Your Questions
Your Questions
Q: Dr. Eppley, I am interested in a custom skull implant for the flat back of my head.
1- does the filling made behind the head reveal my permanent and any discomfort in the future?
2- if I fall asleep, if I sleep on my back or lie on my back, does it pose any problems, is there any problem if I get hit on the head from behind?
A: A custom back of the head skull implant will feel just like bone and has none of the postoperative concerns to which you have described.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a male interested in getting a sliding genioplasty to advance my chin both horizontally and vertically, as well as making it wider. How stable is this procedure short and long term? Is there a chance for bone resorption or the need to do a second surgery due to the chin shifting/non union between the bones? Have you seen such cases? Or simply put, would the results I get after the procedure most likely stay for life without any further complications? Would love to know.
A: The one piece sliding genioplasty is a very stable procedure that is associated with minimal resorption (less than 5%) but that will vary with the degree of movement. But in general it is clinically irrelevant. However when you split the bone into two pieces to widen it you introduce an additional variable which leads to a higher potential for asymmetries and irregularities.
Non-union of a sliding genioplasty, while an item on the all-inclusive list of potential complications, is not a problem I have ever seen in the past 30 years with over 500 bony chin procedures performed. Nor would I expect it to since the chin is not a functionally loaded bone, it has only aesthetic significance.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I had cervical spine surgery via anterior approach about eight weeks ago. I had internal stitches and external Steri-Strips. I was allowed to use mederma and silicone scar sheets 4 weeks postop and I have been doing that. Do you have any recommendations as to what I can do for my scar? It is bumpy in some parts and depressed in the others. And dark. I massage it twice a day and use silicone scar sheets I tried to attach pictures, but I’m not sure if it worked or not. Thank you.
A: Such scars take 9 to 12 months to fully mature. Time and patience is what you need. If by 6 months it is not trending towards good aesthetic improvement then have a scar revision done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
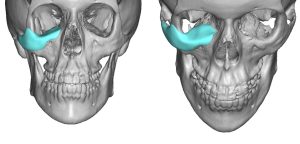
Q: Dr. Eppley, I am writing to inquire about the possibility of reversing a cheekbone reduction procedure that I underwent about a year ago. The procedure was called “high L osteotomy,” where a part of my cheekbone was removed and pushed in. However, I have been experiencing tightness around my cheeks since then and I am unhappy with the results. I am wondering if it is possible to reverse the procedure by doing reversal osteotomies and bone grafting.
A: The short answer is that it largely can be done. The long answer is that a L-shaped osteotomy is a little bit more challenging to reverse due to the pattern of the osteotomy (as opposed to the old style vertical oblique cut) but it can be successfully done. The posterior zygomatic arch part of the osteotomy can be as successfully reversed as the more significant anterior osteotomy but its main purpose is to allow the anterior segment to move it since it is not really important to try and reverse it. It would first require a 3D CT scan, or perhaps you have already had one done postop, to make a careful assessment of what was exactly done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve had a major accident that resulted in 4cm cut (about 0,5 cm deep) to my brow ridge (photos attached). After the accident stitches were put in for 7 days. The injury in question is approximately 19 days old at the time these images were taken. Can this be somehow improved surgically.
A: Scars will naturally start to turn very red within a few weeks after surgery which is a normal part of the healing process. How the scar will look when it matures (heals and the redness fades) and whether scar revision would be aesthetically beneficial is hard to project at this early time period after the injury. Usually good insight in that regard is known by 3 to 4 months, which is the time period you need to wait anyway to allow the tissues to heal to sustain another trauma. (scar revision) I suspect that scar revision will be desired based on how it looks now and given its prominent location.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a question about working out after getting implants. I’m 19 years old and if my bones were to get become bigger either from growing up to age 25 or working out then would the implants become smaller and cause problems? For example I got forehead implants and nasal implants my actual facial bone structure were to get bigger. Could the implants be designed to not become small if facial bones grow and become bigger or something like that? Thank you!
A: At age 19 your bones are not going to grow further to any significant degree nor will working out make them get any bigger either. Thus the concerns about any facial implant becoming too small later because of growth around is not a concern.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have had two wrap-around jawline implants and subsequent removal due to infection. The first one was in February 2022 and the second one was on April 3rd of this year. We also added medpore infra-orbiral/ midface implants this time. The jawline implant was removed last week because of infection. My midface implants are doing well.
At what month post-op should I take photos and initiate consultation for wrap-around jawline implant reinsertion and midface implant evaluation? At what month post-op is it recommended to do the jawline implant reinsertion? I’m still swollen and healing from my surgeries this April.
A: Placement of a 3rd jawline implant after 2 prior implants that were removed due to infection is not something I would do until 6 months after the latest implant removal.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 45 year old transsexual woman, 178cm and I wish to have the shoulder reduction and also rib removal surgery to have a more feminine waistline. I wanted to know if these surgeries can be combined together in a single surgery. I wanted to ask questions: – How long will I have to stay in your clinic? – how long will I have to stay in America for convalescence after the surgery and how long (after the surgery) will I be able to get on a plane to return home in Europe – I will have to face about 9 hours of travel by plane (plus another 3 hours by car to return to my city), after how much time will I be able to do it. – do you have hotels you can rely on to arrange surgeries for people coming (like me) from abroad?. – How long will I have to stay in America in general to be sure I don’t have complications before getting on a plane to Italy?. – What is the overall budget I will have to rely on during my stay in America?
A: Shoulder reduction and rib removal can be done during the same surgery.
The key to doing both is to properly prepare for the immediate recovery. It is most ideal to have someone with you as that will shorten your stay here and aid getting back home. (7 to 10 days minimum) If you do not have someone it is going to take longer until you are ready to go back home. (14 to 21 days)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, male and female ribs are typically slightly different in that the female thoracic cage inclines downwards whereas male thoracic cage is wide and short. Through surgery, would it be feasible in not only have ribs removed, but having the 10th and 9th rib cut in certain parts and through a corset forced to go downwards like seen in the anatomy attachment.
A: That is a theoretical possibility with the key of prolonged corseting.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am 27 trans-femme. When I was 23 and before I started transiting, I had a genioplasty (I believe 8mm), however this brought out the unevenness of my chin and created a step deformity. I am interested in feminizing my face by perhaps moving the genioplasty back a little, and resolving the step deformity so that my jaw/chine line is a smooth line.
A: Thank you for your inquiry and sending your pictures. Certainly setting back the chin can be done and usually to see enough of a difference the usual amount is 50% (4mms in your case) although that number can be any amount you so choose. (subtotal sliding genioplasty reversal) It would be helpful to see a simple panorex x-ray to determine what type of hardware was used in the original procedure. While bringing the chin back will help the notch deformity along the jawline it may not eliminate it 100%. So adding some bone chips to help fill it in can be helpful as well.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’ve had angular chelitis for over 10 years. Ointments don’t cure this terrible condition. The corners of my lips turned downward and now I started drooling. I have crusting, bleeding..I can barely eat, talk or have dental procedures done. Is that possible to have a surgical procedure I heard about to removed the diseased tissues? I went to see cosmetic surgeon today who recommended a lower face lift for $50.000.
A: Despite the many benefits of a lower facelift, improving angular cheiltis is not one of them. Angular cheilitis has to be treated directly with excision of the diseased tissue possibly combined with a corner of mouth lift. It is possible that if enough nasolabial fold tissue hands over the mouth corners that a lower facelift may have an adjunctive benefit with the mouth corner excison but I would need to see some pictures of your mouth area to make that determination.’
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I know that I have two extra ribs on the vertebrae above the typical highest ribs. I was curious if that disqualifies me from being a candidate of this procedure?
A: You are referring to the question of whether having a cervical rib and getting clavicle reduction would increase your risk of developing postoperative thoracic outlet syndrome. (getting a blood clot) That is an astute question and would be of concern. There is no way of knowing what that risk would be since the combination of having that surgery in someone with cervical ribs has never been done. But I think that risk is real and I would be apprehensive for an aesthetic surgery to take on that potential risk.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi! I’m considering infraorbital rim implants. Do I seem like a good candidate, would the procedure be able to fix my problem?
A: It would be very fair to say that you have major infraorbital rim skeletal deficiency for which implant augmentation can only help. But the magnitude of the deficiency requires a combination of vertical and horizontal rim augmentation as well as blending over into the anterior malar area. This requires a custom infraorbital implant approach.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I’m interested in receiving jaw implants to change the shape of my Gonial angle and to fix my TMJ. After checking out the website, it seems like this look could be achieved via vertical mandibular jaw implants? Additionally, is it possible to also fix my TMJ via jaw implants? Attached are pictures of me, as well as reference pictures of my desired Gonial angle shape. What do you recommend for me to achieve my desired look?
A:What you are demonstrating is a jaw angle that makes your mandibular plane angle flat or zero degrees. Yours is not all that far off from that now but some vertical length is still needed. Vertical lengthening jaw angle implants, which also add some width, would be the correct choice. While that creates the desired facial effect in the side and oblique views be aware that from the front view it will square out or increase lower facial width. In addition augmentation of the jaw angles will not fix your TMJ issues.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in getting larger pec implants than I had put in about 7 , 8 years ago here in NYC. I only have one in the right side, the left side developed fluid retention after surgery and had to be removed . Im interested in getting xxl larger implants. Questions: Do you work with larger size implants, how large do you think I can go safely and still get projection and a large lower chest…And, do you think I will experience the lymphedema on the left side again if I have another surgery? I understand there are better after surgery care for such co. Locations these days.
A:In answer to your XL pectoral implants questions:
1) It would be helpful to know what size pectoral implant is currently in your right chest. (I assume it is a standard one and its size must be ‘small’ since your left chest does not look that different than your right chest) That would go a long way in answering the question of how much more implant volume you can get.
2) Because of the size of your natural pectoral muscles to get a more profound effect the pocket would have to be expanded beyond the lateral pectoral line. (see attached) In mosgt men in normal size pectoral implants that line is never violated but in XL pectoral implants it has to be and is usually the look the patient is seeking.
3) What you undoubtably had was a seroma of the left pectoral implant which often only resolves by implant removal. (which you had done) Seromas are a bit of a biologic mystery as no one knows why they occur exactly. There are the body’s response to the separation of tissue planes (in this case the pectoralis major muscle from the rib cage) and the lymphatic fluid leak that naturally occurs when that is done. This usually resolves quickly when the two sides fall back together which the placement of an implant between the two sides delays that process. Usually the body heals the implant pocket by the formation of scar tissue (capsule) which is uneventful. But in some patients for reasons unknown, the capsule persistently leaks fluid and does not stop. (aka seroma) As you had the same procedure done on both sides of your chest…one got it and the other side did not…why that occurs is not known) What is known is that once it occurs in an implant pocket the risk is higher that it might occur again. This is not an after care issue, it is an internal pocket issue.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I have a flat head & need it corrected. Question. How much is it? how long safe is the procedure? How long is the procedure? How long is the healing time?
A:The term ‘flat head’ can mean different locations on the skull. For now I will assume it is a flat back of the head which is the most common flat head correct requested. Placing an implant on the outside of the skull is a perfectly safe procedure, just like placing an implant on the bone anywhere else on the face or body. Most custom skull implant surgeries takes 90 minutes to 2 hour to perform. Healing time usually refers to recovery which in aesthetic skull implants means swelling and how long does it take to resolve enough to walk around in public without being noticeable….7 to 10 days after the procedure.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello. I want to get shoulder lengthening, my right shoulder 2 cm smaller than right because of birth defection. However, exercising is very important to me. After surgery, I want to continue doing workout (mostly shoulder press, lateral raises, front raises nothing like other sports)How much months minimum I should wait to do those movements?
A: Currently I am not very enthusiastic about shoulder lengthening surgery. Between not being able to get more than about 15mms per side as well as the need to avoid shoulder exercises for six months after the surgery I don’t think would be a good procedure for you.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am making contact to inquiry about the Correction of Eye/Orbital Asymmetry, as you will see from the attached photos I have some degree of Eye/Eyebrow Asymmetry, So it be great if Dr. Eppley could review my photos and see if he could help with minimizing my Asymmetry. A case study that I think is simpler to my case is: https://exploreplasticsurgery.com/case-study-correction-of-eyeorbital-asymmetry-with-hydroxyapatite-cement/ I look forward to your response.
 A:In the treatment of vertical orbital dystopia (VOD) it rarely is so ‘simple’ as augmenting the orbital floor and rim and all turns out well. Having treated many VOD patients the lessons learned are that the entire orbital box and eyelids have developed around the eyeball where it sits. If you just raise the eyeball it will get buried underneath the upper eyelid and the eye will have increased scleral show inferiorly. (in other words the eyelids have to be adjusted as well) As you can see in the attached diagram all of your bony and soft tissue orbital structures are positioned lower. Thus a more comprehensive approach is needed to get a more effective result. Today VOD is usually treated with a custom orbito-malar implant (see attached) usually combined with upper and lower eyelid surgery and a right endoscopic browlift.
A:In the treatment of vertical orbital dystopia (VOD) it rarely is so ‘simple’ as augmenting the orbital floor and rim and all turns out well. Having treated many VOD patients the lessons learned are that the entire orbital box and eyelids have developed around the eyeball where it sits. If you just raise the eyeball it will get buried underneath the upper eyelid and the eye will have increased scleral show inferiorly. (in other words the eyelids have to be adjusted as well) As you can see in the attached diagram all of your bony and soft tissue orbital structures are positioned lower. Thus a more comprehensive approach is needed to get a more effective result. Today VOD is usually treated with a custom orbito-malar implant (see attached) usually combined with upper and lower eyelid surgery and a right endoscopic browlift.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I want symmetrical eyes as my right eye sits lower than my left. Can it be done and how?
A: You have an aesthetic VOD (vertical orbital dystopia). This means the entire orbital box and all the associated soft tissues (eyelids, eyebrows) have developed lower compared to the other side. Your VOD is about 5mms. To adequately treat VOD every component of it must be addressed from raising up the lower orbital rim-floor and cheek (custom orbital-cheek implant), raising the lower brow bone (transpalpebral inferior brow shave), endoscopic browlift and raising the upper and lower eyelids. You need the complete version of VOD which addresses all five components of the problem.
Can you achieve symmetrical eyes….no. You can significantly lessen the asymmetry to one that is much less noticeable.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, so basically I have a dent on the right side of my face and am looking for answers on if I can get worked on. I got the dent from a car accident, I had my right bone flap removed then put back in 2.5 months later. Sadly healed up with a dent and haven’t seen any doctors or surgeons for my head since the surgery.
A: You have the classic temporal muscle atrophy that comes from having had a temporal craniotomy from your accident. This soft tissue depression, which may be magnified by some temporal bone settling, can be built up using a variety of methods from injectable fat grafting, bone cements, to custom temporal implants. Each temporal reconstructive method has its advantages and disadvantages.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have jaw denting and sagging due to wisdom tooth removal. Can this be fixed? I have attached a picture of my impacted lower wisdom teeth which were removed.
A: While the picture of the x-ray is of poor quality I believe it shows the impacted state of the third molars…which would require some significant bone removal to remove these teeth. So it certainly seems plausible it could leave external indentations from the loss of bone along the jawline as well as some soft tissue sagging from the subperiosteal degloving of the overlying soft tissues.
My assumption would be that restoration would require fill of the indented bone areas with a possible jowl tuckup for the sagging.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can distraction osteogenesis be performed only on chin to increase the vertical length of the chin! It’s because i atleast need an inch of vertical growth in the chin! Can distraction osteogenesis be performed on chin for this purpose?
A: On a practical basis distraction of the chin has many technical problems the first of which is there are distraction devices available for this purpose. More pertinently if 20 to 25mms of vertical chin lengthening is needed a vertical lengthening bony genioplasty with an interpositional graft can be done up to 20mms, negating the need for a complex and lengthy distraction process.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I am interested in skull and face reshaping surgery. I’m not happy with my head being too wide and having a bump on my left side. My head is also flat at the back. Thus, I am interested in having temporal muscle reduction surgery ( bilateral ) and augmentation of the back of my head with hydroxyapatite. I would also like more masculine and prominent forehead bone and would like to have augmentation with hydroxyapatite there as well. I have read that Dr. Eppley recommends implants in many cases, but I’m more interested in hydroxyapatite. However, it would be good to know the difference in price between implants and hydroxyapatite in my case?
A:I will not use hydroxyapatite cement (HAC) for any form of significant skull augmentation…and augmenting the back of the head and the forehead-brow bone qualifies as significant skull augmentations. HAC is a terrible way to try and do skull augmentation. The incisions needed to use it properly are big, it is very expensive, the amount of augmentation is very limited and there is poor control of its shape. The biologic appeal of HAC is great but its clinical application for onlay augmentation is poor. It was never made for skull augmentation, it was made to fill skull defects which is a very different geometric problem. Implants may be implants but their aesthetic results are so superior and the ability to place them through small scalp incisions makes their lack of biologic appeal an acceptable tradeoff.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I want to see what I’d look like with potential surgeries. I struggle with facial asymmetry, there’s not really a major area that’s bad it’s more like several minor ones on one side which make it look worse altogether. The eye region, cheek bone / jaw line region and one ear from a botched Otoplasty are the most noticeable to my eye.
A: Short of the ear asymmetry (do you bring the overcorrected left ear back out, reduce the more prominent right ear or some combination of both) I would not recommend any facial surgeries for you. Yes there are some minor facial asymmetries that exist but in an effort to improve them you are just as likely to cause other issues that require more surgeries to fix etc….this is known as going down the surgical rabbit hole. i would consider yourself extremely fortunate that you have as good a facial structure/shape as you have with an overall very handsome face. Most men would love to have your face and I have operated on many such patients who never even get close to where you are despite the best surgical efforts.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can anything done for the left cheek was fractured long ago. Looking for a more sculpted symmetry look. What are the options for this?
A: For the left cheek asymmetry from the original fracture better improvement will come from implant augmentation as opposed to now trying refracturing the bone and repositioning it. This is best done with a custom implant approach using a 3D CT scan to match the left asymmetric side to the normal right side.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in getting chin ptosis correction. I am very insecure about my chin especially when I smile, it seems to get bigger. I’ve seen that you have a lot of experience correcting this type of chin, so I am very interested in scheduling an appointment at your place.
I would like to know how you would correct this. I would like to have no sagging, but without changing the length and width of my chin. I would like to have my jaw and chin to form a straight line, both from profile and front view (for reference, I like Ariana grandes lower jaw and chin :D)
I thought about getting fillers in my jaw, and I want my chin to fit. I don’t want the v-line look, I want a more U/line look, I don’t want my chin to be too pointy.
A: The only effective treatment for chin ptosis is a submental technique which works by removing some of the inferior/overhanging soft tissue chin pad. By definition that also removes some chin length from the soft tissue reduction and may or may not make the chin a bit wider. In your case this work have to be combined with some submental/neck liposuction to get a better chin-neck profile relationship.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a chronic migraine sufferer. I am 30-years old and have tried all kinds of pills, nasal sprays, powders, self-injectables, and tablets for my migraines. I specifically get pain in the frontal area. I do believe that the trigger point is either the frontal or nasal. The pain is behind the eyeballs, on the eyebrows, and the forehead. I am aware that insurance doesn’t cover surgery, although it does in my state of where I reside. It is called Nerve Decompression surgery. I do have some questions from Dr. Eppley if possible:
- Specific treatment for this involves decompressing the supraorbital AND supratrochlear nerves in the glabellar area by resecting the corrugator and depressor supercilia muscles using a minimally invasive endoscopic approach similar to that used for a cosmetic forehead lift. Supraorbital and supratrochlear nerves are decompressed……..
Your website states that a brow bone reduction could help this. I think I am only a candidate for Type 1. Do you believe that shaving the bone could help decompress the nerves? (incision would be via frontal hairline)
- Can you combine this with a slight orbital rim shave?
- Have any of your patients with frontal pain who had surgery had any success? Are they completely migraine free or reduced?
- Dr. Bahman Guyuron started doing forehead lifts/brow lifts and many of his patients had little to no migraines. He also founded the migraine surgery society.
I know this sounds crazy but I do believe this pain comes from the anatomy of my bone structure. I do have masculine features.
A :Thank you for your inquiry and sending your imaging to which I can say:
1) You have very wide open orbits and an exit of the supraorbital nerves that shows no inferior bony containment at the medial inferior supraorbital rim. Thus specific bony decompression of the supraorbital nerve does not seem to be needed as there is no obvious bony constriction of the nerve)
2) You have a perfectly straight septum with no inferior turbinate impingement on it, thus I see no evidence for a nasal basis for your migraines.
3) This brings it back to whether standard release of the supraorbital nerves with muscle resection would be of benefit. No matter what is written about the success rate of the procedure all patients must know that it is unpredictable. While many patients get relief some do not. (In the short term everyone does because of the nerve numbness) It would be fair to say that improvement means a reduction in their symptoms. Do some patients become completely symptom free…rarely.
4) The two methods to perform supraorbital nerve decompression and muscle release is either through a superior endoscopic technique or through an inferior upper eyelid approach. Each method has its advantages and disadvantages. Because you don’t need bone removed below the supraorbital foramen this makes the endoscopic technique a viable options.
5) Shaving the orbital rims for their aesthetic benefits has to be done through a frontal hairline incision not an endoscopic technique.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I just wanted to ask how long it would be before I could be active after the surgery. I ride horses and would want to get back to it asap. Is there anyway the surgery could affect my posture. Would all my organs still be fully protected if I had a fall? Are there any long term risks?
A: In rib removal recovery, there are no specific postoperative restrictions since you can hurt the surgery site. It is more about discomfort and the recovery from it. You should be able to ride horses again one month or so after the surgery.
The surgery does not affect your posture, there is no loss of organ protection and there are no long term adverse effects.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I want to get masseter muscle botox (Xeomin) as well as botox in the Crows feet area around the eyes from my dermatologist, would this be an issue with the implants I have? What would happen if the doctor accidentally injected into the cheek, jaw, temporal, or chin implant? Could it leak or get infected?
A:That should not be a problem. The key is let the dermatologist know there are implants there. In the eye area injections are done right under the skin which is well away from the implant. In the jaw angle area they have to go deeper to get into the muscle, they just don’t want to go down into the implant. But having the implant there actually makes the muscle easier to inject since it is pushed out.
Your implants can not leak since they are solid, not gel-filled like breast implants.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Would you be open to performing a bony genioplasty for vertical lengthening? It is my preferred option vs an implant. Also can a genioplasty add width and squareness?
A:A vertical lengthening genioplasty is a good choice for dropping the chin down and allows for much greater amounts of lengthening if needed. However it can not make the chin wider or more square since it takes the natural chin and moves it down. It will essentially be the same chin width and shape. It would take an implant to add to it to do so.
Dr. Barry Eppley
World-Renowned Plastic Surgeon