Your Questions
Your Questions
Q: Dr. Eppley, I may need to remove my silicone cheek implants placed with screw. I may need a facelift during the removal.
A:I believe your concern with the removal of your cheek implants is that some cheek tissue sagging may result…which is a legitimate concern since the osteocutaneous ligaments have been detached for the placement of the implants. In that regard there are three potential strategies to consider to mitigate that potential issue.
1) Remove the cheek implants and see what happens with healing. Such cheek sagging may or may not occur depending on the size of the implants and their actual location.
2) Remove the cheek implants and replace with smaller ePTFE cheek implants. The smaller implant will still provide some tissue support and the ePTFE material allows tissue ingrowth to give the overlying tissues something to hold onto unlike the silicone material.
3) Remove the cheek implants and do a temporal cheeklift.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a young man from Europe. I have a question for you if possible. My biggest insecurity arehow wide my face is wich i Think is ddtermined by how wide my cheekbones and temples are, and also my jaw. My biggest doubt is if it is possible to make it any narrower. All patients I’ve see having reduction procedures are asians, and although they look wonderful i feel like our anatomies are different. For instance their problem has usually to do with how their cheekbones arch, while mine i think is directly at the roots of the cheekbones ( I might be wrong this is why i’m asking you).
A: I think the fundamental question is whether your face would benefit by cheekbone reduction osteotomies given that the temples above it will remain the same. (forget about for a minute how technically possible it is and that requires a 3D CT scan to determine and not plain x-rays) The best way to make that assessment is computer imaging. (see attached) Your reaction to that prediction will answer that question.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My goal is to have a more defined long term, permanent chin. In which case my chin would align with my upper lip and or nose as it should. In most cases my side profile looks like a straight slope and no chin. The TMJ clinic believes it is not in my best interest to have a foreign body implanted due to my past history of JIA. It seems as though a plate and screws that would be used for a sliding genioplasty is not a foreign body, which I do not entirely understand. They are unable to say for certain exactly how much they may be able to extend my chin with a sliding genioplasty and I am concerned if I go through the surgery and the chin is not slid forward enough for the look I’m wanting, it would be a waste of money and unneccessary risk with my JIA. They are unable to do a picture of what it should look like upon completion to help with my decision. I would like to know if you believe I can accomplish the look I’m wanting with merely a sliding genioplasty since I am unable to go forward with an implant for health risks and reasons.
A: Having treated numerous extremely short chin patients, including RA patients, the first thing you have to realize is the magnitude of your chin deficiency…which is really a jaw growth deficiency of which the chin is but a symptom of it. Avoiding an implant in such a short chin is a good thing even if you didn’t have RA so a sliding genioplasty is the correct procedure for you. Secondly the actual measured chin deficiency, as defined by your own goal of bringing the chin out to a vertical line dropped down from the lip is probably in the range of 25mms or an inch. The sliding genioplasty is based on moving the entire thickness of the chin bone forward. In your case you need what is known as a ‘jumping genioplasty’…which means putting the entire thickness of the lower chin bone in front of the bone above it as opposed to a traditional sliding genioplasty which just pushes it forward along the cut line. (this also prevents the chin from getting vertically longer) This is what I do in cases of extremely short chins. But even with this procedure the amount of forward chin advancement is limited to the thickness of the bone which is probably in the 10 to 15 mm range.
This is the anatomic explanation for why your ideal result can not be achieved as you have imaged it as it is beyond what the bone thickness will allow. More achievable is a 50% to 75% amount of what you have imaged.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have recently undergone fat transfer to my under eyes as well as canthoplasty. Is there a cheek implants that targets the zygos-malar region for men that I can still use or is this not possible since I had canthoplasty and fat transfer.
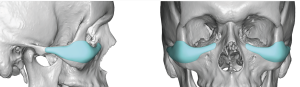 A:You are referring to custom cheek (zygomatic)( implants which can have infraorbital extensions anteriorly and zygomatic arch extensions posteriorly based on the patient’s aesthetic needs. There are endless variations of this midface implant concept. This style of midface implant is the most common male midface implant that I do. Having had lateral canthoplasties and undereye fat transfer does not preclude having this implant placed even through a lower eyelid incision.
A:You are referring to custom cheek (zygomatic)( implants which can have infraorbital extensions anteriorly and zygomatic arch extensions posteriorly based on the patient’s aesthetic needs. There are endless variations of this midface implant concept. This style of midface implant is the most common male midface implant that I do. Having had lateral canthoplasties and undereye fat transfer does not preclude having this implant placed even through a lower eyelid incision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am sure you are aware of the new craze around “hunter” masculine eyes. Is it possible to achieve this look through orbital rim implants or any surgical procedure in general or is it purely genetic? Many Thanks.
A:Trying to achieve a Hunter Eye Look is a common male eye periorbital reshaping request today using custom implants and eye corner surgery to try and achieve. How successful that may be heavily depends on one’s starting point. For some patients it is achievable, for others it is not. How that applies to your ability to achieve it requires pictures to make that assessment.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Interested in forehead reduction surgery.
A:Thank you for sending your pictures. You have bilateral prominent forehead eminences (horns) which is the obvious basis for the pursuit of forehead reduction surgery. In consideration of such surgery there are two determinations to be made. First, what is the thickness of the forehead horns and can they be adequately reduced based on this bone thickness. This requires a 2D skull scan to make that determination. Secondly, where is the incision going to be placed through which the reduction can be done? It has to be either at the frontal hairline or just behind it which poses a bit of a technical challenge given the distance between the hairline and the prominent bony area.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, i have untreated sagittal craniosynostosis as a child. it has always bothered me greatly I’m in my early 30s now and seeking help form somebody that may be able to help me.
Thanks for your time.
A: Most adult sagittal craniosynostosis are treated by a custom skull implant with potentially some bone reduction of the sagittal and occipital skull areas. Whether all of that applies to you I. can not say without knowing what you look like.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Calf: I would like a muscle augmentation from knee to ankle.
Forearm: Muscle augmentation from elbow to wrist.
Could you please confirm if a longer implant is feasible in both areas in your clinic.
A: What you are seeking can not be done. In the lower leg and forearm the upper half of the length of the extremity can be done…not the full length as you have indicated.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can I get facelift and lipectomy and necklift/lipo? Goal is tighter and thinner look. I have loose tissue cheek area after having buccal removal annd malar implants put in back in 2022.
A: As a general rule you can’t lift your way into improved facial definition, at least not in the cheek area due to the lack of good incision locations to do so. Simulating a cheeklift with your fingers over the cheeks is not representative of the effects of what a lift can do. Rather it has to be done back where the lift is actually performed in front of the ear and up in the temple areas.
I would be very cautious about any form of a lift as I have seen many a young person who had a ‘facelift’ and now has hypertrophic scars and a minimal result. The tissues of a young person should not be confused with an older person who has lost elasticity and scars better with a more sustained lifting effect. Liposuction and further defatting efforts are fine and will produce a modest improvement but it is not achievable to expect any form of surgery to do much more with your naturally thicker soft tissues.
You don’t want to attempt any soft tissue refinement/sculpting until all the implants are successfully implanted as swelling will work against these efforts.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a male patient considering lip augmentation. Given that I have identified I do not have the right shaped lip for a bullhorn lift, I am interested in the vermillion advancement procedure you have written about.
My only reservation is the risk of bad scarring, such as a keloid, forming at the edges (which presumably would be irreversible and completely ruin a persons lip). Could you please explain the likelihood of this risk please.
Many thanks!
A: I have never seen a lip keloid from an aesthetic procedure in any gender or ethnicity so that is not a real concern in my experience. Like all lip advancements there is always the risk of some scar visibility which may require a revision. Interestingly that risk is higher in women than men because of the presence of beard skin into which the vermilion edge is advanced.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, just wondering if I can send a picture so you can let me know if a brow bone implant is appropriate for my issue? I damaged my brow as a kid and have become increasingly self conscious of the indent and lack of symmetry it caused in my brow. I don’t know what I can do about it and am just looking for a route forward.
A: With your brow bone asymmetry you have correctly surmised that an implant augmentation would be the best approach, particularly using a custom brow bone implant design made from a 3D CT scan of your forehead. It would be placed using an endoscopic technique.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am hoping that you can help. I have previously had Medpor Malar cheek implant surgery done through the mouth, upper/ lower eyelid blepharoplasty procedures in the past 6 months. However I am not satisfied with the results, one implant is oversized to the other. Would you be able to help correct my condition to help improve the asymmetry in my face?
Thanks
A: Thank you for the implant info. Because two different cheek implant sizes were placed I assume you have some cheek asymmetry to start. Like many ‘eyeball’ implant techniques for fixing facial bone asymmetries the asymmetry is not solved and is often more apparent than before. While it would be prudent to get a 3D CT scan to understand the bone and implant differences between the two sides, Medpor material rarely shows up on 3D CT scans. So there is no way to know with accuracy whether the right cheek implant has a size, placement or a combination of both problems which account for the asymmetry from the left side.
The ‘simplest’ path forward is to eyeball the asymmetry correction, remove the implant, modify in size if needed and do an immediate replacement in the same or different position. While this is not mu usual recommended facial implant modification technique it is the most practical one given the implant’s material composition.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I was tested for Noonan’s syndrome and tests came back negative. I have lived with a relatively mild variation of a webbed neck since I was an infant. Judging from the pictures attached to this email.
A: In cases of mild/moderate webs in a male I am less than enthusiastic about webbed neck surgery in these cases for 2 reasons:
1) The indirect central diamond excision on the back of the neck leaves a visible which, while in a female with long hair remains hidden, that would not be the case for a male.
2) In my experience moderate non-syndromic neck webs are the most resistant to sustained change because the tissues are often stiffer and less mobile which makes for the potential of some relapse.
I would not say I would never do webbed neck surgery in the non-syndromic patient but we have to be careful about creating a visible scar if we can’t get significant improvement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Upon reading your jaw augmentation page I stumbled upon the Chin wing osteotomy. I was wondering if you do this procedure yourself.
A: I do perform the chin wing osteotomy provided the patient is properly qualified for it which requires two criteria:
1) That they understand that the chin wing osteotomy is an incomplete or partial jaw augmentation procedure. It does not change the jaw angle area in either width or vertical length. It provides moderate horizontal and vertical augmentation to the chin and body of the mandible but makes no changes to the posterior or jaw angle area. Think oif it as an extended sliding genioplasty noit a total jaw augmentation change. This is why it is appropriately called chin wing and not a jaw wing procedure.
2) A preoperative 3D CT scan is needed to determine the location of the inferior alveolar nerve in the lower jawbone and thus where to safely placed the osteotomy cut.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Seeking Chin Implant Revision, Custom Implant for a more square, symmetrical and masculine appearance.
The implant was placed about 4.5 years ago. The implant was in a size ‘large’ and was a silicone material; placed sub-mental (small incision under chin). The brand of the impact was Implantech Associates, Inc. Some information: Reference: CEAC-L
Although I have no regret about getting this implant initially, it did bring the necessary harmony to my overall appearance by bringing my chin forward however, the reason for seeking a revision is because I believe the implant had either shifted slightly (based on images from a CT scan) or was placed in a position that caused some asymmetry (the chin leans more towards my left side) which was not an issue I had before the implant. My natural chin was receded however, was more symmetrical and had a square shape to it. Which brings me to my second reason for a revision, I would like to see what my options are for a square-shaped implant. I would like to have a more masculine square chin shape instead of the rounded one I currently have. I do believe that it would complete the facial aesthetic goals that I have for my face. I have read some articles by Dr. Eppley online and am excited to see what he believes a realistic goal would be for me.
A: You have a Conform Extended Anatomic Chin Implant – Large – 6mm projection
Between getting the implant centric and achieving a more square appearance, the two options are:
1) a custom chin implant design
2) a standard Type 1 square chin implant
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a few questions – could you please help with these?
- When I smile, I have creases that form under my eyes every time. Would the under-eye implants eliminate or reduce these?
- Is there anything that can be done to the under-eye implants to further minimize my nasolabial folds? If not, I understand, but I’ve heard of injections along the cheekbone to reduce those folds, so wondered if that was possible with the implant
- Is it possible to create a chin dimple with the custom jaw implant?
- The image that perhaps looks the strangest to me is this one (below). If I had to be critical, it makes me look a tiny bit like a witch because of how pointy the chin seems to be. Perhaps the surgery results would look better / slightly different. But a couple of related / follow up questions:
- Is it because perhaps the chin is too narrow / pointy from the front (needs to be wider?)
- Is there a different procedure other than a sliding genioplasty that would split my jaw / mandible between the chin and the gonion, thus advancing the entire jaw and lower lip, and therefore make the chin less pointy but still giving better projection? I would trust Dr Eppley’s opinion if this is ill advised. My family has a big problem with double chins so wondering how to address this
5) Finally, I recognize it may be very difficult to get my facial shape to change so drastically, but I’m wondering if there’s something that can be done to approach an aesthetic closer to the image below. Is it a matter of making the cheekbones higher and the front of the face more flat? I don’t expect I can be turned into the below very easily, but just wondering if Dr Eppley has any insight if there is anything else that could be done to get closer to this.
A: In answer to your questions:
1) No. That is a dynamic issue while the implant provides static volume enhancement.
2) IOM implants will not improve nasolabial folds. This is a soft tissue issue not a bone-based one.
3) Chin dimples are muscular defects in the soft tissue chin pad, they have no bony basis for them.
4) That is an imaging artifact and not what the surgery would do.
5) You can become that picture or even close to it. All you can do is simulate the bone structure on the face you already have.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’d like to inquire about procedures for improving narrowly spaced eyes. My narrowly spaced eyes have been a lifelong insecurity and it increasingly negatively impacts my disposition. I understand that procedures to improve this trait are risky (orbital box osteotomy), but I am tremendously motivated. To put the extent of the trait into numbers, I have measured a few lengths:
intercanthal distance: 27.5 mm
interpupillary distance: 59.5 mm
bizygomatic width: 141mm
eye spacing ratio: 59.5mm/141mm = 0.421
My intercanthal distance alone is below the range considered normal in the population (>28mm), and is thus abnormal. Furthermore, having narrowly spaced eyes makes my face appear longer and thus more masculine, making it more difficult to live as my desired gender.To provide an actual goal in numbers, I’d like to aim for an ES ratio of 0.46 – 0.47. To achieve this, I’d like my interpupillary distance increased by 5mm.
A: You are referring to orbital box osteotomies as you have noted. This is not a ‘risky’ surgery medically, it is just a procedure where the ‘effort vs reward’ ratio is tilted a bit unfavorably. Meaning you have to do a big operation to make a small change. (5mms) The most effective orbital box osteotomy is a transcoronal approach using a frontal craniotomy for exposure with a 360 degree osteotomy…but that is a bit extreme for a 5mm interpupillary change. The more appropriate technique is a modified subcranial 180 degree orbital osteotomy which has less aesthetic risk and can be done through a combined lower eyelid and intraoral incisional approach.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 55 year old female located in Oklahoma. I recently had a small button chin implant removed after 30 years along with a neck lift. My surgeon replaced it with a large terino chin implant. I was not expecting it to be so large. It was very uncomfortable and the wings pulled downward. After a great deal of pain, my surgeon removed it and replaced it with a medium anatomical implant. This implant is off center with the midline on the right corner of my chin. It is also under the skin and not the periosteum. My surgeon said that it must have shifted but I don’t think the midline was ever centered. Anyhow, it does not stay in position and it falls below my jawline. I am having to hold or push it back it to position constantly.
My first implant never gave me any issues. It stayed in place and didn’t move.
My surgeon said he would remove it but he would not replace it. I don’t know if I should let him remove it as I’m sure my chin will sag.
Or, should I have another surgeon replace it at the same time that it is removed?
Can you advise? Thank you!
A: I am not sure what the compelling motivation was for the original chin implant removal and replacement but not that such a large implant pocket exists and the implant is not secured with screws….it is going toi move around. This is the result of downsizing from a larger implant where the ligamentous attachments have been released. (and they don’t reattach)
Given that you have always had a chin implant there siomply removing it will ljkely create some chin pad sag. I would replace it with a more appropriate chin implant (no wings) and secure it into position with microscrews to an end to this chin implant saga.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I wrote to you a while ago that I was interested in replacing Medpor mandibular angle implants with custom implants.The thing is that after visiting a surgeon he told me that the medpor implants I have caused my masseter to tear and the area has become too skeletal.
Therefore, I wanted to know if you have experience repairing the masseter after removing the implants. Also, I wanted to know if this operation could be performed at the same time as the placement of the new implants or would we have to wait for the masseter to heal properly. Thank you very much for your time.
A: As a general statement once the masseter muscle is dehisced /torn it becomes shortened and scarred and its repositioning is very challenging. I have found masseter muscle repair to largely be an operation with a low chance of success.
That chance of success is improved if implants are being removed but those chances decrease significantly if implants are placed at the same time.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hey!! I have seen cheek arch implants done by dr eppley!! I just wanna know can cheek arch implants be 1 inch in size ?? As i have read on your website that it must be 5 mm in thickness, but i wanna know can it be 20 mm in thickness??
A: I have done cheek arch implants as large as 15mms but not 20mms.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to ask, in general, what is the maximum upper jaw advancement movement in mm (Lefort 1) that will not cause discrepancy between the lower and upper midface and that will not disrupt the facial harmony?
A: This is a question that would be affected by many factors most notably the shape of the face. Thus a specific answer can be provided to a general type question without pictures to understand the basis of your question.
Dr. Barry Eppley
World-RenownedPlastic Surgeon
Q: Dr. Eppley, I am interested in getting a combination of surgeries done. The surgeries I am interested in consist of shoulder narrowing plus rib removal and iliac crest implants.
Could these surgeries be done at the same time? And would I require assistance from another person (ie family member) or friend to be present for my recovery?
A: All three such body contouring surgeries, shoulder narrowing, rib removal and iliac crest implants, impose a lot of stress on the body and make for a very difficult recovery, particularly when you have early limited use of your arms. Thus these trio of body contouring surgeries should not be done together. Any two of them at the same time is commonly done and that is enough of a recovery on its own.
In regards to coming alone or with someone it can be done either way and we see both commonly. Suffice it to say, particularly with shoulder narrowing surgery, that having someone with you makes the recovery a bit easier and you would likely return home a few days sooner due to the added assistance. When you come alone we just have to put more forethought into your immediate postop recovery management as we have to provide some support for it.
Dr. Barry Eppley
World-RenownedPlastic Surgeon
Q: Dr. Eppley, I am curious about ribcage narrowing. Removing my floating ribs wouldn’t make much difference I don’t think. It’s my side ribs that bulge out making my back too wide for my narrow frame. I have no fat really.
It’s rib 10,9,8. My floating ribs do not show much because my side ribs stick out. The sides of my ribs feel hollow.
My hips and legs are extremely small My ribcage is narrow from the side. Looked like the ribs squash sideways slightly.
A: Rib removal of the non-floating ribs is more limited than the floating ribs. Rib #10 can be partially removed as it wraps around the side of the torso and rib #9 can be shaved down in the same side torso area. This is the maximal ribcage reduction/.narrowing that can be done. I would also agree that removal of ribs# 11 and #12 is of no benefit to you in what you are trying to achieve.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I wan to reduce the size of my face as it is larger than a normal human being as its size is extra large.
A: I don’t see any effective method for reducing the size of your face. What makes your face ‘large’ is the amount of thick soft tissue over it. There are numerous defatting procedures and even that of skin reductions (aka facelift) but the question is how effective they would be in making an overall facial size reduction. I suspect they would help make it a bit less full/thinner but not necessarily smaller in size.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Here are some pictures of my face. Based on these would it be possible to say that the lefort 1 surgery affected my facial harmony?
A: Every Lefort I osteotomy alters the natural shape of the face essentially leaving what lies above it behind. (infraorbital-malar region) Your current facial pictures certainly reflects that postop issue.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My breast implant size, I think there is 250 in one and 235 in the other. They are saline, probably close to 15 years old. Yes, I would like to go up in size.
A: Thanks for the info. To see an appreciable/visible increase in breast size you should at least go into the breast implant sizes of 300, probably 350 to 375cc. Always more than a 30% volume increase its needed to see a difference.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, As you can see I have the side of the skull on the right in the photo and on the left in life larger than the other. What I would like would be to refine and reduce this side so that it is homogeneous with the other side.
A really flattened skull on the left with a bump while the other side is normal. I would like to know if it was possible to do something or if it is impossible.
Know if we could raise the skull at the back of the left side so that it is less flat and much more aesthetic.
A: As part of your plagiocephaly there are differences between the shape of the two sides of your head. The options are to either reduce the larger side or augment the smaller side. That is a personal choice based on one’s aesthetic preference.
The flatness on the back of the head is a classic concern in plagiocephaly which is commonly treated by a custom designed skull implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I’m interested in both the cheekbone reduction and double eyelid surgery. Therefore, I was wondering which one should I do first? Lastly, how soon could I have the plates and screws removed and is shaving of the Zygoma cheaper than L-Osteotomy method?
A: The order of cheekbone reduction and double eyelid surgery is a personal one and the two, while anatomically close, are not related or affected by the other. The one you do first is the one that is most important to you.
Shaving of the zygoma is usually a poor choice for many cheekbone reduction patients as its effects are more limited and is a procedure that is not aesthetically interchangable with cheekbone reduction osteotomies. They each have different indications for the cheekbone reduction patient.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 42 year old male. I follow you on Instagram. I would like a consultation about my right clavicle. When I was 8 years old, my father had me fire a rifle that caused a greenstick fracture on my right clavicle. The callus makes a prominent bump as you can see in the pictures attached. I work out a lot, but there is asymmetry. I would like to know if it’s possible to fix the clavicle and add chest implants that would improve the appearance of the upper chest.
‘A: Clavicle Reshaping and pectoral implants can be done together. I suspect the bump is either a hyperostosis at the fracture line or it developed a slight bend at the fracture site. Either way the bump can be likely be shaved. down/smoothed over without compromising the integrity of the clavicle. I would check a clavicle x-ray to have a full understanding of what the bump is.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, For my plagiocephaly compared to the side of the skull I think reducing the bigger side is a better solution. The back of my head will have to be cohesive with the side reduction by increasing the flatness. I also have a few questions to ask you about the risk of this delicate operation since it touches the head. Are there any infectious risks or any other risks? The intervention keeps the desired outcome alive. I mean, aren’t implants changing over time? and Does this procedure present a risk on the nature of the hair or causes it in loss. Recovery after the operation is it essentially pain or difficult? And keep your big scar for life ?
A: The amount of the bigger side that can be reduced will be determined by the CT scan but almost assuredly it can not be done enough to match the other side. As a result reasonable symmetry is not going to be obtained by bone reduction alone.
I have never yet seen an infection from any form of skull reduction or skull implants.
Skull Implants are structurally stable and do not change over time.
Skull reshaping surgery does not adversely affect hair growth.
Recovery after skull reshaping surgery is neither painful or difficult.
Scalp scars from incisional access are permanent.
Dr. Barry Eppley
World-Renowned Plastic Surgeon