and the jaw surgeon recommended a LeFort 1 with CCW rotation and possible 5 mm advancement, and up to a 10 mm BSSO advancement of my lower jaw once my teeth have been put in braces.
One concern that I have seen folks getting upper jaw advancement/impaction present with is sagging cheeks and more pronounced undereye circles. This seems to happen due to pre-existing flat cheekbones and lack of orbital rim support (which I think I may have). I have attached photos below of me pre-filler. With my existing facial structure, would the risk of my malar fat looking “droopier” be there?
A:Your fundamental question is really about the concept of surgical tradeoffs. The exact midface/cheek concerns you have expressed are very likely to happen as the cheekbones get ‘left behind’. It is a very common aesthetic sequelae in Bimax advancements and while the chin may look better the midface will pay the price for that exchange. Bimax surgery is worth it if significant functional improvement is needed (sleep apnea) or the lower 2/3s of the facial skeleton is recessed and needs to be moved forward. (fat face) In our case it really comes down to the value of sleep apnea elimination and correction of your Class 2 bite. But inevitably it will not be your last surgery as the undereye hollows and the cheek deficiency and low soft tissue cheek fullness that results may likely be undesired aesthetic effects.
Dr. Barry Eppley
World-Renowned Plastic Surgeon