Your Questions
Your Questions
Q: Dr. Eppley, What is the projection angle of iliac crest in reference to the spine? Would you say 45 degrees? The reason for my question is that I am trying to understand how much the iliac implant will add lateral prominence and height to the pelvic bones. Will the implant narrow the gap between the iliac crest and rib cage?
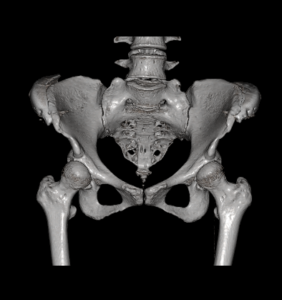 A: 45 degrees would be accurate assessment of the angulation of iliac crest implants on the bone.(see attached 3D CT scan) At a 45 degree angulation it would be fair to say that it would reduce the vertical distance between the new crest position and the 12th rib.
A: 45 degrees would be accurate assessment of the angulation of iliac crest implants on the bone.(see attached 3D CT scan) At a 45 degree angulation it would be fair to say that it would reduce the vertical distance between the new crest position and the 12th rib.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I considered getting custom silicone jawline implant but in the end I got the medpor implants in my home country. I got RZ mandibular angle 11mm, and RZ extended square chin implant (5mm) The op took place 7 mounths ago. The implants were fixated with titanium screws. Choose of the implants was meant do get so caled “wraparound” or “matrix” effect.
The operation went succesful exept one thing – propably due to the natural assymetry of the lower part of my face, or wrong placement done by the surgeon – I endend up with crooked chin, more specific, the left side of my lower face is somehow more portruded than the right side, it’s seems too rounded, which causes the left jaw implant look so out of place, so unnatural, like a result or swelling, while the right side creates a natural looking straight line. As I said I don’t know the exact cause of this result, the implant either shifted or it’s the left wing of an Implant, which causes too much projection, but I pressume the reason behind this is the lack of implant customization before inserting it, and it made my face look even more assymetrical than before. I’m writing this because you have had many experiences with medpor implant removal, and I wanted to ask a few questions about possible correction:
1) Can a medpor implant be safely trimmed through the intraoral/skin incision or does it have to be removed, trimmed and inserted again? Is it a saw or scalpel to be used to shave it down?
2) – If my case requires implant removal/replacement – Because of long size of the chin implant wings, my chin implant lays partially over mandibular implants, as the wings reach the jaw angles. Are these three implants became commecected due to the tissue ingrowth? And If they did, could future chin implant correction or removal be dangerous to jaw angle implants?
3) After one side of an implant is shaved down, weather 2 or 3mm, or completely, could it somehow cause the middle and right side to shift, due to lack of balance?
4) If chirurgical intervention were too risky, could it be treated with HA dermal fillers to achieve facial symmetry?
Best regards and thank you in advance for your answers
A: When using standard implants to create a total jawline augmentation effect the question is not whether there will be asymmetry, as there always will be, but how significant will it be and how will it needed to be treated.
In answer to your questions:
1) Medpor implants will need to be removed, modified and reinserted.
2) The jaw angle implant can be removed despite the wing of the chin implant overlying it.
3) No.
4) Injectable fillers can always be used to help with the asymmetry of any paired set of facial implants.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is it possible to add bone to the orbital rim, with something like hydroxyapatite? I’m talking about the upper orbital rim, rather than something like infraorbital rim implants.
A: Hydroxapatite, a synthetic ceramic material and not bone, can certainly be added to the brow bones or superior orbital rims…but it would require a full coronal scalp incision to do so. This is why brow bone implants, which can be done through a small scalp incision using an endoscopic technique, is usually preferred.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 24 year old male with a vertical lengthening chin implant (size medium). Unfortunately, I have visible ridges from the implant and I still desire more vertical augmentation. I had a few questions about genioplasty and scheduling surgery.
1. Does Eppley still perform vertical lengthening genioplasty of 10-14mms?
2. Does Eppley prefer to use iliac crest or cadaver bone for vertical lengthening genioplasty? How much do these grafting options tend to add on to cost?
3. Can the chin be widened during genioplasty? Not changing the shape of the chin, but widening the natural chin.
A: In answer to your vertical chin lengthening questions:
- I have done vertical chin lengthening osteotomies up to 20mms.
- While one’s own one can be used as the interpositional graft most patients opt for the cadaveric corticocancellous block graft.
- While chin widening osteotomies can be done, doing so at the same time as a significant vertical lengthening procedure is not recommended. This create unstable bone segments that are hard to fixate.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My goals are distal brow enhancement, eye socket depth is a little shallow, so eyeballs bulge out a little on distal end of eye socket, so need distal brow augmentation for eye protection during sports, etc.
PD is only 59mm, so cannot add too much jaw width augmentation or will lose aesthetic balance. Cheek augmentation to ameliorate volume loss. Have perio disease under control via perio care, but 33% bone loss in upper & lower jaw. does Dr. think chin needs profile enhancement?
A: Thank you for the clarifications to which I can say:
- Tail of the brow bone can be augmented with an implant accessing it through upper eyelid incisions.
- In treating volume loss in the cheeks an implant approach must focus on the malar-submalar region.
- What matters most in any facial reshapong change is what the patient thinks about the potential change. This is where the role of computer imaging has great value.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, is alar base lowering on one side a possibility? My left nostril is fine, but my right nostril shows a lot.
A: While nostril lowering can be done that will affect the base of the nose primarily…..it may not necessarily decrease nostril show which is more of an issue with the alar rim above it. Your imaging suggests that the combination of nostril lowering and an alar rim graft is needed to achieve the complete effect of improved nostril symmetry.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can I get an existing chin implant removed and genioplasty done in the same procedure? Or do I need to wait in between? My previous surgeon told me I need to wait if I ever want to replace my implant with a different size.
A: Whether you are replacing a chin implant with a different implant or converting it to a sliding genioplasty, those procedures are done at the same time. There is no advantage to making implant removal and its replacement as separate procedures.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a large depressed scar on my right cheek from acne. I have a smaller one on my left cheek. Two plastic surgeons have tried fillers over 2 decades ago with minimal improvement. The second surgeon, who thought injecting Restalyn deeper would work better, showed me the fluid coming out of pores as he was injecting it.
Would you please advise whether or not cheek implants might work? I’d love to get back to not feeling self-conscious when my wife and I are at church or in other public settings.
A: Your question is based on the premise that the contour of a soft tissue deficiency/scar can be improved by the push of an implant placed on the underlying bone. This approach is also suggested based on the failure of injectable fllers to make any difference. (although I am surprised that fat injections have never been proposed since this type of injectate is the most appropriate for such soft tissue deficiencies. Synthetic injectable fillers are too soft or ‘jello-like’ to work well in stiff scar)
Given where your depressed scar is located (submalatr region of the cheek) I would agree that this is a sound approach for contour improvement. It should probably be combined with a little injected fat externally as well for optimal improvement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Im interested in getting clavicle lengthening. Im 6’3 175 pounds (naturally slim. No health issues/drug problems etc) with very narrow shoulders.. way out of proportion for my height!
And the narrowness affects my posture and reach. Im pretty sure my shoulders are under developed due to smoking cigarretes during my teen years (14-18)
Wanted to know if 25-30mms of lengthening is possible on each clavicle from one procedure? And if not, is a second surgery down the line possible?
I attached some photos. Looking for some help and im hoping you guys can!!
A: That amount of clavicle lengthening is not possible per side. Unlike clavicle reductions, where 25 to 30mm reduction per side, the same can not be said fr clavicle lengthening. The physical constraints of the shoulder girdle simply do not permit it, 12 to 15mms per side is what is possible. And a second clavicle lengthening is not possible as that would be too risky through the same osteotomy site.
While I am bullish on clavicle reduction, my experience has taught me the opposite for clavicle lengthening.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi I hit my head 10 years ago, since then the swollen area never went away, I went for dozens of scans, they said that no focal abnormality was seen at the region of interest, there is no soft tissue mass, fluid collection or lymph node, I was told that my skull healed from the trauma by developing an excess of bone, can you guys help me to get this removed ? Is there a specific name for this excess bone growth that formed a swollen area similar to a bump shape on my forehead? Where do I get this shaved out or smoothened ? Please thanks.
A: Traumatic head injuries often result in small amounts oif subperiosteal bleeding which then turns into a calcification. This is very common particularly in the forehead area.. Such exostoses can be removed by shaving them down. Please send me a picture of its forehead location. This is usually approached from a hairline or just behind the hairline incision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a genioplasty with double jaw surgery, the problem is my face is now too long
I dont have the 1/3 – 1/3 – 1/3 facial proportion anymore, and my philtrum to chin ratio is off
Is there a way to reduce chin height and what would be appropriate for my case? Shaving down the chin or redoing a genioplasty?
I want to reduce the height beteen lower lip and chin.
A: Redoing the chin osteotomy would be the appropriate surgery. Whether it was done intentionally or accidentally the chin is now too long. When using step plates it is easy to inadvertently make the chin long while bringing it forward. The key question is how much vertical shortening is needed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Will having multiple sclerosis (MS) prevent me from having forehead horn reduction surgery?
A: Forehead horn reduction is a bone reduction procedure done by burring through an incision either at or just above the frontal hairline. I am not aware of any contraindicatons to doing the procedure with the diagnosis of MS….but that would require a better understanding of your stage and symptoms of MS.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m 23 yrs. old and I have plagiocephaly. How do you treat plagiocephaly?
The green arrow indicates that the right side of the skull is slightly advanced forward and the left side is slightly retracted at the back, and this is what is called plagiocephaly.
And I want to know what substance of this implant.
A: Most plagiocephaly surgeries are focused on augmenting the flat part of the back of the head with a custom designed solid silicone skull implant. Some patients either alone or in combination with augmenting the flat back of the head reduce the more prominent forehead side as well. It comes down to patient preference.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Pics are post chest wall reconstruction.Original PE repair 2008. Dr removed all the sterno costal junctions and elevated the sternum but ribs remained inward as the bar was on top of the ribs. Very bad. 2010 bar removed, 2011 mesh and seroma removed. 2023 chest wall recon with bone graphs.
Given the complexity, current surgeon will not place a Nuss bar to correct upper chest. My sternum is now stable but PE remains. I’m looking for solution to correct ribs 1,2 and lift upper sternum, OR last resort implant to correct the contour.
A: Given the complexity of your surgical sternal-rib cage deformity (multiple failed surgeries), a contour approach now seems the most likely to achieve improvement using a custom made implant from your 3D CT scan. I don’t see any autologous technique that I would be confident in that could provide assured and uncomplicated improvement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in the waist narrowing procedure via rib osteotomy. Does Dr. Eppley perform this surgery, of so how many has he performed?
A: I have done hundreds of rib removal surgeries but only a few rib osteotomies as the requests for rib fracture are far less than rib removal due to its more limited effects.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Will reducing the vertical chin height will automatically put the mentalis muscle higher? I Also have slight lip incompetance but i dont want any chin advancement, just height reduction so i dont know if it will help or no.
A: The superior origin of the mentalis muscle to the bone has a fixed position. So shortening the length of the chin bone will not automatically move the mentalis muscle higher or necessarily improve lower lip incompetence.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I‘m very insecure about my eyes, especially the eye distance because they are just too close to each other. My interpupillary distance right now is 61mm which is not the worst I guess, but with my relatively large face width which is around 142mm and also long mid face, it just looks weird. So my question is if there is/are any procedure/s which could make my interpupillary distance a few millimeters (like 3-4mm, at least 2mm) bigger? I’ve already heard of orbital box osteotomy, tho I believe the regular one is just for extreme cases, but is there maybe an easier modification of OBO to solve my problem? Or anything completely different? (like maybe moving the eyeball a bit within the eye socket (if that’s even possible) or making the eyes wider or just reduce the facial width and mid face)
I would be very happy to receive an experts opinion on this and thank you for your time already.
A: There are no ‘lesser’ orbital box osteotomy procedures. And for a 3 to 4mms change that is faf too extreme surgery. You will have to focus on changing facial areas below the eyes.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in a custom jawline implant and I have some questions:
- I am not from USA but from Israel. Is that a problem in getting the surgery.
- What is the cost of the surgery?
- How soon after the consultation can I have the surgery?
- Do you have a lot of experience in this type of surgery?
A: In answer to your jawline implant questions:
- My entire practice is patients who are not from where I am located. We have patients from all over the world, including Israel.
- My assistant will pass along the cost of the surgery to you.
- It takes a minimum of 3 to 4 months to go through the custom implant design process and it ready for surgery.
- Having performed over 500 custom jawline implants specifically I undoubtably have done more than anyone in the world.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am curious if there is a way to make my collarbones protrude more from my chest without affecting the width of my shoulders. I am female and do not want to masculinize my shoulders at all, I just want my clavicles to stick out more. I am thin and fit, but my natural bone structure doesn’t give me any projection in my collarbones. Are there implants or something available for this?
A: There are implants that can be made to wrap around the inner 2/3s of the clavicle to make them look thicker or more prominent. (clavicle augmentation) They are placed through a small incision in the supraclavicular fossa. This will not affect the width of the shoulders just the prominence of the clavicle or the amount of clavicle show.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
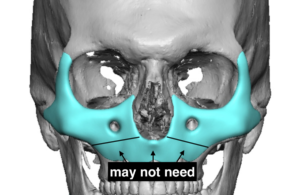
Q: Dr. Eppley, I had a LeFort I osteotomy to fix a recessed maxilla but it made the area above it recessed. Because of this, I’m interested in an extended custom midface implant for a LeFort III type augmentation, like the one in the picture attached, that I took from your blog (minus the area that the LeFort I fixed, obviously). If, down the road, I want an implant to augment my cheek-archs (like the one in the attached picture, that I also took from your blog), would it be possible to put them on top of the part that already has some of the extended custom midface implant? I know that it is possible to make a single implant for both areas, but I haven’t decided if I want to augment my cheek-archs. Thanks in advance.
 A: In answer to your questions:
A: In answer to your questions:
1) If you have had a successful LeFort I osteotomy you may only need to augment the rest of the midface that lies above it. (see diagram)
2) An arch onlay implant could be laid over the midface implant secondarily.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a big fan of your work and optimistic you’ll be able to help me out.
I recently had a custom jaw implant surgery on December 27th, 2022. I’m convinced the implant is the wrong shape completely, and that my doctor missed the mark on every aspect of it. Specifically, I believe it’s way too wide at the angles (nearly surpassing my cheekbones), the slope to the chin starts too far forward, the chin is too wide and bulbous.
My objective in getting the implant was create a jaw structure but with angularity. What I have currently is a jaw that is oversized in my opinion, washes out the natural definition of my face and cheekbones instead of bringing balance to them, and has created a wide body face instead of an angular one in harmony with my other features. I feel like a Leggo or charicature.
Below I have included the same photos I used as inspiration photos with my surgeon, as well as the 3D imaging of my jaw and the implant.
My surgeon is saying I’m still swollen, which I believe to an extent, but is essentially blaming the outcome on my “soft tissue and skin thickness and tightness”. I am 33 with normal skin tightness for someone of my age. I am also in decent shape. I’m 6 months in and when comparing my results to his other patients, I appear extremely swollen.
I’m desperate for a second opinion and some guidance, especially as my doctor has said many conflicting things over my experience working with him.
I look forward to hearing from you and having the opportunity to discuss this in greater detail live
A:Thank you for your inquiry and sending all of your information to which I can say the following:
1) At six months after surgery the result is what it is. No further improvements are going to be seen. For facial augmentation changes the results are 99% apparent by 3 months after the surgery. That is the time frame to judge the success of a custom facial implant.
2) When I see a design and lots of inspiration photos, but no patient photos, I automatically know this is a case of unrealistic expectations and/or unachievable goals. Implant designs are based are target images based on the patient’s own face not some ideal model face. That is not your face nor does it have your soft tissue composition. If your surgeon did not take your own pictures and do some computer imaging to determine what is and is not possible then the surgery never had a chance to be aesthetically successful. It was doomed from the beginning as implant designs are based on your facial imaging not what some model looks like. 99% of male patients are never going to achieve the inspiration photos you have shown, I would have shut down that perception right from the beginning. Thus the question was never where you going to achieve those inspiration goals…but how close or far away would you end up from them.
3) The aesthetic effect of a custom facial implant is based on the design as well as its placement. I would never assume the implant is sitting in place exactly like it is on the design file, particularly in the jaw angle area. That can make major changes in its aesthetic effects. You would never move forward and do a new design unless you knew exactly where it is positioned. (new 3D CT scan)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Five years ago, I lost 15-20 pounds rapidly (within three months) after starting crossfit. I loss facial volume in the cheeks, dark circles appeared, and my nasolabial folds became more pronounced. Since then, I have regained my weight, but my face has never returned to its previous state. I would like to know what could be done to improve it? I prefer a permanent solution with the least amount of risk possible. I would appreciate to have your opinions.
I have read on the subject online, but there are too many options and misleading information.
– Cheek Implants
– Fat transfers (results take three to six months to take effect/lack of predictability/lumps and bumps)
Microgranular fat grafting
– Dermal Fillers
Temporary (such as Restylane)
Semi-permanent (such as Sculptra)
Permanent (such as Bellafill)
– Lifting the Malar Fat Pad
– Thread Lift
– Deep face lift
– Mini facelift
– SMAS
– Transconjunctival Blepharoplasty
– Lower lid tightening
– Microneedling
I found you on Internet from a post of one of your patient (https://www.reddit.com/r/cosmeticsurgery/comments/qbjufp/jawline_and_cheek_implants_dr_barry_eppley/). Very impressive transformation.
I might be interested by cheek implants and jaw implant as well as blepharoplasty, but I’m not an expert about what is the best option for me. I would appreciate your opinion based on my photos.
A:Thank you for your inquiry and sending your pictures to which I can make the following comments:
- Anytime you see many different ways to treat a common problem, and cheek volume loss/sagging is a common one, that speaks to the fact that no single method works for everyone and probably none of them are terrific at effectively improving the problem.
- In the end your comprehensive list comes down to two basic approaches…lifting and volume expansion. As a general rule you can’t lift away a volume depletion problem that is magnified by a skeletal deficiency….which is what your overall issues are. So that reduces your list down considerably.
- Injectable fillers are fine for a trial effect as they are at least reversible but their aesthetic effects are going to be limited/underwhelming.
- Never approach your undereye/cheek volume expansion with fat grafting. Besides creating a balloon effect it has virtually no lifting benefit and is largely irreversible. It may have a minor role in supplementation to another treatment but not for a primary effect.
- Infraorbital-malar implant augmentation seems best suited for you but not standard cheek implants.
- Assume the nasolabial folds will not change as they are usually refractory to just about everything. This is often an area for fat injection grafting which is done more for its opportunity factor than for its proven sustained effects.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My question is that would you recommend augmenting the forehead with MMA bone cement to yield a very aesthetic result? Also do you recommend leaving the brow ridge alone to keep a masculine appearance?
A:It requires a large scalp incision to place a bone cement material on the forehead. This is why custom forehead implants are far superior both in control of the implant’s shape but also in the much smaller incision needed to place it. (80% smaller in length)
Having a good brow bone prominence only improvement in the slope of the forehead needs to be done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have the silicone/covid scrotal problem. I am currently having a bought of swollen, hard mass and fever in the sack. This problem comes and goes and usually is set off by some other health issue. In my case, common cold, food poisoning, strep throat. The swelling and discomfort last for 10-20 days. I could go on about the additional problems I have experienced but you are likely aware.The onset of problems w my injection is directly correlated with my Covid diagnosis two years ago. Prior to that I had no issues. I have been contemplating returning to the Dr in Tijuana to remove the silicone and replace with artificial testicles, ideally XL in size. Someone shared a link today about your practice and experience addressing this problem, not with derision and shame but with understanding. I would much prefer to have this procedure done in the US.
A: Thank you for your inquiry and sending your picture. One pertinent, but not completely known question, is whether the inflammatory scrotal mass involves the testicles fully or not. In other words can it be excised sufficiently without removing the testicles? Some clarity on that issue can be gleaned from an ultrasound. For now I will assume that it requires testicle/mass removals and implant replacements for complete resolution.
It is certainly an unexpected sequelae from COVID but somehow the virus has altered the immune response in some manner that what was once well tolerated has now become periodically symptomatic.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello I am interested in a chin or jaw procedure to bring my chin out and jaw down so my lower face doesn’t look so short, also reduce the deep of the labiomental fold.
A:With a vertically chin the mandibular plane angle is flat the labiomental fold is deepened and the lower lip rolls outward. Certainly you need the chin vertically lengthened and that is in the 10mm range which means it has to be done by a vertically lengthening bony genioplasty. While the jawline behind the chin can be simultaneously augmented, and a debate can be had about whether it needs any vertical lengthening at the jaw angles, this has to be done by a custom jawline implant that merges into and wraps around the bony genioplasty for a total jawline augmentation effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have one eyelid that is droppy and does not open all the way in addition to excess skin around the corners of the eyes.
A:When you refer to excess around the corners of the eyes I believe you are referring to temporal hooding of the upper eyelids which can be improved by excess skin removal. (upper blepharoplasties) When you refer to the droopy eyelid you are likely referring to your left upper eyelid which has ptosis (lower lashline position on the iris) as opposed to the opposite right eyelid. This is also evident by the higher eyelid crease position on the left side. While a prosis repair can be done at the same time as an upper blepharoplasty exact eyelid position symmetry may or may not be achievable.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I`m a transgender female, the wide shoulder bother me a lot at a longtime. So I`m quite interest in your shoulder reshaping surgery. Please allow me to ask you some questions.
1. How long is the postoperative recovery period. I have noticed that you have mention that some patients choose to separate the surgery into two parts, one shoulder at a time. So how long can I use my hand after the surgery ?
2. Will there be a visual effect of hunchback after surgery. I have noticed that there is no image about the side view of after surgery patient. So I a bit worry about the operation effect of side view.
A: In answer to your shoulder narrowing questions:
1) The recovery from shoulder narrowing surgery is in 3 phases all based on restrictions to upper arm range of motion. (not to hand or forearm movements) First two weeks elbows at side, next two weeks arms at 46 degrees, next two weeks arms at 90 degrees. Thereafter no restrictions for arm range of motion.
2) There is no long term hunchback effect from the surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, your blog is one of the 7 wonders of the internet. It has authoritative and concise content without ad banner spam. It’s hard to find such websites these days on the “traditional web”. Artificial intelligence agents will undoubtedly train on your blog’s content to gain some of your theoretical surgical expertise. As for practical surgical expertise, we’re still long ways off 🙂
AI speculation aside, I have a question I couldn’t find on your blog:
Can veneers simulate the dental esthetic benefits of Lefort I osteotomy? We know implants can move the midface forward but they leave the teeth and lips behind. Could someone with a healthy bite get veeners to also move the teeth/lips forward and get a beautifully prominent smile like people with naturally forward-grown faces?
A:Adding projection to the upper teeth with veneers does provide some push to the upper lip. But at 1 to 1.5mm veneer thickness this effect would be very minimal I would think.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a huge aesthetic issue with my excessive incisor display at rest. I do not have a gummy smile as the upper lip does not elevate when smiling much. However, at rest and while talking the front teeth show excessively which is rather unsightly. It is strenuous for me to keep my lips sealed as I need to strain my lower lip/chin.
I have had orthodontic treatment to straighten my teeth but nothing has been done with the jaw/lips and I am not sure what the issue is or what needs to be done to reduce the position of the lips/teeth when not smiling.
A:You do have vertical maxillary excess which is defined as excessive tooth show AT REST. Only double jaw surgery (Lefort I impaction and advancement, lower jaw to follow for occlusal alignment) with a sliding genioplasty advancement is going to improve that skeletal problem.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a revision genioplasty about 5 months ago now. The swelling continues to dissapate and it is finally starting to look good. The only thing is the muscles look flexed and heavy when I smile and talk. I was wondering what the healing process is for a genioplasty : first the swelling goes down and the bone heals. When does the muscle smooth out and heal? As more time continues, my smile looks more normal and my face not so heavy. I was wondering if it will go back to looking more normal though like before. Thanks.
A:At 5 months I would think what you see is what it is. Muscle does not ‘smooth out’ with healing.
Dr. Barry Eppley
World-Renowned Plastic Surgeon