Your Questions
Your Questions
Q: Dr. Eppley, My question is therefore whether submental placement of jaw and chin implants is to be preferred over intraoral in terms of safety and infection risk? I know Dr. Eppley has done both of these, but what are the pros and cons of going submental vs. intraoral?
A: In custom jawline implant placements, three incisions are needed….one anterior and two posterior. The two posterior incisions are always intraoral and are located way back in the mouth opposite the 2nd/3rd molars. The only ‘debate’ is whether the anterior incision at the chin area is intraoral or submental. To decrease the risk of infection and potential mental nerve injury the submental approach is preferred. In very small custom jawline implants that are used in some females the anterior intraoral approach may be able to be used but with that comes the aforementioned increased risks.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am going to “study” the custom facial implant design and get back to you on it. But I have two questions:
1) I see different measurements between the two sides, should I chose one of them or do I have an asymmetrical face?
2) Is it possible to get a computer simulation of ” my new face” with the lue implants?
Thank you very much and best regards
A: 1) When implant measurements are asymmetrical that is because the program sees an asymmetrical bone structure and that is compensated for in the implant design.
2) Custom implants are made for the bone and there is no software that can predict exactly how that will look on the outside. Thus much of the implant design is based on the surgeon’s judgment and experience of a likely aesthetic result. Knowing exactly what the aesthetic outcomes are from an implant design remains the missing part of the custom implant design process.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am currently considering getting a temporal reduction surgery, but I am wondering what the recovery process may be like for this procedure. I understand that for some surgeries, the recovery process can be quite long (a few weeks to months) and require certain types of diets, while for other surgeries, the recovery process can be very short (a few days or less). Thank you so much for your help!
A: The recovery from temporal reduction surgery is remarkably quick. Other than some expected temporal swelling there are no postoperative physical limitations. One can eat and drink immediately after surgery in an unrestricted fashion. Most of the swelling subsides by 10 to 14 days after the surgery.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I was considering getting implants for my bone brow. However i am a boxer, will these implants interfere with my boxing career and if so what can i do to prevent any damage.
A: While I have never put forehead or brow bone implants into a patient that boxes, I do not see it as a problem. You can’t break the implant and it would be hard to displace it with any force. It actually has an opposite effect…it adds a layer of protection or acts like a bumper guard for the bone.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, When would I have enough mobility to resume massage therapy work after clavicle reduction surgery? Could you also explain to me in more detail, how the recovery in mobility will evolve?
A: As a massage therapist I would think 6 to 8 weeks would be the soonest. That is fairly strenuous arm work. Whether that time period is too optimistic I can not say since I have never yet had a massage therapist.
The evolution of postop arm mobility does according to the following schedule:
1st 2 weeks = keep elbows at side as best as you can
2nd 2 weeks = arms can go out ot 45 degrees
3rd 2 weeks = arms can go out to 9- degrees.
4th 2 weeks = full range of arm motion allowed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I plan to get orthognathic surgery in the near future which will change my jaw most notably so I didn’t include a side profile but I still have some concerns with some frontal features that seem like they cause poor facial harmony. My first concern that I wanted to bring up is the width of my lips. They are quite narrow and the fullness of them exaggerates that as well. I also think I could benefit from eyelid procedures to make me eye area appear less droopy and sad and make them more awake and angular.
A:The problem with mouth widening in patients with full lips is that it not well seen…as the height of the widened lips would be so much more narrow than the natural fullness of the rest of your lips.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had otoplasty 6 months ago. Cartilage was removed from my conchal bowl and the antihelix was created by mustarde sutures (3 sutures per ear). I was very unsatisfied with the results since it was pinned too much to my head. 4 weeks ago i had a revision, and im still not very sure about the result. It got less, but still not as i wanted it to be. Is it possible you could take a look at some pictures and give me advice.
 A: I will be happy to look at your pictures but the bottom line undoubtably is…when an otoplasty is overcorrected and cartilage has been removed in doing so simply releasing it months later will make very little difference in the over correction. Effective subtotal reversal otoplasty requires some cartilage support to be put back to get a more effective and sustained change.
A: I will be happy to look at your pictures but the bottom line undoubtably is…when an otoplasty is overcorrected and cartilage has been removed in doing so simply releasing it months later will make very little difference in the over correction. Effective subtotal reversal otoplasty requires some cartilage support to be put back to get a more effective and sustained change.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, do you perform subcranial modified orbital box osteotomies?
 A: You are referring to a lower 180 degree orbital box osteotomy done through a combined lower eyelid and intraoral incisional approaches, an operation of which I am familiar and have done. It is certainly far less invasive than the transcranial 360 degree orbital box osteotomies which allows it to fall into an aesthetic operation for adults. It is, however, more limited in what it can accomplish and thus its primary indication is when 10mm or less of orbital widening (interpupillary distance increase) is needed. There are two variations of this type of limited orbital box osteotomy depending upon whether some cheek widening effect is also needed.
A: You are referring to a lower 180 degree orbital box osteotomy done through a combined lower eyelid and intraoral incisional approaches, an operation of which I am familiar and have done. It is certainly far less invasive than the transcranial 360 degree orbital box osteotomies which allows it to fall into an aesthetic operation for adults. It is, however, more limited in what it can accomplish and thus its primary indication is when 10mm or less of orbital widening (interpupillary distance increase) is needed. There are two variations of this type of limited orbital box osteotomy depending upon whether some cheek widening effect is also needed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a 23 yo female. I am actually quite satisfied with how I look from head on (I’ve no prior procedures). I’m dissatisfied with the slight nasal hump and nasal tip drooping, but am more concerned with the weakness of the profile of my chin.
I have considered going to local, domestic, and international surgeons. However I am fearful that I might go to someone who will not adequately address my concerns and that I will have limited improvement in my chin projection thus wasting my time and money. I’m impressed by your work and thoroughness and would rather travel to you for such an operation.
I anticipate a more aggressive approach to produce as much augmentation as possible. Potential through the use of multiple procedures/techniques. Sliding Genioplasty, Chin Implant, Custom Implant, and Chin fillers are all procedures that I’m open to. I don’t think I can make a well informed decision. I prefer an option that is permanent, offers significant projection to the chin, avoids severe labiomental fold, and that is within my budget. I will take your suggestion on what might be best.
A: In answer to your chin augmentation questions:
1) With the significant weakness of your chin you are only a candidate for a sliding genioplasty and not an implant. Your horizontal projection increase in the chin exceeds what any implant can do or the stretch of the soft tissues of the chin to accommodate that change over an implant.
2) The amount of chin bone movement you need is well into the double digits, probably in the 14 to 16mm range at least. (see attached imaging). In addition to coming that far forward it also needs to be vertically shortened to avoid making the chin longer which can inadvertently happen when that amount of chin bone advancement is done. The tightness of the soft tissues over the chin when it is moved this amount will preclude the use of a chin implant over it. That is best anyway as make your own natural tissues do all of the work of the augmentation.
3) The labiomental fold is going to get deeper which is unavoidable. That is the aesthetic tradeoff for any significant horizontal chin increase.
4) Patients coming in for surgery and traveling home is the norm in my practice, not the exception.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have microcephaly. My head circumference is 21cm although i have normal intelligence, this condition is psychologically distressing and has negatively impacted my self-esteem. I often stuff my wigs with clothe just to add volume to my head and give off an illusion of a semi normal sized head. Is a reconstruction possible for me that would make my head size bigger? that would be a dream since microcephaly is incurable and permanent. Thank you.
A: Skull augmentations using custom implants can provide some increases in head size based on how much the scalp can stretch to accommodate the underlying augmentation. Most significant head size increases require a two stage skull augmentation approach using a first stage scalp expansion.
To determine what can be done in your case I would need to evaluate and do some imaging using pictures of your head.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 45 year old man. I have desired testicle enhancement for many years, since I was in my early twenties. Now that I see that an implant that envelopes the testicles individually to enlage them is on the market, i would actually consider having such a prosedure done. I have previously had a vesectomy and I would prefer if at all possible for a potential prosedure to be done under local anasthetic.
A: In answer to your testicle implant questions:
1) I have designed and used various styles of wrap around testicular implants which is a clever concept for it. But it is plagued by a certain percent of secondary implant-testicle separations (testicle coming out of the implant) for which I have not solved how to completely prevent that postoperative risk from occurring.
2) This is not a procedure I would perform under local anesthesia.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I found you on the internet while searching for a resolution to un even butt cheeks. I’d love to have a virtual consultation if they’re offered.
A: Given the volumetric difference between the two buttocks and your lack of fat harvest sites (from a prior BBL harvest ??) the remaining treatment approach would be a small intramuscular buttock implant on the smaller side.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am scheduled to have a unilateral clavicle reduction but wanted to first understand the recovery process in more depth. I live in Montana and needed to understand the travel aspects (how long I need to be in Indianapolis), how long I will be unable to use my arm for computer office work, and whether I can manage on my own post-op since this would be a unilateral procedure. Any other pertinent info would be helpful, too.
A: In answer to your logistical surgery questions:
1) Having one good arm, which is unlike every clavicle reduction procedure I have done to date, allows for numerous advantages doing the recovery period one of which allows for a more rapid return home. Assuming you are coming by yourself you should be able to return home in 2 to 3 days after the surgery.
2) The key to the first few weeks after surgery is to keep the elbow of the affected arm near your side. While I have never used postoperative slings/garments after clavicle reductions due to their bilateral nature, you would represent the exception in which it is probably of benefit. Think of your one arm in a sling (not when showering) when determining how activities will be affected in the first few weeks after the surgery.
3) As a unilateral procedure you should be able to handle the immediate after care given that many bilateral patients do…albeit with more difficulty and requiring some nursing support.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have the prominent arteries on my temples which I would like to have treated. In my case a y shape branch on the right hand side and a single vessel on the left. The pulsate very visibly even at rest.
In addition to this I have a very visible pulse in general, especially in my neck and chest. On the right hand side of my face when it’s hot or I have exercised I can see my cheek pulsating and can feel this artery at all times running from my jaw, past my nose and up my forehead. My main concern with having the procedure done is that this artery pulsation would become worse and more visible. Have you seen this happen in any of your previous patients and if so is it safe to ligate this artery as well as the temporal arteries?
A: While prominent temporal arteries can be safely and successfully ligated, their larger origins along the ascending pathway of the external carotid artery (ECA) are a different story. You are describing pulsations along the entire ECA which can not be treated. Whether such ECA pulsatile visibilities bode poorly for successful temporal artery ligations or would make these more proximal pulsations more visible I can not say since your aesthetic arterial situation is not one I have previously encountered.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I want to do the hip implant to enhance my hip a bit what to know the price and I’m slim is it ok to do it. Thank you in advance
A: If you are slim with little subcutaneous tissue thickness over the hips you would not be a good candidate for hip implants as the risk of complications is too high.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hi. I have a chin implant from a different surgeon, and my chin still does not look quite as symmetrical as I would prefer. I’m interested in replacing it with a more customized implant, and was wondering what that process would involve. Would I first have to get my implant removed before getting CTI scan? And how long would the replacement take? Thanks.
A: You do not need to remove your chin implant prior to getting a 3D CT scan. The presence of the implant can usually been seen in the scan and is digitally removed to do the new implant design. Knowing what the existing chin implant looks like and where it is positioned on the bone is also helpful information in a new implant design.
The usual time frame from starting the design process to having it available for surgery is 3 months.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in the skull augmentation and also live out of state, hence would need to travel for this procedure if I were receive it. I was wondering, how many days would I need to stay in town after the procedure?
A: While I don’t know the skull augmentation procedure you need, most patients don’t need to stay more than a day or two after surgery.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in the Custom Jawline Implant Design procedure for high gonial/mandibular plane angle as I am insecure and bothered by my short chin and small Jaw . Is it possible for me to receive this treatment from you, even though I live in Spain?
A: Almost all of my patients are not local so patients far away are common in may practice. The need for a 3D CT scan and the entire design process is done in a virtual manner. You only travel here for the actual surgery. All follow-ups are done in a virtual manner as well.
Dr. Barry Eppley
World Renowned Plastic Surgeon
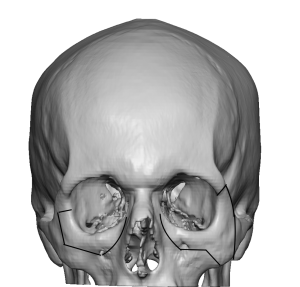
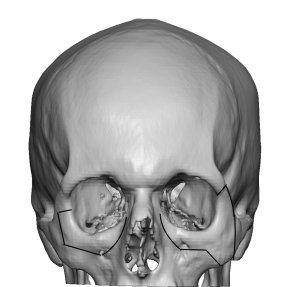
Q: Dr. Eppley, I have seen you are well qualified in the realm of orbital implants. I have also noticed that you use custom infraorbital rim implants over standard Medpor infraorbitals or Implantech tear trough implants — your proposal being that these custom implants saddle the infraorbital rim and increase vertical height whereas standards do not.
I am intending to get both infraorbital implants to increase horizontal cheek projection, as well as have lower eyelid repair (canthoplasty and graft). What is the benefit to this vertical heightening and customisability of the custom implants in my case? Wouldn’t a standard implant suffice considering my goal is horizontal projection and support to the lower lid through use of a graft? (I’ve heard the increase in vertical height helps support the lower lid, but given I’m also having the other procedure, I didn’t know if it was relevant in my case).
I would be very grateful if you could answer my question, Many thanks and kind regards
A: Any time you can add vertical height to the infraorbital rim it has a synergestic effect with lower eyelid repair…which I assume the goal is to elevate the rounded/sagging eyelid. If one of the contributing causes to the shape of the lower eyelid is the shape of the rim (there is a linear relationship between the shape of the lower eyelid and that of the underlying bone which supports it), then a 3D bony approach is superior to a 2D one.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hello! I have been searching extensively for a plastic surgery solution to my deep dark circle/hollow tear trough problem since i was young. I do not desire fillers or fat transfer because of the impermanence and unpredictability of the procedures respectively. I came across infraorbital rim implants which seem to have a beautiful and permanent aesthetic outcome. I was told by a dermatologist that the source of my deformity was a lack of sufficient bone structure around the eye region rather than tissue loss/migration. I had my own theory that an abnormally connected orbitomalar ligament also plays a role, where release may be necessary to correct the depth of the indentation. I read about the type 2 implant mentioned on your website and thought it would be perfect for me as it could fill my under eye area as well as give me a more chiseled cheekbone projection. Please let me know if this would be suitable or if something else could be done better. I’ve attached a photo for reference. Thank you very much
A: Anytime deep undereye hollows exist, tear troughs and rounded lower eyelids are present, there is an underlying bony deficiency. Thus infraorbital rim augmentation is needed. The only debate is in whether a standard style 2 infraorbital implants is adequate to whether custom infraorbital-malar implant which straddles the rim and added both vertical height as well horizontal rim projection would be better.
In placing infraorbital implants off any size or style it is always necessary to release numerous ligaments along the orbital rim from the tera trough ligaments out to some of the orbitomalar ligaments. (of which there are numerous ones)
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have 2000cc breast implants and for more Id like to get 3000cc to 35oocc can you this for me?
A: I will assume that your current breast augmentation has been done with 800cc saline implants that have been overfilled to 2000ccs….as that is the only way you can get that implant size in the U.S. To go from 2000cc volume to 3000cc volume would require adding to your current implants since there is no larger base implant sizes. Thus I don’t see any benefit to new implants in your case unless there is a reason to change the projection of the 800cc saline implant.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have some custom forehead implant questions for you.
Question 1: I was wondering if you could reshape a flat forehead into a youthful rounded protuding forehead I had in my early years using custom made forehead implants .I wanted a more concave forehead Ala Rihanna . Will it be able to look natural and not uncanny ?
Many people get frontal bone /brow bone reduction to change a concave forehead into a flatter profile is there such a procedure I can achieve the opposite
Lastly Will my forehead feel numb ? Can I still form wrinkles in my forehead ? Will my eyebrow position since I do Not want to change my eyebrow position or get a super shiny forehead . Lastly how is the scarring for the procedure like?
A: In answer to your forehead augmentation questions:
1) With the proper design a custom forehead implant would be the only way to get a more rounded and less inclined forehead shape.
2) Every forehead augmentation patient will have some temporary postoperarive numbenss andf stiffness of eyebrow/forehead movement. But this will resoolve within 6 to 8 weeks after surgery.
3) The way to avoid an uncanny/unnatural look after forehead augmentarion is to not make it too big.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, do you perform subcranial modified orbital box osteotomies?
 A: You are referring to a lower 180 degree orbital box osteotomy done through a combined lower eyelid and intraoral incisional approaches, an operation of which I am familiar and have done. It is certainly far less invasive than the transcranial 360 degree orbital box osteotomies which allows it to fall into an aesthetic operation for properly selected adults. It is, however, more limited in what it can accomplish and thus its primary indication is when 10mm or less of orbital widening (interpupillary distance increase) is aesthetically needed. There are two variations of this type of limited orbital box osteotomy depending upon whether some cheek widening effect would also be desired.
A: You are referring to a lower 180 degree orbital box osteotomy done through a combined lower eyelid and intraoral incisional approaches, an operation of which I am familiar and have done. It is certainly far less invasive than the transcranial 360 degree orbital box osteotomies which allows it to fall into an aesthetic operation for properly selected adults. It is, however, more limited in what it can accomplish and thus its primary indication is when 10mm or less of orbital widening (interpupillary distance increase) is aesthetically needed. There are two variations of this type of limited orbital box osteotomy depending upon whether some cheek widening effect would also be desired.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I have been searching extensively for a plastic surgery solution to my deep dark circles/hollow tear trough problem since i was young. I do not desire fillers or fat transfer because of the impermanence and unpredictability of the procedures respectively. I came across infraorbital rim implants which seem to have a beautiful and permanent aesthetic outcome. I was told by a dermatologist that the source of my deformity was a lack of sufficient bone structure around the eye region rather than tissue loss/migration. I read in a research article that an abnormally connected orbitomalar ligament can also play a role, where release may be necessary to correct the depth of the indentation. Furthermore, I read about the various customizable implants on your website and thought it would be perfect for me as i desire volume to be restored under my eye as well as an extension into the malar region to give me a more chiseled cheekbone projection that i am lacking. The tissue around this area appears to have a flat/sagging appearance because it doesn’t seem like there is enough support holding it up until i artificially mimic the motion with my fingers and lift up my cheeks. Please let me know if the implant would be suitable or if something else could be done better. I also desire more symmetry in my face as I have noticed that one side appears to be more developed than the other. I do not know exactly what procedures can correct this, as I haven’t researched too much into it, but if you can recommend something that wouldn’t be too surgically aggressive, that would be helpful for me. I’ve looked through many photos of your work and I greatly appreciate your aesthetic outcomes. I’ve attached two photos for reference of myself. Thank you very much
 A: You have correctly identified the proper treatment for your undereye hollows/tear troughs….infraorbital rim augmentation. The only debates are: 1) whether standard vs custom infraorbital implants are to be used (see attached) and 2) whether there should be a malar extension to them or not. The first one is not much of a debate as when you have known asymmetry beforehand using standard implants will almost always make the asymmetry appear more pronounced. That combined with the need in infraorbital bony deficiencies to add both horizontal projection and vertical rim height, only a custom infraorbital rim implant can make those dimensional changes. As for any malar extension to the infraorbital implant that is an individual aesthetic decision of which you have stated that would be a good addition for you..
A: You have correctly identified the proper treatment for your undereye hollows/tear troughs….infraorbital rim augmentation. The only debates are: 1) whether standard vs custom infraorbital implants are to be used (see attached) and 2) whether there should be a malar extension to them or not. The first one is not much of a debate as when you have known asymmetry beforehand using standard implants will almost always make the asymmetry appear more pronounced. That combined with the need in infraorbital bony deficiencies to add both horizontal projection and vertical rim height, only a custom infraorbital rim implant can make those dimensional changes. As for any malar extension to the infraorbital implant that is an individual aesthetic decision of which you have stated that would be a good addition for you..
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in testicular enlargement. I have attached some pictures of my scrotal ultrasound.
A:With natural testicles at 3.9cms on the right and 3.7cms on the left you are in the ‘gray one’ of the two testicular enlargement methods. If you were a bit smaller than the side by side method with 6.0cm or larger imnplants with a very low rate of problems could be used…and which is always the preferred method. If you were any bigger then the wrap around method is preferred with its relatively higher rate of complications which is always the risk of implant separation from the testicle. In this size testicle it tis always a difficult decision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in testicular enlargement. I have attached some pictures of my scrotal ultrasound.
 A:With natural testicles at 3.9cms on the right and 3.7cms on the left you are in the ‘gray one’ of the two testicular enlargement methods. If you were a bit smaller than the side by side method with 6.0cm or larger imnplants with a very low rate of problems could be used…and which is always the preferred method. If you were any bigger then the wrap around method is preferred with its relatively higher rate of complications which is always the risk of implant separation from the testicle. In this size testicle it tis always a difficult decision.
A:With natural testicles at 3.9cms on the right and 3.7cms on the left you are in the ‘gray one’ of the two testicular enlargement methods. If you were a bit smaller than the side by side method with 6.0cm or larger imnplants with a very low rate of problems could be used…and which is always the preferred method. If you were any bigger then the wrap around method is preferred with its relatively higher rate of complications which is always the risk of implant separation from the testicle. In this size testicle it tis always a difficult decision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in an implant that could give a more forward grown forehead/browridge and slightly reduce the slope as well as a vertically longer forehead. My 2nd interest would be correcting a very weak/almost non existant occiput. Ideally it should go from the browridge all the way to the end of the occiput. My last concern is that my head size is way too small for the rest of my body, so a rather large augmentation would be preferred. I would like to know under which price range such an implant would be in. Thank you.
A: Essentially what you are referring to is a one piece skull implant design that goes from just above the brow ridges all the back to the occiput. While that can be done such large surface area implants add a lot of volume in which the scalp has a limited ability to stretch to accommodate it. This the size/thickness of the implant must factor in the soft tissue scalp which means either a smaller volume implant is used and immediately placed or a two stage skull augmentation is done using a first stage scalp expansion to end up with an implant that would have double the volume.
To best understand the aesthetic differences between a one vs two stage skull augmentation with that surface area of coverage I would need a side view picture to do some imaging to show you those different effects.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a 26 old female and I write you because I have a concern about the shape of my forehead bone. I thought it was lack of fat and thin skin, because i can see bones in all my body, but I read one comment of you under the post of a girl with more or less the same case of me in which you was talking about frontal deformity. I would ask you if in my case it’s a deformity of the bone. Thank you and best regards
A:While you did not clarify your exact forehead shape concerns I am going to assume based on your pictures that you are referring to your forehead eminences also more commonly known as forehead horns. (paired upper forehead bumps) Whether that bothers you or not determines whether it is an aesthetic deformity. Presuming that it does those forehead horns can be reduced/burred down to have a smoother forehead contour.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I´m a 42 year old male interested in getting custom-made wrap around jaw (and chin) implants. While considered reasonably good-looking, I´ve always been lacking in self-confidence owing to what I perceive as receding, narrow chin and weak, underdeveloped, receding lower jaw. To address the aforementioned – I´d had a Medpor two-piece chin implant (5mm projection) inserted back in 2008. As it failed to address any one of the described issues, I´ve had it removed in 2015 and replaced with a large silicone chin implant, which, alas, also proved insufficient and inadequate in providing me with a full, robust, chin and lower jaw. To add to the existing problem, the implant also rotated downwards and suffice to say it doesn´t sit properly in its pocket. Since then I´ve tried to treat the receding jaw with fat transplant along the lines of my jaw but that failed to give me that chiselled and robust look the lower jaw should project.
That custom wrap around jaw and chin implant should address
1. receding chin – projection
2. narrow chin – width
3. “short” chin – vertical length
4. depressed jowls – projection
5. receding, underdeveloped lower jaw – projection, width …
Is that achievable? Can wrap around implants “elongate” the lower third of my face the same way Chin-Wing can? Since I have a fairly pronounced case of receding chin, would it be possible in one procedure to remove my silicone chin implant do genioplasty AND on top of that insert wrap around jaw and chin implants? Or is that rather too ambitious? The reason for asking is that I´d rather skip the hustle of undertaking several trips all the way from Sweden, Europe. Also, would fat transplant interfere in any way with the custom made wrap around implant, at least in terms of blunting the final results? If so, should/can it be removed during the surgery?
Finally, would it be possible to get an approximate cost estimate for the surgery at this point?
Of course, I do have more questions, especially in relation to patient safety (for patients outside the US), results, recovery, accommodation during my stay etc., but let us leave those for another time.
Thank You!
Looking forward to Your answers.
A:What you are describing by what you want to address is exactly what a custom wrap around jawline implant does. What it can achieve dimensionally is far superior to the chin wing osteotomy. Your surgical history describes exactly what the limitations of the procedures you have done for lower third of the face augmentation are. The only question is where the custom jawline implant is needed by itself (with simultaneous chin implant removal) or whether your chin augmentation needs as such that it is better to combine a sliding genioplasty with the custom jawline implant. That determination will require photographic imaging of your face as well as a 3D CT scan. Your fat grafts do not need to be removed nor so they pose any limitations in the result as they are likely of low volume.
When you get a chance please send me some facial pictures so I can begin the imaging process. The 3D CT scan can be done in your country as my many Swedish patients get in their geographic area.
All surgical planning is done in a virtual manner so you only come here one time for the surgery. Followups are also done virtually.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I was looking at the head reduction surgeries, in particular occipital reduction. I just have one question left before I want to arrange a consultation
My question is, in general how much head circumference reduction can you expect. You posted that the average reduction in the back is around 7 milimeters. So does a 7 milimeter reduction in the occipital area result in a 7 milimeter head circumference reduction aswell or is it different? Is it possible to calculate it? I know its a hard question to answer but if you could give me an average estimate of the head circumference reduction that happens after the occipital reduction from previous patients. I sent a picture so you can look at it as well.
Thank you for your time
A:That is a very good question to which there is no exacting answer since the reduction in bone projection does not correlate with reduction in circumferential measurement in a linear manner. I am certain there is a mathematical way to answer this question based on spherical geometry but that is beyond my expertise. Rather than circumferential measurements I focus on what aesthetic effect will be achieved in profile projection which is a lot easier to see. Certainly the red line you have drawn in your photo is beyond what 6 to 7mms of bone reduction would achieve.
Dr. Barry Eppley
World-Renowned Plastic Surgeon