Your Questions
Your Questions
Q: Dr. Eppley, My major concern unfortunately, is in the anterior temporal muscle area, but also the bony part ABOVE it. My hairline was straight and low a couple of years ago, but now, i have the typical M shape, because it is now recedded at and above the temples.
Even if you cauterize the anterior temporal muscle, i thing it is also the bone that makes my forehead soo wide ( the part above the muslce as well)
From the side view, my forehead is also almost straight instead of sloped towards the back. Is there anything that could be done?
A: You are referring to reduction of the bony temporal line at the sides of the forehead which is commonly done as part of bony forehead reductions or even as a stand alone procedure. (with or without anterior temporal muscle reduction)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have left deltoid atrophy due to brachial plexus injury long time ago. I m looking for deltoid implant or fat grafting to make left shoulder thick like right shoulder. Now I m 53 year old guy.I m also sending you one picture of patient who had this type of surgery.plz give me the cost and good advice. Thanks
A: There are advantages and disadvantages to both injectable fat grafting and implants for your deltoid deformity….and not to be confusing there is even a third option. (dermal-fat graft which is sort of a cross betwween the two being a solid fat graft much like an implant) The key determinant in your case is that your left shoulder is very scarred from prior injuiry/surgery. This makes it not great for injectable fat grafting. With all of the scars on the shoulder this makes it more ideal for either an implant or a large dermal-fat graft. And those two options are worthy of a more indepth discussion.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have some questions about the custom jawline wrap.
1) I see that you’ve noted the typical maximum horizontal lengthening is around 10-12mm for an implant, if I have an indwelling chin implant, can it be assumed the 10-12mm can be added onto whatever implant I have now?
2) Adding on to the 1st question, can a custom jawline wrap add in the range of 14-16mm in horizontal lengthening with the presence of an indwelling implant?
3) If it is possible, does such a big horizontal lengthening effect how much gonial width can be added, because the skin will already be stretched too much?
Thanks
A: In answer to your custom jawline implant questions:
1 and 2) While you may get up to 50% more chin projection by a secondary implant augmentation it will not be a 100% increase as the soft tissues can not tolerate that implant load. If you need that much chin projection increase it should be converted to a sliding genioplasty.
3) Whatever is done at the chin does not impact what can be done at the jaw angles in terms of soft tissue stretch.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I saw your website and send this message to know about your head size reduction surgery. I have quite big head. Circumferences is about 60cm, and overall size of my face and head looks large and big. my heigh is about 170cm So it looks more weird then others. I want to have under 58cm circumstances. Is it possible? I heard there is surgery of botox for temprolis muscle which can make my head smaller. Can I get both of this way? and after surgery is there any issues on Durability of my skull?
A: Temporal reduction can usually reduce the circumferential head measurements by 2cms. It has no negative effect on durability of the skull.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I read your post about rib shaving surgery (https://exploreplasticsurgery.com/case-study-subcostal-ribcage-protrusion-correction/). However when trying to do research online I cannot find any doctors who do this kind of surgery. I have a cartilage protrusion at the connection of my 3rd rib with the sternum, as well as my second rib protruding outwards greatly after an injury.
I was wondering if you perform this kind of surgery and if you also know of any other doctors that perform this kind of surgery as well. Why is this surgery not more widespread for cartilage protrusions?
A: I have removed hundreds of ribs for aesthetic purposes and may be one of the few, if only, surgeon in the world that does so. But, quite frankly, I can’t imagine the incision and resultant scar to shave down your upper chest rib protrusion (costochondral junction of rib #3) would be a good aesthetic tradeoff… small as that incision may be. So the question is not whether it can be done but whether a small scar in a highly visible location would be viewed as a less noticeable aesthetic problem.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am looking for bivalve testicular enlargement due to testicular atrophy from steroid use years ago.
A: I assume when you say ‘bivalve’ testicle implant you are referring to a wraparound or hollow chamber implant. Whether that is appropriate for your testicular atrophy depends on the current size of your testicles. The cut off between the wrap around technique and the side by side or displacement technique is 3.5cms in my experience. If the testicles are 3.5cms or smaller than much larger testicle implants will displace them out of the way sufficiently and is the better testicular enlargement method. Such small testicles have a high slippage rate out of the implants. With 3.5cm or larger testicle size the wrap around implant is the better method to avoid a ‘4 ball’ look.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have some questions about my upcoming surgery:
Q1) I am really unfit / mostly sedentary living, then would being under general anesthetic be a risk for me?
Q2) if I decide to go ahead with the buccal fat removal, can the fat extracted be placed where the orbital region is below the eye?
Q3) could having genioplasty combined with a Buccinator myectomy improve the outcome of less rounded cheeks?
A: In answer to your facial plastic surgery questions:
1) I am not aware that being unfit increases general anesthetic risks.
2) The buccal fat can be recycled and relocated to a facial site of the patient’s choice.
3) A sliding genioplasty always improves the appearance of the rounded face.
Q1) I am really unfit / mostly sedentary living, then would being under general anaesthetic be a risk for me?
Q2) if I decide to go ahead with the buccal fat removal, can the fat extracted be placed where the orbital region is below the eye?
Q3) could having a sliding genioplasty combined with a Buccinator myectomy improve the outcome of less rounded cheeks?
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can you still perform chin and jaw augmentation with coral hydroxyapatite implants ? If yes do you have some before and after pictures on male patients that had this procedure done ? What is the price ? I’m prone to autoimmune issues so i can’t use regular implants.
A: As a general statement HA granules are a very poor method of chin and jaw augmentation….unless the amount of augmentation is very small and localized. (which has not been my experience with most male patients that seek jaw augmentation) The results often are uneven/irregular and extremely modest in its aesthetic effects. Normally I would never consider using it because of these issues. It is very biologically appealing but aesthetically unappealing.
However I can understand why you ask given your autoimmune concerns…which means this is your only onlay jaw augmentation option. (obviously fillers remain a non-surgical option) The question from my standpoint is not whether they can be used but their cost. To do chin and jaw augmentation of any significance you would need 8 to 10cc (syringes) of material and would have to accept that it would need to be placed in a non-linear fashion. (meaning on the chin and jaw angles but don’t try to connect the three areas)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am struggling with plagiocephaly, to be more specific, one side of my face is significantly protruding, which affects almost every aspect that would be responsible for the symmetry of my face, it is rather complex, since it is causing a correlation of many smaller problems that lead to assymetry not only in my eyes, but also nose, forehead, jaw, cheek bones, temple region, eye socket. Is there a possibility to harmonize my face by implants or bone, skin removal, autologous fat injection?
I went through bimaxillary osteotomy surgery already, but since the doc focused on functionality rather than aesthetics, i am satisfied with the side profile, but definetly not with frontal symmetry, it is hard to compare for me but i have the feeling this surgery worsened my frontal symmetry even more….
A: Plagiocephaly is well known to affect the face with protrusive asymmetries on the ipsilateral side. Like all facial asymmetries the critical question is which side of the face is preferred regardless of the pathology behind the differences. Also it is important to recognize that augmentation improvements usually produce more substantial changes that reductive procedures.
That being said the most meaningful piece of information beside your pictures is a 3D CT scan in the treatment planning process.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi there, I had some issues with my facial asymmetries especially in my jaw. I am a university student in my second year, and am 19 years old. I started to notice it about a year ago where I started to take pictures using the back camera which accentuated the asymmetrical jaw in picture and I grew more insecure because of it. I wanted to simply consult and ask of the severity and if there would be anything I could do as a young man in my final developing stage before it’s fixated and permanent. Would you recommend any types of exercises or medications prior to resorting to plastic surgery? I would highly appreciate an honest assessment and advice.
A: Bony jaw asymmetry can only be improved by surgery not exercises. Whether that would be by orthognathic surgery or onlay implant augmentation requires a 3D CT scan to evaluate.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, have a very wide mouth and I was wondering if Commissuroplasty procedure could be performed to reduce the width of my mouth ?
How bad are the scars from the procedure?Can the scars be hidden ? Does the procedure come with complications? Will there be a need for scar revision?
A: Changing the width of the mouth does require incisions and resultant scars at the mouth corners. Such scarring is the major determinant of whether one should undergo the procedure. Unlike mouth widening (Y-V technique), where the scar lines remain at the vermilion-cutaneous junction, in mouth narrowing (V-Y technique) there is a scar line that trails away from the mouth corner from its original location more lateral location to the new more medial location. Short of the need for reconstruction of traumatic injuries or a congenital deformity I can endorse the mouth narrowing operation as an aesthetic procedure….the visible scar line is not a good tradeoff.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a few questions about testicular implants.
You mention that the wrap around implants are about 70% wide as they are long. I’m curious if that ratio could be changed if someone wants a rounder implant.
You also mention that the largest wrap around implants you have placed were 7.5cm. What if I wanted to go larger than that?
A: In answer to your testicle implant questions:
1) They are custom made so the ratio of length to width can be altered to whatever the patient wants.
2) 7.5cm testicle implants are an extremely large implant that has 130cc volume…which means a pair equals over 250ccs volume. It would be hard to imagine anything larger could even fit in any one. I am happy to do what the patient wants, my only concern is will it work or fit.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in skull and face reshaping surgery. I’m not happy with my head being too wide and having a bump on my left side. My head is also flat at the back. Thus, I am interested in having temporal muscle reduction surgery ( bilateral ) and augmentation of the back of my head with hydroxyapatite. I would also like more masculine and prominent forehead bone and would like to have augmentation with hydroxyapatite there as well. I have read that Dr. Eppley recommends implants in many cases, but I’m more interested in hydroxyapatite. However, it would be good to know the difference in price between implants and hydroxyapatite in my case?
A: The combination of side of the head narrowing (temporal reduction) with back of the head augmentation is a good one to achieve the head shape change you are seeking. However the use of hydroxyapatite bone cement for any form skull augmentation would be the worst way to do it. Besides the large scalp scar that is needed to provide the working space for such bone cements it costs would easily be 2x to 3X that of custom skull implants and would only achieve 1/3 of the augmentation result. Everyone overlooks that such bone cements were only ever made to fill in skull defects and where never intended to be used for aesthetic onlay augmentations, thus their poor ability to do so. While their biology has understandable appeal their aesthetic effects do not remotely match it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have some questions about custom facial implants:
- Can the material used for them potentially cause cancer?
- Can they be rejected?
- How often do patients get revisions iof they are unhappy?
- I have had foot surgery with plates and screws. Do them being there make it more likely to cause infection for custom facial implants?
- Can I get an MRI if screws are used to secure the implants to the bone?
- Which is better for facial augmentation, fat injections or implants?
A: In answer to your custom facial implant questions:
1) Custom facial implants and the materials from which they can be made do not cause cancer.
2) They also do not result in rejection. You are confusing rejection with the risk of infection, which does exist, and occurs. in 1% to 2% of such surgeries.
3) Custom facial implants have a revision rate of 20% top 30%, primarily for aesthetic reasons.
4) I am not aware that implants in one location of the body increase the risks of implant placement in any other location of the body.
5) Facial hardware is composed or titanium, a non-ferromagentic meta that is MRI compatible.
6) Fat injections create non-defined volume augmentation while implants create more defined and controlled facial augmentation changes. Both have their role in aesthetic facial augmentation, which is better depends on what facial changes the patient is desiring to achieve.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi. My question is can I have my butt crack shortened? If so how would it be done? It’s way too long to me. I squat exercising and it always shows. I want to be able to workout without a shirt on or go to the beach and feel comfortable swimming and not worry about my crack showing. Can you all help?
A: Can the intergluteal cleft be vertically shortened….yes it can. But I would doubt whether the resultant scar to do so may be viewed as a good aesthetic tradeoff.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I recently had a facelift and lip lift for overall skin laxity in aging, but I also asked my surgeon to try to correct some asymmetry I’ve experienced as a result of having Bell’s Palsy. Unfortunately, I was disappointed in the results. In some ways, it’s even worse now. Is there anything you can do in a case like mine? I don’t have faith that he can fix it, and he’s not even sure he can. Two photos attached. Thank you.
A: While you did not say what specific asymmetric facial features you see as the most bothersome nor which side of your face you prefer, I will have to make those two assumptions based on what I see in the two static non-smiling pictures you have sent. I see nose and lip asymmetries with the left nostril/nasolabial fold contracted upwards as well as the left mouth corner tilted higher than that of the right.
These are two central facial asymmetry features that could never be improved by a facelift and, as you have pointed out, actually are a bit more apparent postop which is not surprising. Facelifts are great for many sagging lateral facial tissues but can not improve any central facial issues.
For the nasal asymmetry I would recommend a release of the left labii superior nasalis muscle which is contracted and pulling up on the left nostril. (which. creates the snarl look) At the same time I would lower the left nostril which has also been pulled up for the same reason.
For the mouth corner asymmetry it is difficult to successfully lower the higher left side. A more effective strategy is to raise the right mouth corner to better match the left side. It is always better anyway to have a bit of an upturned mouth corner than an even or downturned one anyway.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I am interested in getting shoulder narrowing surgery and wanted to know if you are aware of and prepare for any complications that may arise in patients with hypermobile Ehlers-Danlos syndrome. Or would you be against performing surgery on hypermobile patients? Just wanted to know your thoughts on this.
A: I think the question is whether Ehlers-Danlos Syndrome affects bone and its capability to heal if exposed to trauma. My research takes me to a 2017 study which evaiuated the bone structure in EDS patients and came to this study conclusion:
‘This study has identified a tendency of EDS patients to fracture, have low bone mass and abnormal bone structure. The aetiology is likely to be multifactorial, with an inherited structural element, accentuated by immobility or reduced exercise.’
This would indicate that performing elective shoulder narrowing surgery in EDS patients definitely has increased risk over non-EDS patients….and certainly could not be recommended.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, when nis the best time to undergo a chin implant revision?
1) Since I want to change the implant as soon as possible, what is the ideal time to do a new operation at a clinical level? Would you wait 6 months to place the new, smaller implant to stabilize the tissues or should you do it sooner also to avoid greater enlargement of the tissues?
2) The first implant was positioned by making an internal access from the mouth, should the second revision surgery always be done from the inside or, to avoid traumatizing the same tissues for the second time, is it better to do it externally under the chin?
A: In answer to your questions:
1) The earliest one should do a revision is 3 months to give the tissues adequate time to heal before re-injury. It would probably take that long as this point to have the new chin implant made.
2) While going external from under the chin (submental approach) has the least risk of infection and secondary wound breakdown that approach may not be possible based on where the screws are in the implant. Since the implant was pit in intraorally the direction of screw placement may make it impossible to remove the implant from below. That information remains to be obtained.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Shaved head, Can anything still be done to reduce my brow bone or minimize how noticeable it is
A: In the shaved head male there are more direct brow bone reduction options such as a limited mid-forehead wrinkle line incisional access. Whether that would be beneficial for you would require an assessment of pictured of your forehead.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, am in the early stages of considering a skull reshaping implant and at this stage simply gathering information to help me make a decision further down the line. I would be extremely grateful if you could spare the time to answer a few questions regarding this procedure.
1. What is your preferred material for skull implants as I understand there are several materials available?
2. I understand that titanium screws used to fix the implant in place will eventually start to corrode and need to be replaced after 20 years. Is this an easy-to-do process?
3. Is there an alternative to using titanium?
4. Can corrosion from titanium screws cause any health problems or damage to the brain.
5. Is there an alternative to using screws to secure the implant as the very thought of having screws placed into my skull terrifies me.
6. Is there any chance of damage to nerve or muscles in the scalp / neck.
7. Will the outer edge of the implant or screws be visible through the scalp, even with a shaved head.
8. Is there any chance of mis-measurement and ending up with an implant that doesn’t fit properly.
9. Are there any activities that I won’t be able to do again once the implant is fitted.
I look forward to hearing from you.
A: In answer to your skull implant questions:
1) The far superior material for aesthetic onlay skull implants is solid silicone.
2) Titanium screws do not corrode or ever need to be replaced.
3) The alternative is no fixation at all.
4) There is no corrosion from titanium metal. You are confusing a pure titanium metal with stainless steel which is an alloy.
5) Then don’t use them.
6) No
7) Implant edge visibility in the shaved head is always a potential aesthetic concern but is usualluy avoided.
8) No
9) There are no postoperative physical activity restrictions once fully healed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I’m wondering what is the material of your implant?
A: Custom facial implants can be made of either solid silicone, Medpor, PEEK, or titanium. It is the patient’s choice. With each material choice comes different costs, lengths of the incision and whether it can be placed as a one piece or multi-segment implant. Most patients choose silicone because of its superior handling properties and lower cost.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m looking to get a large square chin implant. Wondering if you do custom chin implants?
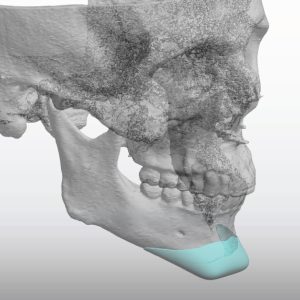
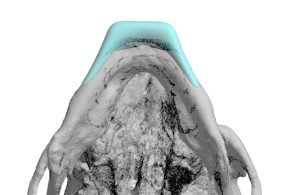 A: You have correctly surmised that the only way to get a really good square chin implant design is to have it custom made. The standard so called square chin implants are not well designed and lack the necessary shape to create a good square chin appearance, instead they just make it look wider. I have designed and placed many custom square chin implants. (see attached example)
A: You have correctly surmised that the only way to get a really good square chin implant design is to have it custom made. The standard so called square chin implants are not well designed and lack the necessary shape to create a good square chin appearance, instead they just make it look wider. I have designed and placed many custom square chin implants. (see attached example)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, can clavicle lengthening be repeated twice?
A: Theoretically it can…but that remains a theory since it has never been yet done. There is no question that it can technically be repeated. I would have concerns, however, that it might not heal as successfully as the first.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My initial V line surgery was done over six months ago. The surgery has left me in a similar place as one of your patients in the gallery. She also suffered from an over done Asian V line surgery.
One of the side effects of having so much taken off is that my bottom lip comes up a lot more than it used to. It complicates many things and is still numb in the center. It looks like I am having, or had, a stroke when I talk or smile now.
That as well as the obvious asymmetry that was already there. My hypothesis is that the asymmetry is from continued pressure supporting my face whilst reading over many years combined with an anxious habit of clenching my teeth, though I am certainly no doctor.
A: Thank you for sending all of your pictures and x-rays after V line surgery. I must say that the V line surgery you had is the most aggressive jaw bone removal that I have ever seen. To call it an overdone V line surgery is an understatement…and I have seen many. While I could have a discussion about how that was the wrong type of V line surgery for you with a natural high jaw angles (which is why the bone cut was so steep and severe) that issue is irrelevant now. Your surgeon should have known better, that was poor judgment on them.
You have correctly surmised that restoration of some of your jawline can only be done by a custom implant design to re-establish some inferior border length from the chin back to the jaw angles bilaterally.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Below are screenshots from a series I did using Facetune. I was able to adjust the skull to what i’d like to potentially achieve… but I am guessing that amount of augmentation is too much?
A: Thank you for sending all of your pictures and your own imaging. It is always hard to do such imaging when hair is present but I suspect your statement about your own imaging being too much is probably accurate….for a one stage skull augmentation. (but not for a 2 stage skull augmentation)
All skull augmentations are limited by how much the scalp can stretch at one time to accommodate an implant placed beneath it. A one stage skull segment ration means the immediate insertion of an implant whose size depends on how much the scalp will stretch. (usually 150ccs or less) A two stage skull augmentation is when a tissue expander is initially placed to stretch the scalp out first to accommodate a secind stage where larger skull implants placed. (usually 200cc to 300cc volume)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I was wondering if fat grafting to the jawline to achieve wider jaw is a good procedure? Will the fat sag in the long term and cause jowls?
A: Fat grafting would not be structurally stable as a jaw augmentation method. As you have correctly surmised it will sag and create jowls…sooner rather than later.Of equal aesthetic importance it will only create jaw fullness, not jaw definition.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, A question for you. As I know he is well renowned about custom made implant. So iIneed entire midface augmentation But I also oneed ne eye moved forward a few milimetters because my right eye is set back more than the left.
My question is can you help moving my eye forward and at the same time using custom implant for complete midface augmentation?
A: Unless the eye is posteriorly placed due to an injury (in which it at one time had more forward projection) you can’t change the natural position of the eye into a more forward position. It is important to remember that the eye is attached by the optic nerve so pulling on it to try and move it forward risk potential vision loss. Moving an eye ur or down is one thing since it doesn’t cause optic nerve stretch/injury but pulling it forward has completely different concerns in that regard.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, In the last few days the swelling from my custom chin implant has decreased a bit and the chin has more normalized but it is still excessively vertically high because the implant is very large and I would like to reduce it above all in height with a revision, I would like to ask you:
1) Going back perhaps the best choice was to opt for a genioplasty but now I have an implant positioned and fixed with screws, having to reduce it, does it make sense to shave it with the bur rather than removing it and doing a genioplasty?
2) Is it possible to reduce the prosthesis by filing it without having to remove the implant from the chin? I think it would be less traumatic to the tissue and also easier to adjust with just the right amount of reduction to do.
3) For the revision, would you make a submental access instead of from inside the mouth as was done at the time of inserting the prosthesis in order not to traumatize the same tissues a second time?
A: The mistake that is often made is that surgeons think they can do adequate reduction/modification of an implant by an in situ technique. (leaving it in place) That may be successful for the most minor adjustments of it but that will never work in your case. That would definitely not be the way to do it. Unscrew it, remove it, do what modifications are needed and then immediately reimplant it. That is the only way to successfully do it.
I also might point out that this is PEEK material…an extremely tough material that does not respond easily to any modification of it. It is the least modifiable of all facial implant materials. It will take considerable work on the back table in surgery to make the needed changes. The challenge of that task should not be underestimated.
As an addendum if you look at three options you now have:
1) Replace with new PEEK chin implant with better design,
2) Replace with sliding genioplasty, or
3) modify the existing implant
Options #3 is actually the least favorable option from an aesthetic outcome standpoint….even if it seems the ‘simplest’.
The impact of surgical trauma relates to the re-opening of the incision which has to be done with all of them so that concern is really irrelevant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi! I have been looking at your work with skull implants. I have two boys ages 7 and 9, both have plagiocephaly. My younger boy had torticollis and it made his head misshapen I tried to talk to his doctor about a helmet when he was a baby but he said it would round out by itself, that didn’t happen. With my older boy he had a skull fracture happen right before his 1st birthday he didn’t have to have surgery but I always laid him on the opposite side of the fractured side and this caused a flat spot. I feel so much guilt and blame myself and really want to find a good plastic surgeon to place an implant to round their heads out. I fear so much that they will be bullied. As a mother I want what’s best for my children. I have so many questions I don’t even know where to start. Is skull reshaping dangerous? Should they wait until they are older to think about having an implant placed? I look forward to hearing back from you! Thank you in advance for your time!
A: Such skull reshaping surgery is not done until they are past puberty and not usually before 16 years of age.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have some questions about clavicle lengthening, my clavicles are not so short but they have a “v” shape and this bothers me, can the clavicle lengthening surgery make my clavicles straighter?
A: I believe when you say V-shaped clavicles that you are referring the pronounced s-shaped curve that they have. Clavicle lengthening can not make an appreciable change in that appearance.
Dr. Barry Eppley
World-Renowned Plastic Surgeon