Your Questions
Your Questions
Q: Dr. Eppley, I have a chin implant questions/issue. In my opinion, I have a recessed chin and jaw. Eight years ago, I had a large silicone chin implant inserted, and liposuction below my chin. At my consultation, the plastic surgeon asked if I breathed through my mouth, which I realized I do. Ever since then, I have been on a quest to resolve this issue. I have been to an ENT doctor who said my nasal passages checked out fine. But since I feel that my chin implant did not provide me with enough projection (I am 41 years old but one year ago I had a platysmaplasty for loose skin beneath my chin), and my lips still do not close with out mentalis strain, and as I age I feel that my lack of a supportive jaw is not helping, I would really like to take action. Also, I recently discovered that chin implants have been known to cause bone erosion, which frightens me. I had braces as a teenager, and still have a bit of an overbite, but I do not know where that leaves me as far as options to both improve my appearance and breathing functions. I sincerely appreciate your time and thoughtfulness, as this is quite daunting to me.
 A: The chin implant issue that you describe is a common one that I hear about. Between your appearance and breathing issues, your description suggests that your lower face/jawline appearance can be improved. With a naturally short lower jaw, a large chin implant that is still inadequate in projection and a residual mentalis strain, this indicates to me that you need a sliding genioplasty for a chin implant replacement. Besides the limitation of chin implant projection (10mms or less), increasing the chin point by an implant will not improve mentalis muscular function nor any lower lip incompetence should it exist. Your existing chin implant may have also developed some settling into the bone. (often erroneously referred to as ‘bone erosion’ which is not harmful) By removing your chin implant and performing a sliding genioplasty you will improve your chin projection, eliminate the mentalis strain, and also improve your neck profile. I would need to see some pictures of your face to verify these statements but your description is not a rare problem that I see with indwelling large chin implants.
A: The chin implant issue that you describe is a common one that I hear about. Between your appearance and breathing issues, your description suggests that your lower face/jawline appearance can be improved. With a naturally short lower jaw, a large chin implant that is still inadequate in projection and a residual mentalis strain, this indicates to me that you need a sliding genioplasty for a chin implant replacement. Besides the limitation of chin implant projection (10mms or less), increasing the chin point by an implant will not improve mentalis muscular function nor any lower lip incompetence should it exist. Your existing chin implant may have also developed some settling into the bone. (often erroneously referred to as ‘bone erosion’ which is not harmful) By removing your chin implant and performing a sliding genioplasty you will improve your chin projection, eliminate the mentalis strain, and also improve your neck profile. I would need to see some pictures of your face to verify these statements but your description is not a rare problem that I see with indwelling large chin implants.
As for your breathing issues, nothing you do to the chin will have any impact on your nasal airway exchange.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in facial reshaping/liposuction for my son. For several years my 16 year old son has expressed concerns with excess fat in the cheek/chin/neck area. He has a genetic double chin that upon weight loss did not help and did not go away. In tears, my son asked if he could do what I did (lower face lift/liposuction) While I do not feel it would be necessary for him to go as extreme, I told him I would research his options. In my own experience, I know it’s not something that diet and exercise alone can help with. As a parent though I am conflicted regarding the risks/ psychology etc. of a surgery for cosmetic purposes at his age. Thank you in advance for your help and information!
A: When it comes to facial reshaping via fat removal, there are several specific areas in the face where fat extraction can be very helpful. This includes the neck (liposuction), buccal fat pad (buccal lipectomy) and the perioral mounds. (liposuction) All three areas would be of benefit to your son based on his pictures. That may not necessarily completely deround is face or give him a thin face but would make a substantative improvement.
When it comes to plastic surgery in teens, the major consideration is their level of expectations. Being less mature and often being guided by information that they find on the internet, their sense of realistic expectations and the necessary recovery process until they truly see the final results is often not accurate. But from a physical standpoint, there is no greater risk of these facial procedures in a teen ager than in an older adult.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in scar revision of my wide midline abdominal scar from a prior surgery. One surgeon I saw recommended a geometric broken line closure (GBLC) type of scar revision. You have recommended a more simpler vertical excision and straight line closure. My question is why would you choose that particular procedure over the GBLC if the broken line procedure yields better results?
A: There is no guarantee that a broken line closure will produce a better result on a midline abdominal scar and there is no medical evidence to support that it will. And if the scar should widen to any degree, you will have more scar length than what you started with. Whomever advised you that a GBLC for your midline abdominal scar (that has never had a revision before) was the right choice for scar revision is simply wrong. That is simply not done on many body scars. It is most commonly done on facial scars which are a completely different in how they heal than any scar below the neck. You should initially do the simplest and least risky scar revision technique first and then proceed to more complex forms should that not produce a substantial improvement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to get a tummy tuck and belly button reconstruction. I’m not sure what type I need. I workout approximately 5 days a week. I have a lot of scar tissue near my c-section scar that is bothersome. Would a procedure also help with the scars? What type do you recommend?
 A: You are correct in your assessment that you would benefit by a tummy tuck. When it comes to tummy tucks there are really only two fundamental types; a mini- or limited and a full tummy tuck. The difference between the two is in the the location and amount of abdominal tissues removed. With uncommon exception, most women are better off with a full tummy tuck because it produces a better result, remakes the belly button and provides the best exposure for complete rectus muscle plication. As part of the tummy tuck, all scar tissue from the previous c-section(s) would be removed regardless of whether one gets a mini- or full version.
A: You are correct in your assessment that you would benefit by a tummy tuck. When it comes to tummy tucks there are really only two fundamental types; a mini- or limited and a full tummy tuck. The difference between the two is in the the location and amount of abdominal tissues removed. With uncommon exception, most women are better off with a full tummy tuck because it produces a better result, remakes the belly button and provides the best exposure for complete rectus muscle plication. As part of the tummy tuck, all scar tissue from the previous c-section(s) would be removed regardless of whether one gets a mini- or full version.
Be aware that many tummy tucks also incorporate liposuction as part of it to get a better overall result.. That could be liposuction of the flanks beyond the zone of the tissue excision or above the zone of tissue excision in the upper abdominal area.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in abdominal scar revision. I’m a 22 year old female who had a major surgery resulting from a self inflicted wound that occurred in a more troubled time as a youth. I still have the ugly scar and started research on my z-plasty scar revision for two years now. I’d love to do a consult with you. I’m turning 23 this year and would love to be in my first two piece. I have attached a photo of “my struggle”. Hope to hear from you soon.
A: When it comes to your abdominal scar revision, I see no reason why you would ever have a z-plasty type revision. Your scar revision would be a straight linear scar revision in which the scar is simple vertically excisioned and then closed in a linear fashion. This is the only type of scar revision you should ever have. While it will not make the scar go completely away, it will make it much more narrow.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have been diagnosed with a mild midface deficiency. I would like to have this corrected to end up with the most aesthetic appearance possible. I have been reading about facial implants and the work you have done with them. I would like to achieve a reduction of the depressions on either side of the nose, reduction of the heavy creases going down to the corners of my mouth and better projections of my face to make it look less wide and flat. In addition I am also interested in lip implants. I already have some lip implants placed. They were the type that look like spaghetti and the size was 4mm top and bottom. I would like to add to these to make my lips bigger. Specifically I would like to show more of the pink lipstick area rather than just make them stick out more. I would also like to bring the implants out to the edges of my mouth to make the lips and mouth appear wider.
A: When it comes to facial implants, there are a lot of facial changes that they can make…and there some changes that they can not. For a mild midface deficiency, consideration can be given to paranasal implants to bring out the base of the nose and anterior submalar implants to provide some upper midface projection. The lower nasolabial folds as they approach the corners of the mouth will not be affected by any bone-based implant. This area is best treated by fat injections.
In regards to the lips, you either have more recent Permalip silicone implants or older style Advanta lip implants. Either way it is not a good idea to double stack lip implants as there will be a great tendencey to have them roll or twist on one another. You may exchange them for the largest 5mm implants but, for the sake of a 1mm increase, that is not likely to make much of a difference. Furthermore, some of the lip changes you desire can not be achieved by lip implants. No implant will increase the vertical height of the vermilion (pink lipstick area) nor will they make the corners of the lip appear fuller or wider, they are too thin in this area. To make these kind of lip changes, you will need to consider a vermilion or lip advancement procedure which directly changes the location of the vermilion…which is what is needed to make the type of lip changes you desire.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in skull reshaping reduction of the size of the back of my head. For a long time, I have had a distressing issue with the prominence of the back of my head in what I believe to be the occipital bone region. The problem is primarily located slightly right of centre of the back of my head. In other words, from side view, my head sticks out more on the right side than it does on the left and the bone can visibly be felt as thicker and more protruding. It also doesn’t help that my crown area feels very flat and almost leads into a boat shape back of the head. After much research, I do not necessarily believe that I have a form of craniosynostosis, though I am not ruling out the possibility of perhaps a mild manifestation of it.
As a young 25 year-old man, are there options out there for me to possibly reduce the ‘sticking out’ of the back of my head, so that I can have a more ‘normal’, flatter back of the head? I have attached two photos, taken from either side of my head, so that you can notice how one side sticks out more than the other (though my occipital bone in general sticks out much more than normal). I also appreciate that it may be hard to tell by the photos because of my hair coverage, which I keep as an attempt to mask the bumps. I understand that things of this nature are usually dealt with more in children but I came across your site when researching possibilities for occipital reduction.
A: Skull reshaping of the prominent back of the head is very common in my practice. It is never a question of whether occipital bone reduction can be done, it is always a question of whether the reduction achieved will be significant enough to justify the effort. As a general rule, 5 to 7mms of occipital bone can be reduced. That may not sound like much but usually produces a noticeable size reduction. Just based on your description of the problem, it sounds like this amount of reduction would be adequate to make a difference in your back of the head shape.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had fat grafting to my face and I love it. I am three weeks out and I have noticed already that some of the fullness has started to go down. I would prefer it to stay this way and I don’t want it to go down. How much of the fat will stay and how will I know when the result is finally stable? I don’t think my doctor overfilled at all. And the first two weeks I looked amazing, but things have changed over the past week and it is not nearly as full now as it once was. 🙁
A: Fat grafting is a wonderful technique for a variety of facial enhancement issues but it plagued by unpredictability of fat graft survival. A good guideline for the amount of volume retention after fat grafting is to wait at least until 6 weeks after the procedure. Generally the success of most fat grafting results is seen by then by ultimately a final judgment should not be done until 3 months after the procedure. That is also the time when fat grafting can be repeated if necessary. At just three weeks after the procedure you will very likely lose more fat, it is just a question of how much more over what period of time.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a subnasal lip lift. I have a long upper lip and I think it would make my face more balanced and attractive. I have not read anywhere on how one determines the amount of skin that can be removed between the lip and the cupid’s bow. I want the maximum to be removed but I still want it to look natural and not be overdone. I want to increase the size of my upper to the maximum as it is basically non-existent now. Also, will the subnasal lip lift increase the size of the whole upper lip and not just the cupid’s bow directly underneath the nose? Thank you.
A: In a subnasal lip lift, you do not want to remove more than 1/4 to 1/3 of vertical distance as measured along the philtral columns. Whether that is 6 or 8mms is a judgment between aggressiveness but also wanting to avoid an unnatural and potentially irreversible overdone result. Applying the principle that it is easier to remove more later but you can’t reverse it, I would take no more than 6 to 6.5mms of skin. Also a subnasal lip lift will not change the amount of exposed vermilion out to the mouth corners, it will only change the upper in teh middle third or within or under the nose area.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in learning about suprapubic liposuction. I’ve been searching for answers for my 8 year old son for 8 years. He has a buried penis. He has had two surgeries already when he was 2, which rearranged the skin on his penis to have it appear normal looking, however nothing was done with the suprapubic fat pad. It took me two years to finally get someone to acknowledge that there was actually a problem with my son’s penis. He was a stalky baby weighing nearly 9lbs, and I was told he would lose the mound when he grew and was a toddler. He didn’t, he’s still a stalky child, very active but never loses the mound. His penis is totally hidden, but can be exposed if he pushes the fat pad down around it. He is active in hockey and baseball and is getting to the age where it needs to be addressed before he starts getting ridiculed by his peers. I would really y appreciate any information you could give me regarding this procedure.
A: Suprapubic liposuction can very helpful in children and adults with a buried penis problem. The suprapubic mound is a common companion of the buried penis problem. It is not fat that is responsive to weight loss nor will it go away as one gets older. Suprapubic mound liposuction can be very effective at reducing the mound and helping get some more penile exposure. There is a limit as to how much penile exposure will occur but the fat mound can be significantly reduced. Suprapubic mound liposuction is a simple outpatient procedure that uses small cannulas to extract the fat through two small groin incisions. (4mms) The recovery is very short although it takes several months for all the swelling and firmness to dissipate from the base of the penis.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in ear reconstruction. I lost my right ear several years ago in a car accident. I have attached a couple of pictures so you can see the extent of the ear loss. How can my ear be fixed?
 A: A complete ear avulsion represents the most complex type of ear reconstruction. The obvious injury seen in the pictures you sent is a traumatic avulsion of the complete external ear. In dealing with such ear injuries, there are two methods of reconstruction which are dramatically different. The first method is known as the autologous or natural tissue reconstruction method using the patient’s own tissues. The framework of an ear can be fabricated from one’s own cartilage since the ear (minus the earlobe) is cartilage covered by skin. To create the necessary skin, an initial tissue expander must be placed to stretch out (expand) the skin around the ear hole. (external auditory meatus) Once enough skin is created, the tissue expander can be replaced with an ear framework fabricated and carved out of rib cartilage. Somke minor touchups are needed later to make the earlobe and a crease or sulcus on the back of the ear. The other approach is to make a prosthetic ear which is held into placed by end osseous (dental) implants. Three implants are initially placed around the ear hole and allowed to heal. They are eventually uncovered and then used as magnetic retention posts onto which a prosthetic ear can be attached.
A: A complete ear avulsion represents the most complex type of ear reconstruction. The obvious injury seen in the pictures you sent is a traumatic avulsion of the complete external ear. In dealing with such ear injuries, there are two methods of reconstruction which are dramatically different. The first method is known as the autologous or natural tissue reconstruction method using the patient’s own tissues. The framework of an ear can be fabricated from one’s own cartilage since the ear (minus the earlobe) is cartilage covered by skin. To create the necessary skin, an initial tissue expander must be placed to stretch out (expand) the skin around the ear hole. (external auditory meatus) Once enough skin is created, the tissue expander can be replaced with an ear framework fabricated and carved out of rib cartilage. Somke minor touchups are needed later to make the earlobe and a crease or sulcus on the back of the ear. The other approach is to make a prosthetic ear which is held into placed by end osseous (dental) implants. Three implants are initially placed around the ear hole and allowed to heal. They are eventually uncovered and then used as magnetic retention posts onto which a prosthetic ear can be attached.
There are advantages and disadvantages with either approach. (autologous = multiple reconstructive surgeries, prosthetic = need to continuously remake new ear prostheses)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I recently read your blog about malar and submalar implants. I just have one question since there doesn’t seem to be much information on these implants, but where exactly are the malar and submalar regions?
If I’m looking at implants to provide a swoop from the nose to the cheeks (sorry, not sure how to describe it, but think of Bradley Cooper’s midface), which implant would actually provide that kind of volumetric augmentation?
 A: The difference between malar and submalar implants is subtle but very different. As shown in the attached drawings on a person’s face, the malar region is the cheek bone itself while the submalar region is actually below that off of the bone.
A: The difference between malar and submalar implants is subtle but very different. As shown in the attached drawings on a person’s face, the malar region is the cheek bone itself while the submalar region is actually below that off of the bone.
There is no preformed or standard shaped implant that provides fullness (a swope) from the nose to the cheek because directly in its path is the large infraorbital nerve. An implant can be fashioned with notching of the nerve to avoid compression (maxillomalar implant) of the nerve using either a 3D model of the patient or pre making it off of a basic skull shape.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I understand that malar and sub-malar facial implants can be used to add volume, 3-dimension and contour to the face. Initially the imaging you provided showed the malar implants only, I think? I am interested to know if the sub-malar implants can be added as well, and more laterally, to camoflauge the slighly hollow buccal area of my face.
Can you please also explain to me the use of paranasal implants? I understand these are largely popular in Asia.
In your opinion, would they assist in the roundening and softening of my face as a whole?
You mentioned the chin augmentation I did may have produced an extreme result, compared to what is actually achievable? Do you think I would notice a measurable reduction in both the width and length of my chin with the sliding genioplasty?
A: What I previously showed was the use of malar implants in your face. The combination of malar and submalar implants is known as malar shells. That would extend the fullness into the underlying buccal space right below the prominence of the cheek bone.
Paranasal implants are designed to add fullness to the base of the nose or push it out further. They are common in Asians because they naturally have a flatter mid face throughout. I can not tell if they would be of benefit to you without looking at picture of your face from different angles, like the side view and the three-quarter or oblique. Midface augmentation in general requires a more 3D type assessment not just a flat 2D picture from the front view.
As for our chin reduction/narrowing, what you had demonstrated was a bit too sharp and extreme which is not surgically possible. But an osseous genioplasty (not a sliding one) can reduce the height of the chin as well as make it more narrow through vertical and midline bone removal.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have always had a long upper lift, and a downturned mouth, causing people to think I’m sad or annoyed, when I’m simply feeling neutral. As I have aged (over 40 now), the downturn has become more pronounced, and in the last year, I’ve started to have problems with the seal in the corner of my mouth being imperfect–leading to drooling at night, and occasional infections in the corner of my mouth. I am interested in a corner of the mouth lift–but am not concerned about the asymmetry in my vermillion, or the longer top lip–just the corners. I have a fabulous smile, and would hate to have anything change it!
I am also a very “moley” person–with new moles popping up every year…and have at least one, almost pencil eraser sized one that I would like removed–and possibly a cluster of four, on the other side of my face, as well. I’m looking for your opinion as to the advisability of the mole removals (potential scarring), as well as a corner of the mouth lift. I am also working on losing weight–have lost 50 pounds so far, and have about 70 to go…I had originally wanted to wait until I lost all the weight until I did anything about this…but the mouth infections are making me push this forward a bit–do you think that additional weight loss would be a concern, in having this done sooner, rather than later?
I’m attaching two images–including all the moles–with the second one approximating the neutral/barely upturned mouth corners I’m hoping for–and with the moles removed.
Thank you for any help you can provide!
A: By your pictures and the imaged changes you have shown, that type of result from a corner of mouth lift is very realistic. I have usually found that the corner of mouth lift can improve or eliminate the yeast infections from the salivary wetness. Your weight, loss or not, has no bearing on the corner of the mouth lift procedure. (in other words there is no benefit to doing it after weight loss)
All of the facial moles you have can be removed with minimal scarring. Given their raised non-melanotic appearance, I would not routinuely send them for pathologic evaluation as nothing about them makes them suspicious for any form of skin cancer.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in scalp scar revision. I had hair transplantation done twenty years ago. However I now shave my head but the recipient area at the front is knobbly and raised where the last line of plugs were placed which is my main concern. There is also a scar running along the top middle of my head an initial scalp reduction which is my second concern and lastly scars on the back of head (donor site) which is much more of a minor concern. So my first priority is to flatten and smooth the recipient area at the front then depending on costs try to break up the linear scar that runs up the middle of my scalp. The donor scars at the back aren’t too much of an issue to me at moment. Do I have to have the old plugs removed (don’t really want to go thru another round of surgery again if it’s at all avoidable) or could I fix this up with dermabrasion/laser/kenalog injection s etc. I would appreciate some advice.
A: When it comes to scar revision of previous hair transplantation recipient sites, there are really fairly limited options. The knobbly appearance is certainly not going to be improved by excising the plugs, that will likely make it worse. There is a substantial surface contour difference between the implanted sites and the native scalp that is not likely to be ever improved by any type of skin resurfacing. Like the face with deep acne scars, laser resurfacing would be a disappointing experience. Dermabrasion may be more effective but at the risk of inducing pigmentation changes. The only procedure that I would remotely consider would be fractional laser resurfacing, as it would be safe, but I doubt particularly effective. The linear scalp reduction may be capable of being improved in appearance by replacing it with a running w-plasty type of scar revision.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a woman who is interested in umbilicoplasty. I have attached one photo which is similar to how my bellybutton looks. I am not certain if it is a hernia as I have had this my entire life. I am wondering how if an umbilicoplasty procedure could successfully change my outie bellybutton into an innie bellybutton, even if it is not a hernia.
 A: The umbilicoplasty procedure involves a variety of small procedure to reshape the belly button or umbilicus. It can be done t change an outie to an innie as you desire or to remake an umbilicus lost from prior surgeries. An outie belly button may or may not represent an actual hernia. If you stick your finger and push the outie in…and feel an inner ring or hole and the outie pushes into an innie…then it is a hernia. If you push on it and the outie simply gets flattened but does not push in, then it is not a hernia, it is just a ‘button of skin’ so to speak. It is not possible to answer that question by just looking at your picture but I suspect, given your young age and perhaps not having children (??) that your outie is not a true hernia. Eitehr way, an umbilicoplasty can convert an outie into an innie whether it is a hernia or not, just some slightly different techniques are used to do it. An umbilicoplasty can be done under just local and, at the most, some IV sedation as a simple outpatient procedure. There is no real recovery from it.
A: The umbilicoplasty procedure involves a variety of small procedure to reshape the belly button or umbilicus. It can be done t change an outie to an innie as you desire or to remake an umbilicus lost from prior surgeries. An outie belly button may or may not represent an actual hernia. If you stick your finger and push the outie in…and feel an inner ring or hole and the outie pushes into an innie…then it is a hernia. If you push on it and the outie simply gets flattened but does not push in, then it is not a hernia, it is just a ‘button of skin’ so to speak. It is not possible to answer that question by just looking at your picture but I suspect, given your young age and perhaps not having children (??) that your outie is not a true hernia. Eitehr way, an umbilicoplasty can convert an outie into an innie whether it is a hernia or not, just some slightly different techniques are used to do it. An umbilicoplasty can be done under just local and, at the most, some IV sedation as a simple outpatient procedure. There is no real recovery from it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in breast augmentation surgery and am having trouble deciding between saline vs silicone implants. I know there are numerous differences between them but one specific question I have is about capsular contracture. Does silicone implants lead to a higher rate of capsular contracture problems than saline implants?
A: One of the risks of breast augmentation surgery is capsular contracture. Capsular contracture is the result of excessive scar tissue forming around the implant. Then like a shrink wrap, it tightens around the implant causing it to feel more firm and can also distort the shape and position of the implant.
Historically silicone gel implants were associated with a higher rate of capsular contracture problems. This occurred because the implant allowed for some of the gel material to get through and out into the breast tissue (gel bleed) leading to the soft tissue reaction known as capsular contracture. In addition there was a moderately high rate of silicone implant rupture which exposed a lot of the gel material to the breast tissues. By comparison, today’s newer silicone gel implants do not have any significant gel bleed and a much lower rate of implant rupture. (less than 1% in the first five years for one manufacturer) Thus, silicone gel breast implants of 2014 are much improved designs over those used in 1989 with a much lower rate of capsular contracture.
The other issue that has led to a dramatic drop in capsular contracture problems over the past two decades has been the change in implant position. Today the vast majority of breast implants are placed in a partial submuscular (dual plane) position. Decades ago it was far more common for implants to be placed above the muscle (subglandular) position. Submuscular breast implants have a known lower risk of capsular contracture rate.
While the risk of capsular contracture always exist with any type of breast implant, it is a very low risk today with the use of either silicone gel or saline implants placed in either a total submuscular or dual plane pocket position.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had liposuction recently on numerous areas of my body including my stomach, love handles, and thighs. My doctor told me he removed two and a half liters but couldn’t tell me exactly how much it weighed. He showed me a picture of a bag that contained the fat removed, which looked like a lot, but he said he didn’t weigh it. can you tell how much you think it weighed?
 A: A question that I often receive from my Indianapolis liposuction patients is “how much does fat weight after removal?” While plastic surgeons remove and record the volume of fat in liters, this often has little meaning to most patients.
A: A question that I often receive from my Indianapolis liposuction patients is “how much does fat weight after removal?” While plastic surgeons remove and record the volume of fat in liters, this often has little meaning to most patients.
In calculating liposuction weights, one has to start with knowing that 1 US gallon equals close to 3.8 liters. While a gallon of water weighs about 8.4 lbs, fat however will weigh less because it is less dense. A gallon of fat is known to weigh about 7.4lbs. The density of fat is 0.9 grams/ml or 1000ml (1 liter) or a weight of 0.9 kg. Taking these calculations, one liter of fat equals roughly 2 lbs. Therefore 2.5 liters of liposuctioned fat will weigh close to 5 lbs.
While one liter of pure fat weighs about 2 lbs, it is actually less straightforward than that when it comes to fat removed by liposuction. What is removed in liposuction is called the aspirate and not just pure fat. Liposuction aspirate is a mixture of solid pieces of fat, free fatty acids (broken fat cell contents or oil) blood and tumescent solution. (what was injected into the area before liposuction) Thus, liposuction aspirate is not 100% fat but just a fraction of it. (a big fraction just not 100%) As a result, one liter of liposuction is really less than 2 lbs of fat removed and may be realistically closer to 1.5 lbs of actual fat. However when you factor in the number of fat cells that have remained behind inside the patient that have been damaged or destroyed and will be lost as the tissues heals, it is still fair to round up the total fat ‘removed’ to 2 lbs/liter.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I want to know if my breast implant got ruptured. I got in a car accident last week. My car was from the side and the air bag was deployed, striking my right breast with considerable force. Although both cars were badly damaged, no one was injured. The only injury I got was a big right breast bruise and pain. I still have pain and numbness on the right side of breast as well as the bruising. Is there any chance that my breast implant ruptured? I had silicone gel breast implants placed five years ago. I am worried about tearing my implant bag. There is no sign of any difference in size between the breasts and the pain is slowly becoming less. Do you think my breast implant is ruptured?
A: The majority of silicone breast implants fail (breast implant rupture) by the development of a small tear or hole that develops from fatigue fracture of the shell in one area. But acute high impact trauma, like from the deployment of an airbag, is one example of the type of force impact that could cause breast implant failure. With considerable bruising of the breast and pain you understandably have legitimate concerns about the integrity of the underlying breast implant. For a variety of reasons, including legal documentation, you should have the breast implant evaluated. Either an ultrasound or an MRI would provide a good assessment of the integrity of your breast implant. You should see a board-certified plastic surgeon for an evaluation and to have the appropriate test ordered.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in skull reshaping surgery for the back of my head. I have attached some pictures. Although they are a little fuzzy I think you can see the problem. The left is much flatter than the right. Let me know if it is possible to do what I want which is to fix the head shape so that it is more round and therefore more normal in the back on both sides (more on the left than the right.) I also have a few more questions to ask. First of all, are there any long term side effects of the surgery? (not the rare ones but common ones I should know about as I know there are risks with any surgery). Secondly will I need to keep coming back for surgeries in the future (for such things as touch-ups)? Will it affect my hair growth? These are questions I was unable to find out for myself. I hope I have not been too much much of a bother. I am really excited for this as you can see and I really, really appreciate your prompt and helpful responses. Thank you for everything.
A: As skull reshaping surgery goes, your back of the head problem is the most common skull problem that I treat. Flat back of the heads are common and rarely are they perfectly symmetrical. They are corrected by an onlay cranioplasty procedure, most commonly using PMMA as the augmentation material. The surgery is done through a limited 9 to 10 cm incision (no hair is shaved) placed closer to the back of the head through the material is applied and shaped. The only short-term complication (< 6 months) that I have ever seen is aesthetic in nature, how smooth is the applied material and does it give enough of the desired augmentation. If either is observed and bothersome, a touch up procedure may be done to smooth it out or add more material if possible. I have not seen any long-term complications. If one has a satisfactory result by three months after surgery to their own assessment, then no further procedure will ever be needed. Lastly, he procedure does not affect hair growth.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question about temple implants. What I want is to build width and length to my face through multiple procedures. (Not all done at the same time of course). These include jaw implants to add width and vertical length to the face, a chin implant which meets the jaw implant, and forehead widening from the temporal region up into the sides of the head, and possibly heightening. I believe the chin and jaw implants are relatively straightforward, but the forehead is a bit more complicated to me. Is the recovery period painful for skull reshaping and is there a significant loss of blood? One question I’d like to ask is how much width can be added to the forehead on each side? Is it possible to broaden the forehead up to 1cm on each side stretching from the cheekbone all the way up to the highest part of the head? As you can tell I really want to completely restructure my face to more large proportions and just add volume all over as it has bothering me greatly for some time now. I do not want to do anything with my features as I like my features, its the size of my structure that I really want to change.
A: When it comes to temple implants, there are two major factors to consider in your specific request. First, the amount of temporal and forehead augmentation is only limited by the ability of the scalp to close over it. Based on a lot of experience in these kind of surgeries I would say that a 1 cm increase on each side is very achieveable. Secondly, it will require custom designed temporal implants that would be made to start at the zygomatic arch and create a maximal 1 cm width increase at the point of maximal convexity as it blends into the forehead area. I have designed such temporal implants in the past so this amount of temporal volume addition I have done before.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a sliding genioplasty but want to know how much it can change the shape of the chin? What is the maximum vertical height and horizontal projection I can receive?
A: The maximum chin changes that can be achieved with a sliding genioplasty is based on the thickness of the chin bone, particularly as it relates to increased horizontal projection. You do not want to move the osteotomized chin bone beyond contact with the superior fixed chin bone. In general, that puts the advancement in the 10 to 12mm range which based on your picture seem more than you would need. As for vertical lengthening, the amount that the osteotomy can be opened depends on whether the created gap would need to be grafted. (with an hydroxyapatite block) For openings up to 5 or 6mm, no graft would be needed. But anything beyond that (8 to 10mms) would need to be grafted. Again, that distance seems greater than your picture would indicate that it is needed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in inverted nipple repair. However I don’t know anything about the procedure and how it is done. Can you help me with that information.
A: I believe you are inquiring about correction of inverted nipples. They are several types of inverted nipples based on the degree of fibrosis/tethering that is causing the inversion. The degree/type of nipple inversion cabe be determined by several factors including its presence since breast development or only developing after pregnancies/breast feeling and whether the nipple can be temporarily everted by gently squeezing it between one’s fingers or not. While all inverted nipple repairs are done by making an incision at the base of the nipple and the tether released, those inverted nipples with the greatest degree of firm inversion may require a small graft, usually fat, to fill the space that is caused by the nipple moving outward. Suturing the space beneath the nipple to hold it outward is a common technique but I have found that to be unreliable long-term at preventing relapse and recurrent nipple inversion. Thus the use of a fat or dermal graft can be very beneficial. In many cases an inverted nipple repair can be done under local anesthesia or conscious sedation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had an endoscopic brow lift to help lift my upper eye lids. Although I had an upper blepharoplasty done over three years ago, that surgeon not only did not remove enough skin to eliminate the ‘hoods’ over my eyes, he did not take precise measurements before surgery (he ‘eyeballed’ the distance, no pun intended, as if he was about to saw a piece of 2 by 4 wood). As a result I ended up with very little to show for that surgery – other than insufficient skin removed – and the brow lift was intended to correct this. Unfortunately, all that I appear to gotten out of the brow lift is two incision lines in my forehead (thankfully hidden – for now – in my receding hairline) and a couple of bumps in my forehead (where the dissolvable endotine ‘screws’ were presumably fitted). My middle brow (over my eyes) was not lifted. My upper lids are just as ‘hooded’ as they were before this surgery, and I am now being told that what needs to be done next is a revision blepharoplasty – a procedure I had asked about having done before the brow lift. It looks like I may have paid for what may have only been a ‘temporal brow lift’ and not a true middle brow lift, and I still need the revision blepharoplasty that I perhaps ought to have had done instead of this endoscopic brow lift.
A: The endoscopic brow lift, and in the results obtained, are highly dependent on the location of the scalp incisions. Where the scalp incisions are above the brows will determine exactly where the direction of maximal brow lifting is done. Unless the scalp incisions are directly in line above the medial brow areas, this area will not be lifted. In addition, in men, the effects of any browlifting is more modest. Thus any residual upper eyelid skin will not be removed and should be dealt with at the same time as the brow lift. It sounds like your case illustrates all of these points.
Q: Dr. Eppley, I had a subnasal lip lift a month ago and it clearly has been overdone. My upper lip, which now does show more teeth, looks like a snarl. My upper lip is too short. What I do not understand is how I could have only ended up with 12 mm of philtral length when I had 21 mm to start with? It sounds like 9 mm of upper lip skin was removed? Although that’s only 2 mm more than the maximum for females, it’s almost 4 mm (or double the maximum distance for females) that should be shortened for a male. Although we are only talking millimeters, that’s like a ‘moon shot’ missing it’s target by hundreds of thousands of miles! What can be done to fix an overdone lip lift?
A: A subnasal lip lift notoriously has 1 to 2 millimeters of ‘relapse’ so I would not rule out that some lengthening all occur despite how it feels. Given that it is just about a month after the procedure, I would start to stretch out the upper lip using your fingers and your tongue from the inside. You might be surprised what can happen by six months after surgery.
As for the techniques that plastic surgeons use to ‘mark’ their surgery, I can only speak for how I do it. It is important to mark out such surgeries beforehand using calipers and magnifying loupes to design the surgery. Just because it is marked out carefully does not always ensure a perfect result but without such precision in the plan the result will have no chance to be close to the desired goal. As the old motto goes ‘You Can Not Hit A Target You Do Not Have’.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have read you perform temporal artery ligations. I am considering this procedure since I have two very prominent arteries on both sides of my head that are very visible.
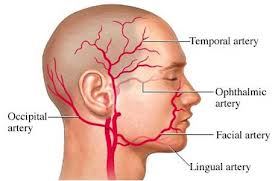 A: Temporal artery ligations can be done and doing them is actually not rare in my experience.. They usually require at least a two-point and sometimes a three-point ligation to make sure there is no unchecked flow into the ligated artery either through the main superficial artery trunk (anterograde) or from retrograde flow from the distal end of the vessel. These require small incisions (4 to 5mms) in the temporal hairline and at some distal location in the forehead/temporal area. They are done under local anesthesia as a simple outpatient procedure. Since you have two prominent temporal arteries, which are likely just branches of the same vessel, I would need to see a picture of the prominent vessels to see where the ligations would need to be.
A: Temporal artery ligations can be done and doing them is actually not rare in my experience.. They usually require at least a two-point and sometimes a three-point ligation to make sure there is no unchecked flow into the ligated artery either through the main superficial artery trunk (anterograde) or from retrograde flow from the distal end of the vessel. These require small incisions (4 to 5mms) in the temporal hairline and at some distal location in the forehead/temporal area. They are done under local anesthesia as a simple outpatient procedure. Since you have two prominent temporal arteries, which are likely just branches of the same vessel, I would need to see a picture of the prominent vessels to see where the ligations would need to be.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to get a corner of the mouth lift. I am a 43 year old Asian female with no fold. I have a neutral corner of mouth, but I just want to have a happier mouth when I’m not smiling.
 A: The corner of the mouth lift is traditionally done for aging in which the corners of the mouth are turned down. By removing a triangle of skin from just above the mouth corners, the lateral commissure point is moved upward. While it does produce a small scar (usually about 7mms in length) that tails away from the corner of the mouth, it creates a very noticeable change in the location of the mouth corners.
A: The corner of the mouth lift is traditionally done for aging in which the corners of the mouth are turned down. By removing a triangle of skin from just above the mouth corners, the lateral commissure point is moved upward. While it does produce a small scar (usually about 7mms in length) that tails away from the corner of the mouth, it creates a very noticeable change in the location of the mouth corners.
In the neutral or non-downturned mouth corner, such a lift creates upturned mouth corners also known as a ‘lip curl’. Such a mouth shape has become popular in Korea and Japan as a sign of a beautiful mouth shape. While imparting an upturned mouth is the opposite of what is desired in the Caucasian aging mouth, this is a modern day use of an older plastic surgery procedure for a more contemporary application.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in getting Botox injections to treat my severe clenching and grinding. I have tried every dental approach from teeth adjustment to splints and none of them have really done anything. I am worried about the wear on my teeth which is starting to become noticeable. You seem to be the only doctor in Indianapolis that does these type of injections for this problem. I would like to know the average cost of one treatment and average time it relieves the forceful grinding of bruxism.
 A: I have done Botox injections for bruxism (grinding, clenching) for well over a decade. In the right patient, it can be tremendously effective if administered properly. As a general guideline, most patients should have 20 units of Botox injected into each masseter muscle for a total of 40 units. This would be the minimum effective dose but a good starting point to see how effective Botox may be for the bruxism. If I inject the Botox it is $16/unit, if my nurse performs the injections then it is $10/unit. The effects of Botox take up to a week to see its effect as it works by depleting the available neurotransmitter acetylcholine, so what it stored up has to be used up before the muscle fibers stop firing.
A: I have done Botox injections for bruxism (grinding, clenching) for well over a decade. In the right patient, it can be tremendously effective if administered properly. As a general guideline, most patients should have 20 units of Botox injected into each masseter muscle for a total of 40 units. This would be the minimum effective dose but a good starting point to see how effective Botox may be for the bruxism. If I inject the Botox it is $16/unit, if my nurse performs the injections then it is $10/unit. The effects of Botox take up to a week to see its effect as it works by depleting the available neurotransmitter acetylcholine, so what it stored up has to be used up before the muscle fibers stop firing.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in liposuction or a tummy tuck, preferably liposuction though. I have had two pregnancies, seven years apart with the last one being five years ago. This has left me with loose skin and fat around my mid section. I am 38 years old and weigh 140 lbs and have a 34″ waistline measurement. I feel great, I just can’t get rid of the skin and fat around and under the naval area. I have had two abdominal surgeries in the past and skin hangs over the suprapubic scar. If I just have liposuction will I be left with flabby skin?
A: As a general rule, if one has significant loose skin on their abdomen before liposuction they will still be loose skin afterwards. While many forms of liposuction have been touted about their ability to tighten skin, the amount of skin tightening obtained is almost always far less than what patients desire. As I always tell patients, liposuction can tighten skin in the range of millimeters, however, patients are interested and need skin tightening in the range of centimeters most of the time. With loose skin around the belly button and overhanging a suprapubic scar, you would be better served by having a mini tummy tuck which would incorporate liposuction with it. Given that you already have a suprapubic scar you might as well take advantage and use the entire scar for a mini tummy tuck. It does not add that much more scar length and its ability to remove skin make it more than a worthwhile trade-off.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a reduction otoplasty. The height of my ears is too tall for my head/face. I have talked to several plastic surgeons about ear reduction and they all say that it can’t be done without severe ear distortions and scarring, which is very disappointing to me. Like I said I have been to a few surgeons who specialize in otoplasty and what bothers me is mostly the top portion. I have found only one surgeon who has pictures of this procedure, unfortunately he is retired. Do you know of anyone who would be able to preform this? Thank you so much for your time, it is greatly appreciated.
A: The traditional method of vertical otoplasty reduction, through a wedge technique, would result in significant upper ear deformation. What you are demonstrating is a different technique, known as a helical flap method, which can reduce the upper 1/3 of the ear without such deformations. It is actually a technique borrowed from ear reconstruction from the resection of skin cancers in the upper helical rim which is a common location of such cancers. That would be the technique of choice when it is the upper ear that is the source of the vertically long ear. It places the incision/scar line at he favorable location of the underside of the crus and the junction of the helical root rather than directly across the helical rim at a 90 degree angle. It would reduce the height of the ear by 8 to 10mms which is a noticeable amount.
Dr. Barry Eppley
Indianapolis, Indiana