Your Questions
Your Questions
Q: Dr. Eppley, What are the limitations to a custom skull implant to add ~1 inch in height? Is a specific skull shape required for this?
A: For heightening purposes the skull implant would have a design that covers the top of the head with edges that cross over the bony temporal lines.
The limitations of any aesthetic skull implant is how much the overlying scalp can stretch to accommodate what lies underneath it on the bone. As an immediate insertion technique (no prior scalp expansion) the limitation is around 150cc in volume or 1.5 to 2cms of maximum projection.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in forearm implants. I have worn long sleeve shirts most of my life and finally wanted to look into escaping this dilemma of embarrassment. Here are photos of the left and right arms. Thank you.
A: Thank you for sending your forearm pictures. By these pictures your area of arm augmentation is the anterior forearm or the wrist region. In this anterior area of the forearm there are no larger muscle bellies in which to place an implant under its fascia. (unlike the upper forearm with the brachioradialis muscle) That does not mean that wrist implant augmentation can not be done, just that it would have to be done on top of the muscle fascia under the skin. I am envisioning the implant location as shown in the attached picture. With an ultrasoft solid silicone implant design with feathered edges I believe such an anterior forearm/wrist implant can be successful.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, am middle aged male. Looking for guidance on which facial procedures for refresh and masculinization. I’d like custom silicone brow implant, full jaw implant. I have ok mid forehead brow bone, but outer area of eye socket bones is deficient (eyes are vulnerable to impacts due to lack of outer brow bone vs. socket depth). I also need brow lift (approx. 1.5mm lift of eyebrow?), modest blepharoplasty uppers (I’ve had hooded outer uppers since childhood so looking for mild upper job and fat transfer to plump up upper area below eyebrow).
So, can you tell me if I should get brow augmentation procedure 1st, then wait a few months for my ageing skin to settle in around implant, before continuing on with brow lift and uppers bleth? I plan to get eyebrow transplant also to boost outers of eyebrows.
Chin angle in profile is a little recessed also, is this always a separate implant to remedy? Separate from full jaw implant that is. I would need neck lift after implant, slight joweling now along with some turkey neck, mid face is still pretty good. I thought to plump up cheeks with fat transfer. I have significant jaw bone loss around teeth due to long time periodontal disease (under control/frequent visits to perio as always).
OK, looking forward to your recommendations.
A: Thank you for you inquiry and detailing your concerns. Your supposition is correct in most cases….get the foundational work first before doing any manipulation of the aging overlying soft tissues. The swelling from the brow bone augmentation is most cases is counter productive to the soft tissue work. HOWEVER if the brow bone augmentation is limited to the tail of the brow and lateral orbital rim then it would make sense to combine that with upper blepharoplasties and browlift because these procedures are incisionally and pocket dissection synergestic and the swelling from the brow bone augmentation is not much worse than from the browlift alone. The need to separate these procedures is when a full brow bone implant is needed which requires extensive dissection from above.
Otherwise a full jaw implant includes the chin area as well.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a man from Norway with a uncommon situation. My skeletal proportions are quite un-manly. My shoulders are very narrow, and I have quite wide hips and large head. I understand you perform clavicle lengthening procedure for widening the shoulders. So I have been wishing for and contemplating such surgery for a long time. Do you accept patients from other countries?
A: Thank you for your inquiry in regards to clavicle lengthening. In answer to your questions:
1) My practice has patients from all over the world, some even from the beautiful country of Norway.
2) Clavicle lengthening surgery is in its infancy so to speak so only a handful of patients have been done. But the techniques developed for it come from its companion procedure, clavicle reduction, where many more patients have been done in the past five years.
3) As part of the preoperative assessment/qualification it would be good to look at some shoulder pictures of you and do some computer imaging of potential changes.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I recently ran across this 2021 paper titled “Waist Narrowing Without Removal of Ribs”. What do you think of it? I have a boxy waist; but I store most of my fat viscerally, which means that I’m not a lipo candidate. I’ve always wondered about rib removal, but I’ve been worried about the possibility of chronic pain or other long-term complications. Would a procedure like described in this paper this be safer?
A: As I have stated in the past, the concept of rib fracture rather than rib removal is a viable approach. The key to its success is the need to corset regularly for at least 2 months after the surgery to successfully reshape the ribs. It is not a question of which one is safer, as rib removal surgery is very safe and has never in my experience had any complications at all, but that rib fracture offers a shortened recovery period and less operating time to perform. The unknown question is which lower ribcage modification approach, fracture vs removal, offers superior results for waistline narrowing, or are they virtually similar in effectiveness. That answer will probably never be precisely known. So for now and into the foreseeable future potential surgical waistline narrowing patients should make that decision based on what recovery period they need and how motivated they are to adhere to a postoperative corseting garment.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I wanted to ask your opinion about the appropriate timing of intralesional 5FU to a post auricular scar- Is 8 weeks post surgery sufficient time to commence the intralesional injection?
A: 8 weeks is fine to start scar injections with 5FU, sooner would have been even better.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I got a sliding genioplasty three months ago. I like the projection of my chin on the profile but I have some concerns. First, I have noticed that there are step offs on both side of my jawline. The step off is more pronounced on the left side than on the right. Is there a change that the step-offs will be filled naturally over time? How long should I wait to see if they smoothen naturally? The second concern is that my chin is a bit long. I am wondering if, after three months, I can still expect the swelling to decrease. I have read that after three months not many changes will be produced but I have also read many testimonies of people who said that they noticed significant changes at 6, 9 and 12 months. What should I expect according to your experience? I personally noticed a significant reduction in swelling from month 2 to month 3, can I still expect changes? Also, I noticed that if the swelling is reduced, I would have a more smooth jawline because the chin would blend better with my jaw. What do you think?
A: In answer to your post sliding genioplasty questions:
1) The bony stepoffs on the side will not improve with further healing. They may even worsen a bit (soft tissue contracture into the induced bone defects) but certainly they will not get better or go away.
2) The vertical length of the chin is also not likely to change with further healing.
The only benefit of time with the lateral stepoffs or the vertical length of the chin is that these aesthetic tradeoffs from the procedure will become more acceptable and you can avoid any additional efforts to improve them. Time also has the benefit of proving whether further healing will reduce their visual appearance.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have noticed just recently you have published a clavicle lengthening result with a video. I am just wondering a few things.
1. I know you were able to get 18-20mm of actual bone width, how much did the patient gain in bideltoid actual measurable shoulder width?
2. How can I personally prepare for a procedure? I know you mentioned shoulder stretching, could that actually make a difference?
3. Could patients move their arms after the procedure?
I am interested in this procedure personally and would like to get the best possible result. Thank you.
A: In answer to your clavicle lengthening questions:
1) There is generally a 1:1 ratio of what occurs at the inner third/half of the clavicle to the increased width at the outer deltoid area. This is because in clavicle lengthening there is a roll back effect on the shoulders as well.
2) Decreased shoulder/scapular tightness is of benefit during such surgery to achieve the optimal lengthening. I would refer you to this link to read more on this topic. https://exploreplasticsurgery.com/preoperative-sho…widening-surgery/
3) While a normal range of arm motion is not permitted during the first few weeks after the surgery, and you wouldn’t be able to do that anyway due to expected discomfort/tightness, limited arm movements are permitted.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I recently ran across this 2021 paper titled “Waist Narrowing Without Removal of Ribs”. What do you think of it? I have a boxy waist; but I store most of my fat viscerally, which means that I’m not a lipo candidate. I’ve always wondered about rib removal, but I’ve been worried about the possibility of chronic pain or other long-term complications. Would a procedure like described in this paper this be safer?
A: As I have expressed in the past, the concept of rib fracture rather than rib removal is a viable approach. The key to its success is the need to corset regularly for at least 2 months after the surgery to successfully reshape the ribs. It is not a question of which one is safer, as rib removal surgery is very safe and has never in my experience had any complications at all, but that the rib fracture method offers a shortened recovery period and less operating time to perform. The unknown question is which lower ribcage modification approach, fracture vs removal, offers superior results for waistline narrowing, or are they virtually similar in effectiveness. That answer will probably never be precisely known. So for now and into the foreseeable future potential surgical waistline narrowing patients should make the procedure choice based on how motivated they are to adhere to a several month postoperative corseting regimen.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m a 34 year old female. A little over a year ago I had sliding genioplasty surgery due to having no chin. I’m slim and I’ve always had extra fat around my jawline, almost as if I don’t have enough bone for the skin if that makes any sense. I’m somewhat satisfied with my genioplasty, however, my jaw area still has loose skin. I’ve had this since I was in my teens making me feel old. Is there more I could do to improve my jawline?
A: As for the jawline there are two fundamental approaches…augmentation or reduction. Reduction means liposuction of the submental and jawline and/or a jowl tuckup procedure. Augmentation means a total jawline augmentation. Each approach has their advantages and disadvantages with different aesthetic outcomes. It comes down to how much effort one wants to put into it and what type of improvement one is looking to achieve.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a sliding genioplasty 6 months ago and whenever I close my mouth this ‘ridge’ of skin appears on my chin. Could this be the plate and screws causing this or is there too much tension on my skin? Thank you
A: It is a soft tissue adhesion/scar contracture. Whether removing the plate and screws alone will solve it or that combined with a small fat graft is needed is the only debate.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have been researching for a long regarding the application of custom implants and the techniques proposed by many were undertook a ‘one suits all’ outlook which for me is the hallmark between an average and leading figure in his field. The attention to detail and to attending each case differently is what yields a high probability of results that achieve the correct look for both the surgeon and the patient. The technique/s, implant design and photos illustrated below in the link below are what I had in mind for years and upon seeing & this reading the link, I can honestly I feel like this long and eternal stretch of a search is finally over.
Plastic Surgery Case Study – Custom Infraorbital-Malar Implants for the High Cheekbone Look
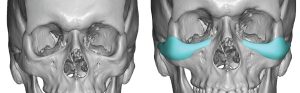
 A: Thank you for your inquiry and sending your picture. I would agree that the IOM (infraorbital-malar) implant concept is appropriate for what appears to be your aesthetic facial needs. (see attached) The basic footprint of the implant design, while changing somewhat with each patient, what really varies is the various thicknesses/topography of the implant design amongst each patient.
A: Thank you for your inquiry and sending your picture. I would agree that the IOM (infraorbital-malar) implant concept is appropriate for what appears to be your aesthetic facial needs. (see attached) The basic footprint of the implant design, while changing somewhat with each patient, what really varies is the various thicknesses/topography of the implant design amongst each patient.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a couple more questions. How tall is your highest rib cartilage for nose bridge augmentation? How tall is your highest rib cartilage for brow bone implants? In millimeters. I have a flat ethnic nose bridge and a low brow bone.
A: The upper end of most brow bone implants is in the 7 to 8mms range. Rib grafts to the nose are in the 7 to 8mm range also. Both are somewhat controlled by the tolerance of the soft tissues to stretch to accommodate what is placed beneath them.
Given the need for brow bone and nasal bridge augmentation one consideration is a one piece brow bone-nasal implant design. You can’t make a brow bone implant out of cartilage.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Since it’s been a couple months since this case-study was posted, I was curious if the plates and screws are meant to be removed eventually? Or will they have to be kept on forever? If they are kept forever do the plates/screws cause issues when going through air-port security? Also will people be able to feel them if they touch my shoulders?
A: The fixation hardware used in clavicle reduction surgery can be left in forever or removed as soon as 6 months after the surgery. Their removal is a personal choice. To date after five years of doing this type of surgery only one patient has requested hardware removal. Their titanium composition does not cause problems with airport security or in MRI studies. I can not speak to whether someone else would be able to feel the presence of the hardware as no one has mentioned that as an issue to date.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, How long does it take for the dermal fat graft to level out/settle?I am 3 weeks post op, approximately how much more will it shrink?If it is too big after the healing time is complete, can it easily be made smaller/more leveled out?mI think he told me this, but I can’t remember and haven’t been able to find these answers online.
A: In answer to your labiomental fold dermal-fat grafting questions:
1) 6 to 8 weeks for dermal-fat graft settling to occur.
2) The grafts can also be reduced secondarily but I have never yet seen someone request to do so. In the long run it often is the opposite issue….I would like some more
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Should I have rib removal before a plasma liposuction / tightening procedure or after it?
A: Ideally you would do it before because….what you are hoping is that the effect of the plasma liposuction makes the need for rib removal surgery unnecessary. You use rib removal as the last ditch effort to achieve what every other procedure can not do.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My main chin augmentation goal is increased width, with some minor increased horizontal projection, and little to no vertical increase. I’m now leaning towards a Terino Square Style II (size small). From what I gather, the dimensions for that specific implant would be 4cm in width across the chin, a total of 7.8cm in width along the chin and jawline (thanks to the wings), and 4.7mm of horizontal projection. Do I have this correct?
A: I find both style 1 and II square chin implants very aesthetically unsatisfactory. They were designed 30 years ago and custom implant designing has taught me how poorly designed they are by comparison. Neither make the chin more square in appearance as the corners are very round. Style II is way too wide as no patient ever needs 40mms in width, 35mm is usually the maximum. They are too skinny in height and end up looking like a rail across the front of the chin. The back wings of the implant for unknown reasons are tilted upwards rather than continuing with the shape of the jawline going posteriorly. When ‘forced’ to use them I choose a more projecting implant and cut off the front edge to make it more square as well as trim off the top part of wings to keep them from going too high along the jawline.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a man and I am 20 years old. I do not have any relevant disease, except allergic rhinitis. I have a question about my brow ridges. I notice them a little big, but I have consulted with doctors and they have told me that they are normal. My dad has it similar. I have also noticed that my left superciliary arch is a little larger than the other one. I suffered a strong blow to my left eyebrow when I was around 5-6 years old. I am not planning to undergo any surgery, I would just like to know if my superciliary arch is normal. I am from Latin America and I really do not have the economic means to undergo surgery. Thank you very much
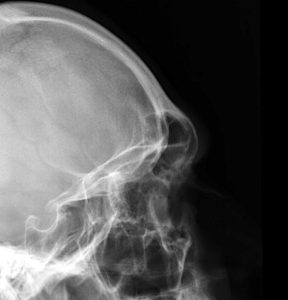 A: The size of the brow bones is a reflection of the development of the underlying frontal sinuses which creates them. Since the frontal sizes are often paired and the two sides are separate asymmetric development of them is not uncommon particularly in men whose natural frontal sinus development is more pronounced than in women.
A: The size of the brow bones is a reflection of the development of the underlying frontal sinuses which creates them. Since the frontal sizes are often paired and the two sides are separate asymmetric development of them is not uncommon particularly in men whose natural frontal sinus development is more pronounced than in women.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have read your informative post about Bullhorn Lip Lift.
My operation was about 7 weeks ago and i think i have the problem with the distortion of the nostril 🙁 The nostrils are much wider than before the surgery. Im very sad about this.
Can you tell from the pictures and the scar whether this is a residual swelling and whether the nostrils are getting smaller?
My doctor told me that a Bullhorn lift will not change the nostrils and from the internet i only found your statement in that direction 🙁
Thank you for your answer and your opinion !
A:Presuming your before and after pictures are taken at the same focal length, measurements do not show any appreciable nostril widening. (see attached) They actually measure identical linear lengths. While they visually appear so that is not what a measurement shows. I believe they appear so because with the vertical lip shortening the linear width of the mouth is now closer to the nasal base….creating the illusion that the nostrils are actually wider.
At 7 weeks after surgery there is no appreciable swelling present nor would I expect the nostrils to shrink down in size.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi. I am looking forward to proceeding with buttock implants. I just had a few questions, thank you so much in advance.
Would it be possible if I could get a Euromed implant that we could use that for the buttock implants?
What would be the difference between a buttock implant and a breast implant for buttock augmentation?
I’ve heard of the dual plane method, that it can project the top part of the glutes. What would be the benefits of that method vs completely under the muscle?
My goals are to try to keep the implant less visible. And for the implant to be softer. But what would be the advantages and disadvantages of having a breast implant vs soft silicone implant placed under the muscle? As far as long-term ect.
Also does the breast implant project the same as a silicone implant?
I noticed online you have an implant that you place holes in it to allow the tissues to grow into the implant. Is that method used under muscle as well? Does that make the implants stay in place better long term?
Will I be able to train squat etc the same in the gym after?
Would I be able to see the implants when I bend over?
I did get a fat transfer over 3 weeks ago to see how it would look and I love it but, I feel that I do still need an implant, to give more upper pole fullness projection, and I trust you for this type of procedure. You are amazing!! I am excited!!! How soon can I proceed with getting buttock implants? My fat transfer was almost a month ago, therefore what would be a recommended timeline to proceed with buttock implants? I would like to book a date for the procedure. I would like to also book a brief consultation beforehand if possible. Thank you!!
A:In answer to your buttock implant questions:
1) In the U.S. we can only use FDA approved implant devices. Medical devices from other countries that don’t have FDA approval can not be imported into the country.
2) The dual plane method refers to breast implants. In buttock implants the implant is either on top of the muscle (subfascial), partially in the muscle (intramuscular) or under the muscle. (submuscular) There are no deliberate dual plane methods although some intramuscular buttock implants do end up as ‘dual plane’ as the muscle thins over them and the central part of the implant ends up projecting through the muscle.
3) An ultrasoft solid buttock implant is fairly soft but not as soft as a breast implant…how different these are can be debated. Long term what you know is that a solid buttock implant will never rupture or need replacing. Another approach is to custom make the buttock implant and have it made in the softest solid silicone possible…which puts its feel pretty close to a breast implant.
4) Breast implants and buttock implants project the same.
5) The placement of perfusion holes in an implant is not done in buttock implants as the intramuscular pocket holds it adequately into place.
6) You would be able to squat train after buttock implants.
7) You would not see the implants in the intramuscular or submuscular pocket position when you bend over.
8) Given that you are 3 weeks out from fat transfer now and given the time to get the procedure scheduled you can get to work on that now.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,Hello, I have been a big fan of your work for years and have gone through your Q&A’s to answer a lot of my own questions. Last July, (10 months ago) I got a sliding genioplasty. My chin looks fantastic, however, I do have lots of tightness at the incision area. I would say that there has been no change in the tightness since November. Everything else has been healing nicely. My bottom teeth/gums are no longer numb, flossing is pretty much back to normal etc. Although my bottom lip feels tight, I would say I have 98% of my movement back. So all really looks and feels pretty good, minus the tightness. The tightness feels more severe than it looks. I feel sometimes like I may look like my lip is stiff while I am speaking, but it actually looks pretty normal. The tightness feels like a combo of it being pulled and like having a lot of food stuck in that area. Not sure if that makes sense. Its not painful, but feels very uncomfortable yet still pretty much works the same as before the surgery. Based on all of my internet research, I am thinking that my chin was pulled so far out (doctor said 13mm), that my tissue is most likely falling into that new empty space where my chin was extended. I love the way that I look and do not want to change it, but I also am slightly miserable with this tightness. I read that you do intraoral release and place of dermal fat graft. Not sure if that is relevant to my case, but if it were, how might that change what my chin looks like and what is the general cost for something like that? I am attaching before and after photos so that you have an idea of how much my chin was moved forward. Thank you for being quite the online resource.
A:Your diagnosis and the treatment for it would be the corrective approach. The bone has been expanded but the soft envelope remains the same. In essence you now have a bone shape that is beyond what the soft tissues were designed to contain.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I wanted to inquire aabout if 30mm of clavicle lengthening per side is possible.
A: One of the major limiting factors in clavicle lengthening is how much resistance is met by the shoulder girdle tissues. When lengthening the clavicle you are pushing out against the AC joint and all of its surrounding bony and soft tissue attachments. As a result, once the bone is cut (sagittal split completed) the shoulder does not unfortunately just fall to the side. (lengthen) This is quite different than in clavicle reduction where upon removing a segment of bone it does indeed fall inward. It requires a fair amount of force to get the bone lengthened due to the shoulder girdles tissue whose resistance must be overcome. This is why it is a challenge to just get 20mms of lengthening…and even that can be a struggle. This is why I thing there is merit in shoulder stretching exercises preoperatively to try and ‘loosen up’ the soft tissue attachments.
The other limiting factor is the length of the clavicle plate. The longest 10 hole clavicle plate is only going to permit three screws per side even up to a 25 mm lengthening.
Thus for anatomic and fixation plate restrictions a 30mm increase in any patient is not a technical possibility. I wish it were as more is always better but we are asking the body to do something beyond what it was designed/developed to be. As a result it does pose limitations sometimes from our ideal aesthetic goals.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in knee and thigh Lifts. I have a few questions:
1. On the site i saw picture of the knees after knee lift surgery ( see attachment). To get such a thin scar is there a special surgical technique or are products for scars enough?
2. after how many days I can fly after knee lift surgery?
3. How long I will be not able to bend my knees?
4. Does yo do a mini thigh lift?
5. in case of both procedures ( knee lift and thigh lift) after how many weeks I can fly back home oversea? It is long flight, about 12-14 hours.
Thank you very much for your reply.
A: In answer to your knee lift questions:
1) The key to having an acceptable knee lift scar is to avoid over resection and do the preoperative excisonal markings taking both the extension and flexion of the knee into consideration. A multilayer closure is done with subcuticular suturing for the skin.
2) You should be able to fly home within 48 hours after the surgery.
3) You should avoid bending the knee more than 45 degrees for 4 weeks after the surgery.
4) Please define your thoughts on what a mini-thigh lift is.
5) Even with a combined knee and mini-thigh lft procedure you should be able to fly home within 72 hours after the procedures.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello! I am a trans woman. I am extremely interested in your work on shoulder reduction surgery and I find myself consistently returning back to the few photos you have of before and afters online.
I have two questions for you, which I hope can be answered:
1. Are there more photos of before and after results from further away than just the shoulders available so i can get a better idea of what results will be like with respect to the entire body? Your case study post on the trans woman was exceptionally enlightening, but I would like to see a few more in order to decide if it’s something i actually want. I am curious how this surgery improves the shoulder to hip ratio and whether it can help shift patients from a more triangular body type to one more hourglass or pear shaped. Below is the case study i am discussing. Being able to see how she looked in the mirror helped quite a bit, but I think the most enlightening pictures would show full body shots.
https://exploreplasticsurgery.com/plastic-surgery-case-study-outcome-assessment-of-transgender-male-to-female-shoulder-narrowing-surgery/?doing_wp_cron=1650927706.0061049461364746093750
2. Have you had any experience getting this procedure covered by insurance? I have Blue Cross Blue shield, which recently updated its policy to cover breast augmentation for trans women, as well as a few other affirming procedures, but I know as this procedure is relatively new it may be some time before we ever see it formally implemented into insurance policies. If any individuals you have seen previously for this surgery have managed to get it covered somehow, I would love to hear some anecdotes about their experience and how they may have accomplished this.
As of now, this procedure is really one of the only things i’ve ever wanted, and would relieve years of painful dysphoria I’ve experienced as a result of my shoulders. Its effected me to the extent I find it progressively harder to focus and has impaired me in school and my social life because it has followed me wherever I go. If I could relieve this I can imagine my life would improve significantly.
Anything you could do with respect to above would be absolutely fantastic! Please let me know when you can.
A: In answer to your shoulder narrowing questions:
1) In respect of patient’s privacy I am limited as to the views I can show. In addition since all of my patients are not local, there is no return for an actual in office followup. All such followups are done in a virtual manner by Zoom.
2) I do not participate in insurance so I can not comment on whether shoulder narrowing surgery would be so covered.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi I just found out that there is a possibility to change the shape of the skull and searched a bit about the ways to do so. When you use bone cement how much of the result can it show, dose it only change the shape or can it also get a bit bigger?
A: The use of bone cements for aesthetic skull augmentation is a near historic procedure. The use of custom skull implants is the contemporary method which adds 3X the volume, has an assured shape and can be placed through smaller scalp incisions.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in 3d printed glabellar region implant. The result I want is natural and minimal. Currently I have has chin implant, check bone implant, temporal region implant and nasolabial implant. They all looks natural and conservative.
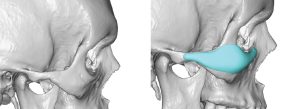
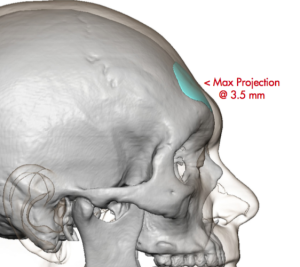 A: By your description you are most likely seeking a glabellar forehead implant similar to the concept as seen in the implant design attachments. To keep it as natural as possible I wold definitely stay under 3.5mm in thickness.
A: By your description you are most likely seeking a glabellar forehead implant similar to the concept as seen in the implant design attachments. To keep it as natural as possible I wold definitely stay under 3.5mm in thickness.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Also, want to double check that, given the clavicle(s) have had adequate time to heal, I should be able to resume heavy weight workouts–I am benching and rowing above 200 lbs multiple times per week, definitely not power lifting, but also potentially putting more strain on the clavicles than is standard. Not sure if these particular exercises would even be the ones I ought to be concerned about, but yeah, wondering if its possible to get some reassurance that this operation shouldn’t limit my ability to workout (again, assuming adequate time is allowed to heal the clavicle(s))
Thanks!
A:Provided adequate time is given for full bone healing, there should be no restrictions for those activities after clavicle lengthening surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in consulting about getting chin and jaw implants. When I was six I had cancer and extensive radiation delivered to my facial region resulting in a stunt of growth in my mandible.
Q:Thank you for your inquiry and sending your pictures. With the history of radiation in the area we have to be very cautious about treatment selection as that affects the involved tissues lifelong and their ability to respond to trauma and exhibit normal healing from it may be compromised. (at the least it has a higher risk of infection) I will need to see a 3D CT scan of your lower face (jaw areas) to have a better appreciation of the bony anatomy. With the history of radiation a custom wrap around jawline implant is out as the infection risk is too high. Thus, for now, I am thinking a bony genioplasty (you need mainly vertical lengthening anyway and jaw angle implants. The bony genioplasty will be fine, it is the jaw angle implants in the back we have to assess very carefully.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Here are some of my desired results from rib removal.
Waist: 28-30
Hips: 40
Inseam: 32
I really want that golden ratio of a .6 waist to hips. I think that a 26-27 inch waist with a 42-44 inch hips is a buffer. Here are photos of what I would like, I will attach photos of myself currently, with as little fat and showing abs for best results.
A:Thank you for your inquiry and sending your pictures. I think with your lean body frame the only way you are going to have a more narrow waist is with rib removal surgery. How much waistline reduction you can achieve with this surgery is never completely predictable so I would not specifically provide a waist measurement number for what can be achieved. The only outcome aspect of rib removal surgery that is assured is that once this is done there are no longer any further anatomic reductions that can be done. Rib removal surgery is the last stop on the waistline narrowing train.
Dr. Barry Eppley
Indianapolis, Indiana
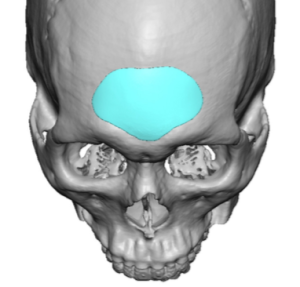
 Q: Dr. Eppley, Is such a skull implant possible for women with no effect on hair color and heat on it ??
Q: Dr. Eppley, Is such a skull implant possible for women with no effect on hair color and heat on it ??
A:Correct, the implant material only changes shape/breaks down at 375 degrees F.
Dr. Barry Eppley
Indianapolis, Indiana