Your Questions
Your Questions
Q: Dr. Eppley, Do standard implants placed after genioplasty have a higher rate of infection/complications (such as erosion, shifting, or poor fit) compared to a standard implant placed on a non-augmented chin? Would a custom implant be preferential in my situation based upon these factors, or would it be more of a personal/aesthetic preference instead? In general, are custom implants less prone to shifting/erosion/infection than off the shelf implants in your experience?
Thanks for the help!
A: The value of custom facial implants (including custom chin implants) is in their ability to create a type of chin augmentation effect that otherwise would not be possible with standard implants. Because of the custom design process they may be less prone to intraoperative malpositioning because features can be built Into them are useful for placement in surgery. Otherwise they share all other similarities with standard implants.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I feel like I have a weak chin that makes my nose look out of proportion with my face. I was curious to know how i could fix this with a sliding genioplasty or with a chin implant. Also the amount of movement (if its sliding genioplasty) and the rough cost?
A: The key decision in whether a chin implant or a sliding genioplasty is preferred is based on the dimensional requirements needed for the desired chin augmentation effect and the patient’s emotional affinity for one vs the other. For men the key defining dimensional issue is often chin width. (and that is certainly true in your case as the horizontal need can be meet by both methods and you need no vertical lengthening) Does you want to keep the current chin width or make it wider or more square? Only a chin implant can make it wider/more square as a sliding genioplasty may even make it a bit more narrow.
As for the amount of horizontal augmentation that is determined by computer imaging as well as preoperative measurements which becomes most relevant when a surgery date is planned.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was wondering for the clavicle lengthening surgery does a patient need to have straight shoulders for this surgery to be possible? I notice clavicles are either straight or sloped. I was wondering if this effected anything and if it mattered. Thanks.
A: The shape of the clavicle does not matter as no clavicle is perfectly straight. All clavicles are s-shaped. The portion of the clavicle that is cut, bone grafted and plated, however, is straight.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m interested in a buttock reduction. I’ve always had large buttocks growing up and during bodybuilding squatting has attributed to that. I don’t work out anymore. If possible I’d like to have a much smaller and flat buttocks. I’ve read Vaser and skin removal is the process. However are there any dangers around the gluteus that would occur during this surgery as I know BBL surgeries have risk of fat embolism and if there’s muscle around my gluteus I assume this can not be removed?
Thank you
A: Thank you for your inquiry and detailing your buttock reductions goals. You are correct in that reduction of buttock subcutaneous fat and a lower buttock skin tuck are the only surgical techniques that can be of benefit. Buttock or gluteus muscle is never removed. Buttock liposuction has no medical concerns unlike BBL surgery in which fat is injected under high pressure into the muscle. (which is not done anymore) Liposuction is the reverse, it is removing fat. Its only concern is of an aesthetic nature which applies to liposuction anywhere…the risk of contour irregularities which may be more prone on the buttocks with aggressive fat reduction. The skin removal/tuck certainly helps mitigate to some degree that aesthetic concern.
Whether buttock reduction may be effective for you depends on what your buttocks looks like and how much fat there is at the subcutaneous level.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a slightly recessed jaw and chin. I might get jaw surgery in the future but I can’t afford it right now. I was wondering 1. Are chin implants and genioplasty the only surgeries for chin you offer? 2. Could I get a genioplasty and then get jaw surgery in the future? 3. I have just discovered chin fillers, and was wondering if they could make your chin wider or do they only increase project?
I could tell by comparing pictures and looking at other results online I would only need one syringe for a chin filler. What I am worried about is my chin looking too narrow after a filler, so I was wondering if they could increase width or do they only increase projection.
A: Thank you for your inquiry. In answer to your questions:
1) The available chin augmentation procedures include synthetic fillers, fat injections, implants and osteotomies. (sliding genioplasty)
2) A bony genioplasty deos not preclude jaw surgery in the future…although that depends on how much the chin is moved forward and how much the lower jaw needs to be moved later.
3) Injectable fillers can create any chin dimensional change…if you use enough filler volume. It is fair to say that both increased horizontal projection and chin width will likely require more than one syringe of filler.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I think I want thigh lift only whether it’s a mini thigh lift with some liposuction or full thigh lift. Please give me estimate price for both. Can’t wait to hear back from you. Thanks!
A: Thank you for your inquiry and sending your pictures. Thigh lifts in patients that look like you are very tough in my opinion in regards to the decision to trade into a scar given the amount of loose skin and skin quality that you have. Thigh lift scars in general do fairly poorly in most people because they are incisions closed under tension and are placed vertically which is perpendicular to the relaxed skin tension lines of the leg. (a recipe for poor scarring)
Like many types of extremity lifts (e.g., arm lifts, thighs lifts) the scarring does best in patients who have undergone large amounts of weight loss and the skin is very loose and stretched out. In people with much better skin quality who are not weight loss patients (you) the scarring will not be good as all. Thus I would be very cautious about considering this operation and I would certainly not dive right in. (full vertical thigh lifts) At best liposuction and a limited upper thigh lift would be the most you should consider. (and even that I cannot really endorse based on the pictures you have submitted)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I read an article you posted about ear surgery using metal inserts instead of rib grafts. Do you do this surgery? Please let me know. I am very interested in this surgery to bring my ears out about 5mm but I would rather not do a rib graft. Thank you!
A: Thank you for your inquiry. You are referring to a subtotal otoplasty reversal for over corrected ears. The key to the procedure is that the released cartilage must be held out by an interpositional piece. Initially I used a small bent metal plate. (which is the article to which you refer) That works fine but I have evolved to using tissue bank rib cartilage which I think works even better. No one wants to have their one rib harvested for the procedure.
Dr. Barry Eppley
Indianapolis, Indiana
Can A Custom Infraorbital-Malar Implant and Custom Jawline Implants Be Done During The Same Surgery?
Q: Dr. Eppley, Hi, I saw that you design Custom Infraorbital Malar Implants. It said it helps get rid of sclera show, but is this implant also part of Infraorbital rim implants?. Like does this implant also help with hollow and poor undereye support while at the same time giving the high cheekbone look?. And can this implant be inserted at the same time of a custom jawline implant?. What would be the approximate range of cost of a infraorbital malar implant+ custom jawline implant?
A: As the name implies, a custom infraorbital-malar implant provides augmentation of the infraorbital rim in both vertical and horizontal dimensions as well as can extend out onto the cheekbone and back along the zygomatic arch. This unique implant design simultaneously treats both undereye hollows as well as gives a high cheekbone look. It is common to place both custom infraorbital-malar and custom jawline implants during the same surgery. Such a combination is a well known male masculinization procedure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, One month ago I had a chin implant (submental approach) and I’m thinking of having a buccal fat pad removal procedure done. Is there any risk an infection related to the fat pad removal procedure could infect the chin implant? Basically, could an infection from the buccal fat pad removal spread to the chin implant, resulting in me having to remove the implant?
A: Thank you for your inquiry. I see no association between a buccal fat pad space infection (should that occur…but have never seen it yet) and infecting an indwelling chin implant. The buccal fat space is in a completely different anatomic tissue plane than a chin implant. Thus an infection of one can not infect the other.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a French Canadian adult and I suffer from plagiocephaly. My right side is relatively flat. The method of injecting bone cement by small incision really interests me. I wanted to know if you could help me find a specialist in Canada to perform this surgery.
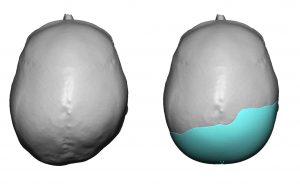 A: Thank you for your inquiry and describing your right occipital plagiocephaly concerns. While once done using bone cements placed through somewhat smaller scalp incisions, that technique has been replaced by custom made skull implants which are placed through similarly small scalp incisions. Custom implants produce far superior augmentation results that cover more of the flattened areas and assure a smooth convex surface with a very low risk of revisional surgery. (which is unlike bone cements) I can not speak for whom if anyone performs this type of skull reshaping surgery in Canada. (which I highly doubt)
A: Thank you for your inquiry and describing your right occipital plagiocephaly concerns. While once done using bone cements placed through somewhat smaller scalp incisions, that technique has been replaced by custom made skull implants which are placed through similarly small scalp incisions. Custom implants produce far superior augmentation results that cover more of the flattened areas and assure a smooth convex surface with a very low risk of revisional surgery. (which is unlike bone cements) I can not speak for whom if anyone performs this type of skull reshaping surgery in Canada. (which I highly doubt)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Glad to hear it’s something possible with iliac crest reduction and upper hip augmentation. Attached are current photos of my hip area as well as what my goal would be with the procedure. Looking forward to your thoughts.
A: Thank you for sending your pictures and the ideal goals. We understand these ideal images are the general idea which is really iliac crest/waistline reduction and upper hip augmentation. (that is bit more than just a hip dip augmentation. You appear to be correct in that the limiting factor in the lower waistline area is the iliac crest bone. Certainly the approach of aggressive liposuction of the waistline/iliac crest area to thin out the soft tissues, some iliac crest bone reduction and hip implant augmentation would be needed to try and affect some similar type of change which I have imaged. (attached)
There are two approaches to the above:
1) Do liposuction and fat transfer to the hips first and see what type of change you can affect by this standard approach. (it would be needed anyway so the effort is not lost) Then if needed the iliac crest bone reduction and hip implants can be done as stage two.
2) Do #1 with iliac crest bone reduction and hip implants.
Obviously #1 is the conservative approach (which is not always a bad thing) and #2 is the aggressive approach.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am planning of chin implant replacement and a submentoplasty procedure with you next month. I have some questions about the chin implant to be sure not will be better after the replacement as well as what changes in the neck that may occur.
A: Thank you for sending your side profile picture to which I can make the following comments:
1) If my memory is correct I have seen an MRI of current chin implant position which shows it hanging off of the end of the chin bone. Thus we know for certain that a new chin implant that is less bulky can be placed in the proper position on the bone which makes for an exclusive horizontal type of chin augmentation effect. Because of the existing chin implant and to ensure that it stays in the higher desired position, this is the role of double screw fixation of the implant.
2) Your neck is very typical for some middle-aged men who have thicker tissues creating a low hanging full neck with an indistinct cervicomental angle. While we know the best result possible comes from a full lower neck-jowl lift, most men are not prepared to go that far. (extent of surgery and ear scars) Thus the submentoplasty procedure has been chosen as it offers the most that can be achieved short of a full lower facelift. The result will not be the same but then the extent of surgery, recovery and risk factors will accordingly be lower. There is no question that the neck part will have the biggest aesthetic benefit but it is important to appreciate what the submentoplasty can and can not do.
3) I have attached an imaging prediction of what I think the likely outcome will be from these two combined procedures.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have facial asymmetry which has impacted on my self esteem for the most part of my life. I wondered if it was possible to treat and if so what procedures it may entail. I was researching v line surgery to have a more symmetrical, balanced and feminine face shape. On the pictures you can see one of my jaw bones is more square and the other more rounded. The rounded side is the side of my face that is wider. I prefer the square jaw on the side where my chin is over to.
Thank you for your time.
A: Thank you for your inquiry and sending your pictures. Your jawline asymmetry, by description and as illustrated in the pictures, has a left more square jaw angle, wider rounder right jaw angle and chin asymmetry. While a jawline reshaping procedure would be indicated, any form of traditional v line surgery would not be appropriate. I think you mentioned that approach with the intent of the result, not in how the surgery would be done. Since the one corner of your jaw is good (left square jaw angle), it is the other two corners of the jawline that need to be changed. The right jaw angle would be reduced in width by burring and a very small jaw angle implant ‘cap’ but one it to make it just more square. The chin bone would be moved to the right to put it into the midline. Before surgery a 3D CT scan of your jaw should be done to fully visualize the bony anatomy and plan the surgical changes.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m curious about a forehead implant. I am a young male and I look very young for my age, I have a round & sloped forehead and while I don’t dislike the slope I think the roundness gives me a childlike appearance. I’ve seen forehead implants that created a rounder less sloped head & i’m curious if it’s possible to create a custom implant that would create a flatter forehead. I still would prefer it to be somewhat slopped just flatter. Thanks
A: Thank you for your inquiry and describing your forehead reshaping objectives. One of the main advantages of any custom facial implant, including a custom forehead implant, is that they can be designed any way the patient wants. So having a forehead implant design that creates a flatter and less sloped forehead is certainly possible. As a general rule it is usually not a good idea to have a completely vertical forehead anyway for a variety of aesthetic reasons.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’ve ripped my tragus piercing, I think on the first or second night of getting it I must have slept on it and pulled it downwards. My piercer suggests switching the hoop to a bar but I can’t see the point if it has already been torn. I’m also concerned with how this hole will heal, whether the hole will heal itself and only be a lined scar or whether the hole will always be present.
A:I am confused between this picture and your description as to your tragus ear piercing concerns. By definition such piercings will always heal and end up as an epithelial-lined skin tract. Thus it will always be a hole through the cartilage. So a ‘lined scar’ and ‘the hole’ by your description are one and the same.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Here are some more rib removal questions after our consult from last week.. Could I get hurt physically from something injuring me in the future from wrestling etc from having rib removal? Do you think that rib removal has more or less complications than a butt augmentation? How painful is it compared to a butt augmentation? Do you think by taking the LD muscle out that it will cause better shape to my bodybuilding frame? And not take away from my lats? And not hurt my muscle when lifting? Can liposuction make my skin less tight? Is there anything that I can do during this procedure to tighten my skin in the abdomen and back region? Could removing my ribs hurt me when I am.older?
I also forgot to ask I have heard that removing the 10th rib can cause less balance coordination and exposure to the organs ect . Are my organs safe after this procedure? I apologize for all the questions
Thank you so much.
A: In answer to your rib removal questions:
1) I do not think wrestling exposes you to any increases risks of injury after rib removal surgery.
2) Rib removal has far fewer potential complications than any form of buttock augmentation, particularly that of implants. I have seen lots of complications from buttock implants but never one yet from rib removal surgery. Compared to intramuscular buttock implants rib removal surgery is less painful and with a quicker recovery.
3) Shaving of the lower outer border of the LD muscle improves the results from rib removal surgery but will not affect lifting thereafter in any way.
4) Liposuction will not make skin more loose…unless it is very loose initially.
5) There is nothing you can do to improve skin tightness after the surgery. Your skin is fairly taut and will naturally tighten on its own.
6) Removing ribs will not cause any problems as you age.
7) Removing part of the 10th rib will not cause any imbalances or expose the organs to any risk of injury afterwards.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am curious if I would be a good candidate for a chin implant or sliding genioplasty to improve my looks, especially my side profile.
I am in my early 20s, physically fit, and not at all overweight. It may be in my head, but I also feel that my side profile seems to be slightly worse from the right side. I’m not sure if you see this or might have insight as to why?
I have been insecure with my side profile for as long as I can remember, and I think I have mostly isolated the problem down to my chin. I would really appreciate your opinion on what throws my facial harmony off.
I would also appreciate if you could give any estimates for pricing of possible procedures. I am a college student, but this issue destroys my self esteem so I am willing to finance within reason. I do not want to go with a subpar surgeon and have done a fair amount of research and am really impressed with your work.
Thank you.
A: Thank you for your inquiry and sending your pictures. I have attached an image prediction from the side view which demonstrates the type of change that would occur in about the 8 to 10mm range of chin augmentation. Both a chin implant and a siding genioplasty can achieve the identical side profile changes. The differences between them lies in the changes they make from the front view (an implant can make it wider or more square whereas a sliding genioplasty either keeps it the same width or makes it slightly more narrow, the cost between the two and how one feels about an implant or whether one prefers moving their own bone.
The reason your side profile looks different between the two sides is that you have natural chin asymmetry which can be seen in the front view. (the right side is a bit more pronounced than the left side)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have been researching a whole lot online and I can not find anything on “midface shortening” procedures. I have a very long midface (pupils to beginning of vermilion border) that is really bothering me. Is there anything that can be done to significantly shorten it or am I just forced to have to live with it? My nose is long and my philtrum area is around 15mm long. Can rhino/lip lift decrease the length of my midface by at least 10mm or is that just impossible and if so than why?
Thank you in advance😊
A:Unlike the upper and lower facial thirds, the middle of the face can not undergo any substantial length shortening. It does not matter what you do to the bone the overlying soft tissues are not going to shorten. You have mentioned the only two procedures that can be helpful to create some appearance of midface shortening. (subnasal lip lift and tip rotational rhinoplasty) Whether that wouold be effective in your case would require computer imaging to determine.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m interested in Medpor implant removal. I’ve heard many horror stories about Medpor removals, such as nerve injury. But my understanding is that Medpor implant is placed under the periosteum — shouldn’t this separate the nerve/muscle and the implant. Or is that because they are adherent, so it requires a careful dissection to avoid tearing the nerve ending?
I was wondering if this “traumatic” removal will hurt the soft tissue, which leads to any functional problem or any indentation.
Also, many surgeons state that revision surgery is much harder because of more scar tissue and its contracture. It’s definitely harder for a nose job, but how about chin surgery? Will scar removal + fat grafting helps the revision surgery?
Thanks, and I’m looking forward to your reply.
A:cOn a comparative basis to solid silicone (which is the unspoken point of reference) Medpor implant removal is considerably more difficult and has some higher risks due to its robust tissue adherence. But that being said I have removed hundreds of Medpor implants and have not seen any adverse problems such as nerve injury or significant soft tissue issues. You do have to be careful, as you have alluded to, that the chin implant wing may be close to the mental nerve. The more relevant issue, like any chin implant removal regardless of its material, what is going to happen to the expanded overly soft tissues once the underlying implant support is removed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello. I wanted to make some enquiries about a chin reduction/jaw reshaping. I am very self conscious about my long face and asymmetry. Im aware I have a class 3 malocclusion which has been ‘camouflaged’ by braces so im not interested in any orthognantic surgery but more so a shaving/cutting of the jaw and chin to shorten and improve specifically the lower third of my face if possible.
My main concern about a chin reduction is the lack of support for the soft tissue and drooping. I also feel like there is a significant submental fat pad on the chin which is even more obvious when I smile. I would like to retain a petite tapering to my chin (I definitely do not want my face to look round).
I would be happy to arrange a virtual consultation. I have attached 6 photos.
A: Thank you for your inquiry and sending all of your pictures. You have correctly surmised one of the two limiting factors in chin reduction surgery: 1) what will happen to the soft overlying soft tissue as it will only shrink so much (very similar to a rhinoplasty with thick skin…what the skin does is control how small/refined the nose can become, and 2) the location of the interior alveolar nerve and tooth roots in the bone which will control how much bone can be reduced. Thus every chin reduction must take into consideration both of these issues. In that regard using your own diagram I have shown the different between a realistic vs a non-realistic goal. I will have my assistant Camille contact you arrange a virtual consultation time to discuss further.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I came across your website and found some of the results of occipital bone reduction surgeries (I could not find a case similar to mine though). As you could see in the attached picture, I have this protrusion that spans all the back of my head up to my neck. I would like to hear from you what could be done to fix it, in as much detail as possible.
From my search on your website, it seems that the solution is through bone burring of a maximum of 6 mm only at the spot of the maximum protrusion. It seems in my case that this will not make a big difference as there will still be some protrusion. Right?
A: Thank you for your inquiry and sending your picture. What you have is an enlarged nuchal ridge line which is the bottom of the exposed occipital skull bone. Most people do not realize how high the back of the skull is which corresponds to the same level as the brow bones in the front. (which is the bottom of the skull in the front) The bottom of the occipital skull (nuchal ridge) is the thickest part of the entire skull so much more bone can be removed here than in other skull areas. (10mms or more) Which would produce a noticeable and likely worthwhile result as I have shown in the illustrated attachment.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi, I wish to one day undergo this procedure to correct my skull shape, mainly my flat back of the head. However, I would also like work on temporal, sagittal, and frontal (all 4 options in total). My main question was since I couldn’t find anything on your website about all 4 procedures being done at the same thing; is this even possible and if it is, how would it be done? Separate or altogether? Thank you and have a good day.
A: It is not uncommon to work on multiple areas of the skull at the same time, whether this be for augmentative or reductive changes. The limiting factors of multisurface skull reshaping is the location and length of the scalp incisions needed to do it and how much the scar can be stretched at any one time in augmentations.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a consultation on earlobe reshaping/revision. I was born with a tag on my left ear and it was removed when I was an infant. As I have gotten older and lost my hair, it bothers me more now because there is no symmetry. Attached are some photos of both ears. I can come any time for an in-office consultation. I appreciate your looking at my photos and giving me your advice.
A: Thank you for your inquiry and sending your picture. I think the best way to make the left earlobe look better and more symmetric is to do a wedge resection of the deformed/scarred part of the left earlobe.That would create a better earlobe shape. It may make it a bit vertically shorter than the right side but the earlobe would have a smoother appearance.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am four months post infraorbital rim/malar implants removal, and my cheeks still feels a bit bloated. I assume swelling may be a big factor, but I feel that is an appreciable capsule that is causing fullness and an imprint of the implant. Here are my questions:
1. Will the capsule go away on its own, and if so, about how long does that take?
2. Can steroid injections be used to dissolve the capsule (whether or not it’ll go away in its own)?
3. Are steroid injections safe? I’ve been told they can cause atrophy. It seems some doctors will inject into scar tissue but soft tissue swelling. Do you agree with that assessment?
4. Is scar tissue and the capsule the same exact thing?
A: In answer to your post infraornital-malar implant removal questions:
1) Capsules can take 12 to 18 months to fully resorb.
2) Steroid injections are not a known effective treatment for capsular resorption.
3) Like all medications, steroid injections have well known side effects which primarily include soft tissue atrophy and contour deformities as a result.
4) A capsule is an organized layer of scar tissue to any implant that has a very distinct collagen formation and four layers of such collagen formation to it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, I had a Lefort 1 surgery done a month ago which left me with fuller cheeks. I want to get my slimmer face back and was wondering what could be done. Hopefully I would be able to achieve my former look. I could attach before pictures if you would like. Thank you have a nice day.
A: Thank you for you inquiry and sending your pictures. A LeFort 1 osteotomy, by definition, moves the lower base of the upper jaw forward, meaning there are certain fascial changes that will occur to the bone right above the teeth roots. (base of nose moves forward, tip of nose may rotate more upward and fullness will appear in the lower cheeks) How significant these facial changes are depends on the amount of forward movement one has. I don’t know your degree of maxillary movement but t hat issue aside I can make the following comments:
1) It takes a minimum of 3 or 4 months until all of the facial swelling subsides AND the overlying soft tissues shrink back down around the reshaped bone. You will know more by then how whether what you are seeing now resolves or merits surgical improvement.
2) The surgical improvement would be to remove the plates and screws and contour down the bony step off located in the under the cheekbone area which is where you see the new fullness.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had an ear reconstruction. My last surgery was done six months ago. I would like a revision to make it look better. Please let me know if you can help with protruding, rim, hair removal.
A: Thank you for your inquiry and sending your pictures. I assume you had a traumatic injury and the soft tissue part of the ear reconstruction was done using a rotation scalp flap, which is why there is hair on the back of the ear. Th thickness of the folded rotation flap makes the helical rim very thick. (protruding rim) That could be improved by removing the skin from the flap from the rim all the way down to the postauricular sulcus and replacing it with a split-thickness skin graft. That should thin out the rim as well as get rid of 100% of the hair on the back of the ear.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, What type of jawline reduction do I need? In my prior facial feminization surgery they did jaw reduction but the inmprovement is not enough to really make my jaw area less masculine.
A: Good meeting and talking you this past weekend. As per our discussion I have attached some imaging looking at what I envision for your jawline reduction/reshaping. Your excessive jaw size is really in the anterior 2/3s of the jaw, particularly having had prior jaw angle width reduction. I would hate to amputate your jaw angles off in the traditional v line surgery approach as, while that creates the most dramatic jaw reduction effect, it also can create loose tissues over the angles/neck as well as gives a high jaw angle look which for Caucasian women today is not the desired jawline look they seek. Thus I would consider a modified approach using a t-shaped genioplasty with vertical and midline wedge resections as well as inferior border removals back to but not including the jaw angle bone. I would need to evaluate a lateral cephalometric and panorex x-rays to make measurements as to the feasibility of these two intraoperative jaw reshaping techniques.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I asked this question because I have had intraoral incision before for the Medpor chin implant. The intraoral scar looks no good.
I was wondering if it’s possible to remove the implant and use sliding genioplasty after it completely healed? Will the intra oral incision again makes the scar worse? I heard some people described its like glue in the mouth…
Thanks!
A: In answer to your questions about sliding genioplasty:
1) Generally the intraoral incision would not look worse. But that statement is said on a general basis as I have no idea what your intraoral scar looks like. Suffice it to say it would probably not look better but slash probably not worse.
2) While you can certainly stage the implant and the sliding genioplasty it would make more sense to put the two together since chin implant removal provides all the access for the sliding genioplasty.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a general question for you regarding PMMA for skull reshaping. Does PMMA last a lifetime? Are there ever cases where there are infections or consequences years later?
A: PMMA material will last a lifetime as it can never degrade or breakdown. I have never seen any long-term medical consequences with its use in 30 years such as delayed infections or any other adverse soft tissue responses.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I think that the most prominent issue is the lower eye however I think that the right cheek is also “flatter” because the right malar bone is not as prominent or is smaller or “set back”. I also think that the hypoplastic bone structure extends to the top right of the skull. For instance, the top right of my forehead doesn’t match the top left.
The point about a flatter cheek on one side wouldn’t show as much I think from a front on photo.
So I think skull reshaping may also be required in addition to any work on the face.
In terms of the question about what was done previously. This was cheek and brow augmentation I think using a bone cement called hydroxyapatite. I was operated on by two surgeons during one operation. One doing the bone augmentation, the second an eye surgeon specialist did left and right blepharoplasties and a right canthal suspension to raise the canthus of the right eye higher up the face.
There was a fat prolapse under the eyes and this also contributed to the appearance of asymmetry.
The brow and cheek augmentation was the cheaper of two treatment options presented to me and was the only one I could afford at the time. The second, more expensive option would have required the production of a custom “implant” that would have augmented the hypoplastic bone more generally in the face and skull.
Obviously I am only a layman but I think with the approach that I opted for the results cannot be guaranteed and of course only augmented the cheek and brow bone in an attempt to reduce the appearance of the asymmetry as opposed to generally correcting it.
The other approach with the “implant” (I’m not sure that is an accurate word for it) designed based upon analysis of scans of the skull would have fixed the issue more generally and I think the results of how it would change the bones near the eye are probably more accurately predictable.
A: Thank you for your detailed response. Your biggest component of your facial asymmetry has always been your VOD. (vertical orbital dysopia) which affects more than just the position of the eyeball. With a lower orbital box the brow bone/forehead/skull is pulled down and the cheek is flatter that side. That is all consistent with the VOD.
Your are correct in that your original facial asymmetry surgery was a patchwork approach to the problem, which helped, but predictably left it uncorrected as the solution did not ideally match the problem. You are also correct in that using a 3D CT scan the fuller extent of the bony problem can be addressed to provide the supportive foundation. Your prior lateral canthoplasty is a good example of just pulling up the soft tissues without underlying bone support results in less than optimal result and one that is not well maintained.
Dr. Barry Eppley
Indianapolis, Indiana