Your Questions
Your Questions
Q: Dr. Eppley, I need scar revision or some type of treatment on two stomach scars that are pretty bad. When I was a baby I had surgery where an incision was made across my stomach. As I grew and have gotten older (I am 24 years old now) it has grown increasingly worse in the way it looks. It is stuck down to my muscles and has made a big groove across my stomach. The surrounding skin has grown up around and over it and the top part hangs over the scar. I also have a lower stomach below my belly button which runs up and down and it is very discolored. That scar needs to be lightened. Attached are some pictures of my scars.
A: Scar revision is frequently beneficial for abdominal scars from prior pediatric surgery procedures done as an infant or child. The ‘infant surgery’ abdominal scar is exactly what I would have predicted to see. They all look like that when done very early life, the scar adheres down and the fat grows around it creating this classic appearance. It needs to be completely cut out, released and put back together as a fine line scar that is level with the surrounding skin.
While the lower vertical abdominal scar has a different origin and is not stuck down to the abdominal wall, there is no non-surgical therapy that is going to lighten the scar. Like the upper abdominal scar, it needs to be cut out and reclosed into a fine line scar to remove its dark discoloration.
t would obviously make the most sense to do scar revision on both abdominal scars at the same time during the same procedure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, what is the true recovery time from a tummy tuck? In my consultation, the plastic surgeon said around two weeks. But I have read online that it can be as long as six to eight weeks. What is the truth? I am a nurse in a hospital and work in an Oncology unit. I don’t lift patients but I am up and down all the time and constantly running around.
A: The concept of recovery can mean different things to different people and understanding what that is is of great importance in a tummy tuck…where the recovery should never be underestimated and often is. The concept of a two week recovery from a tummy tuck is not a realistic one. While you may be up and around the house and doing many normal activities, that is too early to feel comfortable doing strenuous activities. Work for many people is strenuous even though it may not seem so until one is less than 100%. Short of lifting, constantly having to be up and down is a very strenuous activity to be doing just a few weeks from a tummy tuck. A more realistic approach would be to consider going back half-time, if possible, the third week after surgery and then going back full-time by a month after the tummy tuck. This will allow you to ease your way back into work. While some people will not have this luxury for recovery time and simply have to go back after two weeks (and suffer through it), a three to four week approach as described is going to be a lot better.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, if I get silicone breast implants will I be able to breastfeed? If I get pregnant after breast augmentation should I first check and see if the implants are ruptured before breastfeeding? If the implants are ruptured can I breastfeed or do I need to get the implants out immediately or can I let my son self wean??
A: You taken taken the classic ‘can I breastfeed with implants’ question to every conceivable scenario. Most breast implants today are placed under the pectoralis muscle well below the glandular breast tissue. As a result there is no interference with milk production or breast feeding. If you have no symptoms suspicious of an implant rupture (pain, change in breast shape) I see no reason to get an ultrasound, mammogram or MRI before breastfeeding, In addition, the implants are contained within a surrounding scar capsule so even if there was an implant rupture there should be no silicone in the milk ducts. However, in the event that you have a rupture and are breast feeding, I would suggest that you do not breast-feed until you have had the rupture evaluated by a board-certified plastic surgeon.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a rhinoplasty to help with my congenital nose deformity from cleft lip and palate. I am a healthy 60 year female and my speech is fine. But my nose has never been right and until I read your writings on my problem I did not realize that it is a cartilage memory problem. This seems like it might be a magical solution and I hope you are the magician.
A: Correction of the cleft nose is a particularly challenging rhinoplasty procedure as the anatomy is far from normal. Such a nose appears deviated or twisted from the nasal bones down to the tip. The tip is most noteworthy as it is usually bulbous with thicker skin and deviated towards the non-clefted side. Part of this is due to the twisted septum internally which swings away towards the normal side pulling the tip with it. Trying to correct can be difficult and this where the role of cartilage memory comes into play. But the other major component is the nostril on the cleft side. It is deformed because it has a lack of adequate tissue support. The lower alar cartilage is slumped as it is weak and lacks the amount of cartilage on the other side. In addition the skin is deficient further contributing to the shape distortion. (which also makes it difficult to get a shape like the opposite side)
I will assume you have had some prior rhinoplasty work, perhaps years ago, and substantial efforts were made in the tip area. In my rhinoplasty experience, the cleft tip needs considerable support added including a columellar strut, spreader graft on the cleft side and an alar rim and batten graft above the cleft nostril.
If only improving the nostril shape to correct the amount of nostril retraction/asymmetry, I would just do a composite ear cartilage-skin graft to roll down the retracted nostril edge.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had jaw angle reduction surgery last year. I told the surgeon I wanted my jaw slightly slimmer, but I said I wanted to keep the same shape and definition of my jaw. However, there does not seem to be any difference in the width of my jaw, but unfortunately my jaw angle slopes now, whereas before I had a nice defined jaw angle. I didn’t want to lose the jaw angle, just some of the width. From the front I look basically the same, although I had been hoping for a slightly slimmer lower face, but from the side and 3/4 view of my face, I have lost my nice jaw angle definition, which was what I wanted to keep. Was what I was requesting impossible? Thank you in advance for any insight you can provide.
A: I can not tell you whether what you were asking was impossible as I have no idea what your face looked like before your surgery or looked like now. But I can give you some insight about jaw angle reduction. There are two basic techniques and they are done differently. Width reduction of the jaw angle is done by removing the outer cortex of the bone, either by a split osteotomy or burring reduction. Amputation of the jaw angle removes the tip of it, which make reduce width but will also shorten it vertically as well. What technique you had done is unknown to me but it sounds from the result that it may have been more of an amputation approach.
Whatever the jaw angle reduction technique that is decided on before surgery, it is first necessary to see an x-ray of the jaw angles to see how much flare they have and its thickness. That information will help determine if the procedure, regardless of the proper technique, actually has a chance to make a visible difference. This would be of particular importance in the width reduction jaw angle approach as the thickness of the bone determines whether enough can be removed to justify the effort.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in rhinoplasty but think I may need more. I’m trying to find a way to make my side profile look nice and pretty. I hate my nose as its quite large and has a small bump on it therefore I really want rhinoplasty. I also have a small slanted forehead and small chin so it looks like my face goes into a point at my nose. What would be best to change this? Please help, many thanks.
A: By your description, your three main side profile features have an imbalance. Your nose is too big and the forehead and chin is too small, creating the profile that you dislike. In trying to figure out what procedures you may need that creates the best change, it would be important to do some computer imaging. The procedures of rhinoplasty and chin and forehead augmentation must be looked at individually as well as in comboantion to see which creates the best change. It probably goes without saying that all three create the greatest profile improvement but do you really need them all. I suspect that the rhinoplasty and chin augmentation alone may be sufficient and produce the best return on the effort but that remains to be proven by the imaging predictions. Please send me a side profile picture at your convenience to help you make that determination.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in facial reshaping. I am a 27 year old Asian-American female who, through some weight gain and with late puberty, have developed to me what is a foreign look which has caused me great distress. My objective with plastic surgery is to look all-American. I want a natural look, I don’t want it to look like I got plastic surgery at all. I noticed that my eyes grew higher on my head and slightly closer together. I grew a slight bump on my nose and my cheekbones grew flatter and higher on my head. I have gained weight intentionally to fill out of my face because I felt I looked too hollow. The changes have been about a mm but it bothers me considerably. I feel like I am in someone else’s face and it has changed my life for the worse. I am attaching some photos of the way I look now as well as a couple of photos of the way I looked before when I was in college. I am also attaching photos of how generally how I want to look. The biggest objective is that I want to look American, because I am. I am thinking of having my eyes and cheekbones literally moved lower and wider to give it a feminine and youthful look. I have noticed that male to female surgeries don’t look believable if the distance is still too long between the eyes and mouth. Please let me know what procedures you recommend. I am thinking of cheek implants, nose job, and eyelid surgery too? I really need plastic surgery for the life I want to live.

A: I would to make a few general comments about your facial surgery objectives. First you are going to need to set some realistic objectives. There is no plastic surgery that is going to make you look ‘All-American’. You have Asian features, and while there may be some room for softening, you are always going to look Asian. Secondly, you have thick tissues and thick skin. Every American female face pictures that you have shown has much thinner skin and softer features due to a completely different facial bone structure.. While I realize those may be examples, I do not want you to think your facial features can ever be as refined as theirs…you simply have different tissue thickness which only allow for some moderate changes at best.
While there is some facial changes that can be done, those have to be understood in the context of what may be achievable. This issue up front is more more important than what procedures to do…for within lies the key element of whether any patient will be happy after their plastic surgery operation. Some facial reshaping changes can be made but they will not have a facial transformation effect. They will only improve upon the basic appearance of your face.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My concern is my facial asymmetry. My one side of my face did not develop normally, my left eye sets lower than the right. Also my left cheek bone is under developed. I want to know if it can be corrected. I have attached some pictures so you can see what I mean by one side of my face being different than the other.
A: Thank you for sending your pictures. You have a left-sided form of facial asymmetry due to some underdevelopment of various facial structures. This is probably a minor variant of hemifacial microsomia. I can see in looking at your pictures you have some orbital dystopia (lower eye socket) with malar (cheekbone) hypoplasia as well as some chin asymmetry. (shift towards the underdeveloped left side) The best treatment approach would be orbital floor augmentation, medial z-plasty canthoplasty, cheek augmentation and a chin straightening genioplasty. But probably what bothers you the most is the cheek-eye area which is what you see and look at the most.
I believe the eye and cheek area could be significantly improved but I wouldn’t use the term ‘correction’ as that implies they could be made perfectly normal which they can’t can’t. It is just a question of how close to normal can they be made.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am considered having an armlift for my bat wings. I have looked at a lot of scars from that surgery and most of them are underwhelming. I hate my batwings but am worried that I might hate the scar to remove them just as much. Some of the armlift scars seem to be quite long, often crossing the elbow and down past the armpit. Does every armlift scar have to be that long? Do you have any pictures of really good looking armlift scars?
A: The length of the arm lift scar can be shortened or lengthened as the patient desires although, in some cases, that may affect how much improvement is seen. It is also important to understand that with varying degrees of bat wing problems the skin excess may cross the shoulder and elbow joint areas, particularly in the bariatric or massive weight loss patient.
When it comes to the scar for the armlift, one has to approach it as the worst case scenario..as you never know in anyone how well it would do. In looking at our people’s photographs, one has to understand that is them and may not signify at all what may happen in you. Even if you saw a great arm lift scar on another person, that should not be the motivation to undergo the surgery…as you are banking on that will happen in you. You should make your decision for surgery based on ‘typical’ or ‘average’ results, not the best that has happened. If you look at an airlift scar and think it looks terrible, then this surgery is not for you. If you look at an arm lift scar, wish it looked better than that but still think that trade-off is better than having batwings, then it is a good operation for you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a full breast reduction when I was a later teenager. I am now 36 years old) Now that I am older and with time my remaining breast tissue has fallen and is saggy. I would like to now have a breast lift to reshape them and give them more of a perky appearance. My original plastic surgeon has since retired and office records are no longer available. One plastic surgeon I consulted with said he said he would be worried about doing a second lift after the reduction. I have read from other plastic surgeons that a lift with a small implant is safe and will help. Is this a worrisome procedure after having a reduction? I would be open to a small implant but ideally would like to be the same size, just rounder. I’d love to be able to go bra less. Is this possible?
A: It is not rare to have a breast reduction done when someone is young that wants augmentation or a lift many years laters. It is perfectly safe to do a breast lift now using the same scars from the original breast reduction. The blood supply to the nipple through the central breast tissue pedicle will be undisturbed. It would be similarly safe to place an implant under the muscle which is beneath the overlying breast tissue mound. The role of the implant is to maintain upper pole fullness which a breast lift long-term will not do.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in forehead augmentation/reconstruction for a congenital skull deformity. In terms of using cement on my forehead, by how much can we get an additional thickness there, i.e. what distance can we add to the flatness/deficiency? Why is it cement (on the forehead) instead of a prefabricated implant? I have a very rough terrain of the forehead. In our opinion the implant’s inner side would hide all the problems beneath, but the cement treatment might be not creating a proper elliptical smoothness unlike an implant should do. Correct us please if we are wrong, it is just to dispel our concerns.
A: The amount of expansion of any skull bone surface is based exclusively on how much the overlying scalp will stretch. How much the scalp can stretch is a function of many factors, including scar from prior surgery and an innate ‘looseness’ factor. As a general statement, skull expansion can achieve up to 25mm in thickness if a full coronal incision is used for access.
Forehead augmentation/reconstruction can be done very successfully, using either intraoperatively applied bone cements or prefabricated implants. One is not necessarily better than the other. A bone cement is an intraoperatively made putty froml iquid and powder components. It is applied as a putty to the bone surface and then shaped by hand to whatever external shape is needed. It has an intimate connection to every nook and cranny of the irregular bone surface as its outer surface is shaped into a smooth round/elliptical shape. Bone cements can be either of PMMA (acrylic) or hydroxyapatite (HA) compositions. Most large volume bone cement cranioplasties use PMMA due to its lower cost. A prefabricated skull/forehead implant is made from the patient’s 3D CT scan using computer designing software for its creation. It is then fabricated in a silicone material for implantation. It too will have a good fit to the underlying bone surface and an external shape of whatever is so designed. It is the costliest of all the alternatives due to the design process.
In short, your perception of the differences between a bone cement and prefabricated implant is not accurate. They are just different ways to get to the same place. They differ primarily, however, in the cost to do them.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in perioral mound liposuction. I have a problem with fat pockets around the corners of the mouth. I’ve had buccal fat pad removal before, but it did not help at the right area. I also have some fat along my jaw line that I do not like. Do you think it is possible to perform microliposuction at those areas? And how drastic will the result be? Are there any complications with this surgery? Have you done this surgery many times?
A: I am not surprised that a buccal lumpectomy do not affect your area of concern as the large buccal fat pad or any of its arms does not extend downward toward the corner of the mouth and jawline. This area, as you have correctly pointed out, is known as the perioral mound area which is a subcutaneous layer of fat. (not like a well defined fat capsule like the buccal fat pad) I have done perioral mound liposuction numerous times. It is done with a very small cannula from a small incision inside the corners of the mouth. As there are no facial nerve branches in this area, one can aggressively liposuction it. It never produces a large amount of fat and often only a few ccd is obtained, but in the right patient, that can make for a noticeable thinning effect.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have an indented lower end of my sternum, I think it is called pectus excavatum. I have read about implants to fix but I don’t want a scar on my chest to put it in nor do I ever want any problems with an implant down the road. I was wondering if I was a good candidate for an injectable method of pectus excavatum repair. That seems perfect to me for my chest problem. I have attached some pictures.

A: Thank you for sending your pictures. You have a very discrete lower tail of the sternal depression or a limited pectus excavatum deformity. It’s size and location is deal for an injectable form of pectus excavatum repair or sternal augmentation, the question is one of which material to use. The options include your own fat, hydroxyapatite granules or an hydroxyapatite cement. Having used all three for an injectable sternoplasty approach, I would opt for hydroxyapatite granules or fat. While I love injectable fat (and yes even you as a thin guy have enough to harvest) as it is both natural and will never created an abnormal contour problem, it is very prone to partial or complete resorption due to the tight attachment of the sternal tissues. The pressure of the tight overlying skin is the cause of fat atrophy/resorption. How much of the fat will take can not be precisely predicted before surgery. Hydroxyapatite granules can be injected, are very moldable (as they are granules), will not resorb, and have low risk of any contour/shape issue. Any of the bone cements (composed of hydroxyapatite) are great space fillers and are permanent but are very prone to being overfilled or having an irregular shape (as they set as a hard mass), thus requiring a revisional procedure for adjustment should that occur.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in minor skull reshaping. I would to have a point or bump at the crown of my head reduced. From what I have read, it is does not appear too big (tall) that it could not be adequately reduced based on the thickness of the skull bone. I have attached a front and side view picture of it. Now that I have lost my hair, what used to not be an issue has become one.

A: Thank you for sending your pictures. Your crown ‘point’ is very obvious and I have seen this very skull issue numerous times. Usually this can very successfully be burred down to be confluent with the surrounding skull contour. But because it is in the midline over the vertex of the skull it would be important before surgery to check a simple x-ray to determine the thickness of the skull in this area. I have seen a few times in taking this area down that the bone becomes quite thin and the dural lining of the brain is close by. While this is not dangerous, it would be important to know beforehand if an adequate reduction can be done so that the surgical effort would have been worth it. Also, as is the case in every male with elective or non-elective lack of hair, is the issue of the fine line scar to do the procedure. That small aesthetic trade-off must always be carefully considered.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a breast augmentation three weeks ago. I am no longer worried about any particular problems at this point as they look great. What I wonder is if the heat from a hot tub can weaken the implants in any way or cause them to prematurely break down and leach out the silicone material.? Could it weaken them in any way? I have read that it is ok to swim after they are healed but can’t find anything about what happens if they are immersed in temperatures above body level like 104 or 105 degrees. How heat resistant are these materials?
A: The answer to your question comes from the Periodic Table of Elements. Breast implants are composed primarily of silicon-based materials. Silicon is a metalloid element (#14, atomic weight 28) that is very stable and non-reactive. (it is actually less reactive than carbon) When combined with oxygen, a wide variety of polymers are created which are used to create elastomers (rubber-like materials) which make up breast implant shells and the internal gel. They are very resistant to degradation including a high heat resistance and are structurally stable from temperatures ranging from -55 degrees to 300 degrees F. Thus a hot tub poses or even a sauna that reaches air temperatures of 150 degrees F or higher poses no risk of causing any implant-related issues. This is not to mention that they are also protected by your body tissues which would suffer a burn injury far sooner than your breast implants ever would.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 25 year female and I am looking for an honest surgeon who can do a chin reduction surgery for my long chin. I am wondering if you can reduce the height of my chin vertically? I am not sure if I also need to reduce the width of my chin. I feel I have a long chin when I look at the front of my face in the mirror. To me what most important are the risks of undergoing this surgery and the outcome. I am not just concerned about nerve damage but I am also afraid of having loose/saggy skin after the chin reduction surgery. Because our skin sag when we get older, will this mean any chin reduction will make the sagging worst when we are like 45 or 56 years old…even if the soft issues was reattached and tighten properly? I look forward to hearing from you.
A: Vertical chin reduction is done by one of two approaches, an intraoral wedge reduction genioplasty and an external submental chin reduction. Which one is best for any patient depends on ow much vertical reduction they need, does width reduction need to be done as well and do they have any pre-existing soft tissue excess or sagging. In either case, the soft tissues are managed with both procedures. In the intraoral genioplasty approach the soft tissues remain attached to the inferior chin segment and and are never detached so they move up with the reattachment of the bony segments. In the submental chin reduction technique, a wedge of soft tissue is removed and tightened after the bone is reduced. In general, the submental approach is more effective at vertical chin reduction than the intraoral wedge genioplasty approach. I would need to see front and side view pictures of your chin (non-smiling) to see which approach may be best for you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I recently had chin and jaw angle implants combined with fat transfer ten days ago. I see that my lower face is much wider than expected. I realize that a lot of this is swelling and that fat transfer is overdone with the expectation that much of it will be reabsorbed. However, if there is a “window” of time that would be possible to remove the jaw implants (the chin is just fine) then I would want to be aware of that.

A: One of the very common early postoperative features of any jawline implants, including the chin, is the amount of swelling that occurs. Suffice it to say it is tremendous and doesn’t signify at all what the final outcome will be. It is actually very common that many patients in the first three weeks want to remove their implants as it just seems too big. While I am always happy to do whatever the patient wants, any judgment now is way premature and doesn’t indicate what the final results will be. As a general rule, the result of any facial implant follows the general guideline of 50% by 10 days, 75% by three weeks, 90% by six weeks and the real result (100%) by three months.
There is also the psychology of facial structural changes. Facial augmentation of natural structure is not like a facelift. In anti-aging procedures, people are psychologically comfortable with the swelling because they are just trying to go back to a place they know. (what they used to look like) Facial structural surgery is more psychologically unsettling because the person is going to a place of which they are not familiar. (a new look) This is tremendously unnerving and there is a natural tendency to want to return from when they came. If most patients can just get past this transition period (which is usually about 3 weeks, when a lot of swelling goes down) then they are usually fine and happy with their new look.
It is important to remember that the jaw angle implants are only 3mms thick, just a sliver of width really. So don’t let this temporary facial look with the swelling remotely think that the final result will look anything like what you see now. When you combine the swelling from the jaw angles with the fat grafting, it ail, temporarily look especially heavy on the lower third of the face.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have an occipital knob on the back of my head just like the one you have shown in your website. It’s destroying my self confidence and I would like it removed. How is it done, what is the recovery like and how much would a procedure like this cost?

A: The occipital knob is a prominent bulge of bone at the back of the head on the lower edge of the occipital bone along the nuchal line in the midline. It is an abnormal thickening of completely cortical bone that sticks out like a knob. It is most commonly a concern for men who shave their head or have very short hair. I have seen some really impressive occipital knobs that are extremely prominent. Surgical reduction/flattening of this bone knob is done through a small horizontal incision over it, usually no greater than 3 to 3.5 cms in length. (limited incision occipital reduction cranioplasty) The knob is burred down to be smooth with the surrounding bone. Usually I will then suture the soft tissues down to the bone surface through bone holes to make sure no fluid develops between the skin and the reduced bone. The skin is then closed with small dissolveable sutures. This procedure takes about one hour under general anesthesia and is done as an outpatient procedure. The cost of the procedure, all expenses included, can be obtained by contacting my office for a quote.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am seeking gynecomastia reduction. I have hard lumps bilaterally under each areola. I am a 32 year old male and would like to have them surgically removed. I have a toned muscular body and It is somewhat annoying. I’ve had this condition since puberty and it hasn’t resolved. They are visible through shirts and when I’m shirtless or in the water it is somewhat noticeable. What is involved in getting this condition resolved?
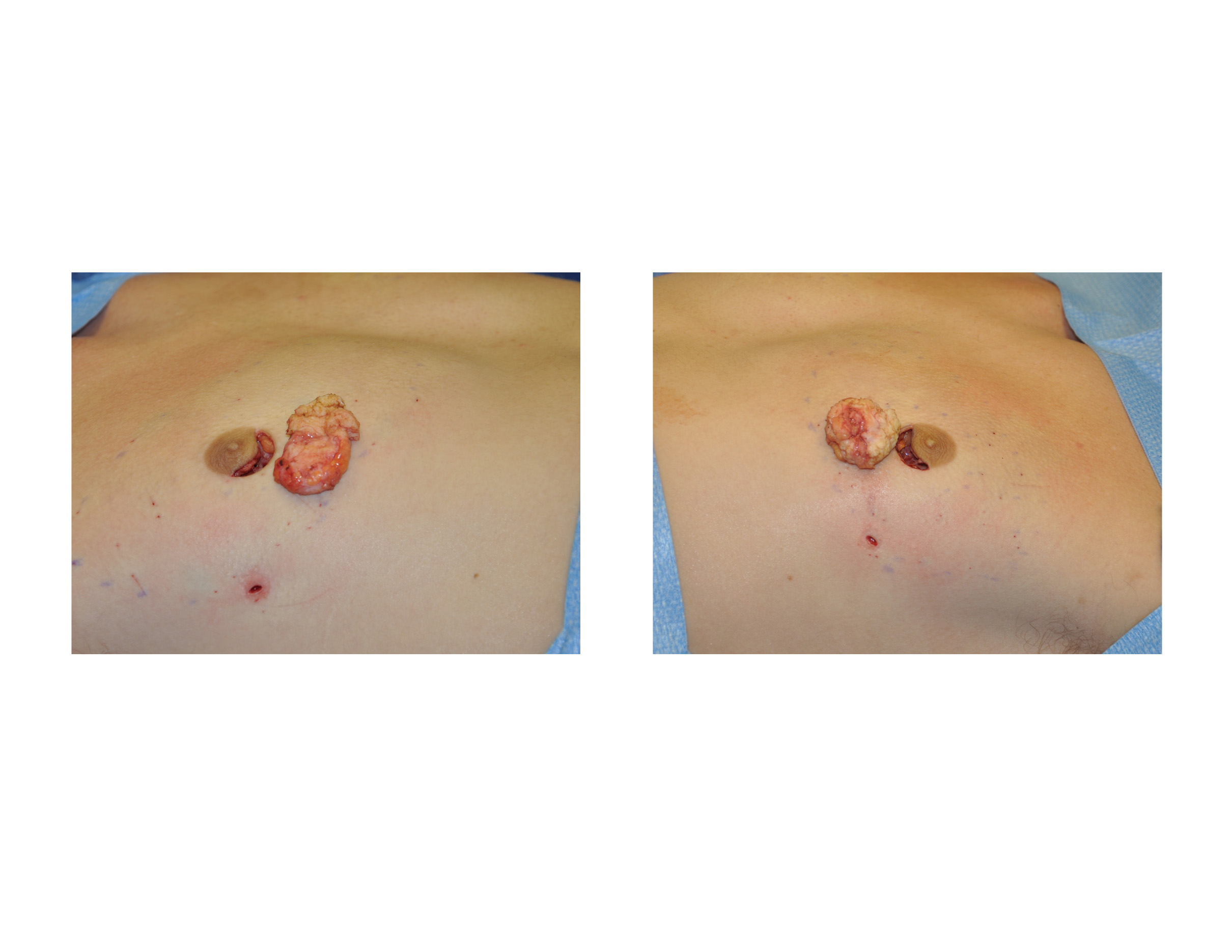
A: It certainly sounds like you have areolar gynecomastia which appear as isolated hard lumps under the nipple. There may also be extra breast tissue that is softer that extends outward from these hard lump areas. This type of gynecomastia reduction is done through inferior areolar incisions including the liposuction portion if needed. Most such areolar incisions heal imperceptibly. This is done as an outpatient procedure under general anesthesia. Drains are not usually used for such limited male breast tissue excision procedures. Recovery will take a few weeks until you can return to full activities including strenuous exercise.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, when you do liposuction do you close the incisions with stitches or staples or just leave them open? A relative of mine across the country had liposuction recently on her stomach and thighs and they didn’t close her incisions. I didn’t realize that liposuction was done that way. She said her incisions bled for days and she had to keep changing her wet bloody garments. How does this affect the liposuction result and does it increase the risk of infection?

A: Whether a plastic surgeon chooses to close liposuction incisions is a matter of personal preference. There is no evidence that not closing these incisions increase the risk of infection or affect the outcome of the procedure in any way. It is common for the liposuction incisions to leak fluid for 24 to 36 hours after the procedure which is primarily induced by the wearing of the compression garments. (squeezing it out) What one sees, although it looks like a lot of blood to the patient, is actually just a little bit of blood mixed with the tumescent solution that was infused at the time of the surgery. One could argue that the more this fluid comes out the less swelling and bruising that will subsequently occur. If the fluid does not come out it stays in the body and must be absorbed over time as one heals. If the incisions are closed probably less fluid comes out but a fair amount will still ooze out anyway. This is why I tell patients to not sit or lay on anything they value (without a blanket) for the first few days after surgery.
That being said, I do prefer to close my liposuction incisions (with the exception of those placed inside the belly button) as it increases the likelihood of better scars, small as they may be.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, years ago I had a brow-bone reduction surgery for facial feminization. Unfortunately, the surgeon I chose tried some novel procedure that ended up leaving me with a missing anterior sinus wall and bone chips lodged in my frontal sinus. Another surgeon, an ENT, then obliterated my frontal sinus with hydroxyapatite. This fixed the air leaks and replaced the missing bone, but left obvious irregularities in my forehead. I recently had a CT scan done and discovered that he also failed to completely obliterate the sinus; there is still a cavity on the left side. I came across your page while doing research and discovered that you had a lot of experience in forehead work as well as craniofacial experience, and I was wondering if this was something you think you could fix. I’m hoping to have the last of the sinus obliterated with hydroxyapatite or similar and to have the defects in my frontal bone filled.
A: In doing brow bone reduction surgery, removing the anterior table of the frontal sinus and putting it back as morselized bone chips is not going to be a successful strategy. (as you have discovered) This will leave one with significant indentations and irregularities over the brow bones. Repairing this problem with frontal sinus obliteration by mucosal lining removal, obliterating the frontal sinus ducts with bone grafts and then filling it with hydroxyapatite cement up to the level of the desired brow bone shape is the correct treatment. However if one fails to get out all the lining or does not obliterate the frontonasal ducts, a residual frontal sinus cavity will remains which could be a source of infection.
I am going to assume that this residual sinus cavity is located near the frontonasal ducts underneath the hydroxyapatite cement. If this asymptomatic and the cavity is clear, then I would just fill in the outer brow bone contour and leave it alone. However, if it is a source of pain or frontal sinus infections, then it should be removed and obliterated with cement along with the brow bone/forehead contouring.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in deltoid implants which amongst other procedures as I learned you are very skilled at. I have pictures for my shoulder which are attached. The dimensions for the augmentation are 16cm measured from clavicule down lateral view to end of the deltoid in the center line, the widest part is around 10cms with a projection of 2 cm.

A: Thank you for sending your shoulder augmentation desire and dimensions. Deltoid implants are one of the most uncommon type of body implants but requested for them are becoming more frequent. One of the reasons I asked for them is to have a vision as to where the patient sees the location of the deltoid augmentation and the dimensions that the implants have to be. As there is no off-the-shelf premade deltoid implants, I have to either use an existing style of body implant (usually a calf implant or a custom silicone carving block) or have a custom one made. As it turns out there is an existing silicone carving block with the dimensions of 16 cms long, 9 cms. wide and 2 cms. high. So that does fit the dimensions you have given although although that is probably a bit big. A more appropriate deltoid implant size would be 14cm long, 7 cm wide and 1.5 cm high. The other consideration is knowing the location and the implant size I have think about the incisional location to put it in during surgery. Usually this is done from the back side of the shoulder rather than a direct incision over it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m a 38DD and my breasts sag slightly. I have been treated for back pain for several years. My question is…is it difficult to get this procedure covered by insurance? I’m very interested in getting a breast lift but could not pay the entire bill out of pocket. Should I even try to pursue this?

A: To answer your question, the first thing to determine is whether you are trying to achieve a breast lift (with no reduction) or trying to get an actual breast reduction done. (smaller breasts with the lift that comes with them) Breast lifts are never going to be covered by insurance as that is a cosmetic procedure. Conversely many breast reductions are covered by insurance as they improve back, shoulder and neck pain as the size of the breasts are reduced. Thus they are often viewed as medically necessary and may be covered. But their potential coverage has to be determined before surgery by a predetermination letter which documents your breast size, the symptoms associated with them and how much breast tissue will be surgically removed. From this information, the insurance company bases their decision for coverage.
But when it comes to breast lifts, there is no purpose in trying to see if insurance will pay for it as that can be determined right now…there is no medical need and thus no insurance coverage for the operation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi! I’m 23 years old, and I would like to have breast augmentation. But I am a petite person and a ballerina. I wouldn’t want anything bigger than a medium B cup, is that possible? I really don’t know the difference between the types of breast implants so I don’t know which is best for me. How much does this surgery cost? Thanks.
A: Any size breast augmentation can be done, even for very small size requests. Implants comes in volume as small as 100ccs and go all the way up to 800cc in silicone and 960cc in saline (can be filled that volume from a 800cc implant) The cost of the surgery is somewhat dependent on the type of breast implant used so knowing what you would want is important.
While both saline and silicone breast implants are available, FDA-approved and can create excellent breast augmentation results, there are some differences between them that every woman needs to fully appreciate. While saline breast implants costs less (total cost $3,999) and can be placed through the smallest incision, they will one day suffer catastrophic failure (deflation) and are prone to developing rippling on the bottom edges of the implant in women who are thin with little breast tissue. Silicone implants cost more (total cost $4,999) and require a slightly larger incision to put them, but have virtually no rippling (most natural feel) and do not fail by deflation but by a ‘silent rupture’ process in which the breast does not lose volume or size. Because of the delayed awareness of an implant problem (which is harmless) silicone breast implants will last longer.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am in need of jaw angle implant revision surgery, I had large, off the shelf, silicone jaw implants done two weeks ago. To me (at this stage) they look too big and are asymmetrical. As you can see from the photographs there is a distinct difference to both sides of my face, with one jaw side being lower than the other. i am also concerned that they bulge and “round out” my face from under the ears. also believe they made my face longer and squarer. I want badly to correct this and if this entails customized implants that achieve (or approach) symmetry, I hope you can help.

A: Let me start by first making a general comment about jaw angle implant surgery in men. Just about every patient in the first few weeks or month after surgery thinks that the implants are too big, asymmetrical or both. While they may very well be (I obviously don’t know what you looked like before and what your aesthetic goals were…and the beard adds another visual element which may or may not be helpful in interpretation of the results), what is important to know is that 50% of the final result is seen at 3 weeks, 75% of the result is seen by 6 weeks and it takes a full 3 months to see every detail of the final result in any form of facial skeletal augmentation surgery. So at just two weeks after surgery what you are currently seeing may or may not be a harbinger of the eventual outcome of the procedure.
I say this because I have seen numerous men jump too quickly into jaw angle implant revision surgery…long before the final result was apparent. There is an accomodation phase to the new look and that does not happen for most patients in the swelling phase of the recovery period.
The two most common complications from any facial implant surgery, in particular jaw angle implants, is what you are feeling now…over/undersizing and asymmetry. Given that you are still somewhat swollen it it hard for me to know what look you were trying to achieve and what makes the way it looks now not desired. Did you have computer imaging done before our surgery to get a feel for the look you could achieve in your face? Your description suggests that they are too big (wide) and are of a lateral design…which would account for the rounded lower face look. I suspect these are 11mm wide lateral angle implants. Such dimensions can also make the face look more square and longer (which is what many jaw angle patients want) but this style implant has very rounded edging.
Jaw angle implant asymmetry is a function of placement and how secure the implants are onto the bone. They were placed from inside the mouth but where they secured with screws?
I ask these questions because the solution to your jaw angle implant concerns may already lie within you (modification of existing implants and their positioning) While custom implants can always be made, I would first look at whether what you have can be salvaged to the right amount of jaw angle augmentation and symmetry…consisting of the simplest and most economic approach to jaw angle implant revision surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I need earlobe reconstruction. I’ve stretched my earlobes to two and a quarter inches. I’ve decided I want to get them fixed and I know you are the surgeon who is best at this. I was wondering how long will I need to let my earlobes shrink before getting the surgery?

A: I would allow them to shrink down for a minimum of 6 weeks, which will be about 75% to 90% percent of how much they will shrink. Usually three months is tehe time when 100% shrinkage has occurred. That is sort of a standard protocol since there is rarely is a need to fix them on an immediate basis. But having done several urgent cases where the earlobes have torn from overstretching and having fixed both sides at the same time, the outcome has been the same whether the earlobes were allowed to shrink down or not. This is not surprising since what is really expanded is the outer rim of earlobe skin which gets removed anyway. It is just smaller if the gauges are removed beforehand. The adjacent earlobe tissue around the gauged site (whcih is what is kept to reconstruct the earlobe) does not change that much.Thus I do not believe it matters greatly whether you allow the earlobes to maximally shrink or not. But if you have the time then I would do so.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a fat injection breast augmentation done one month ago. I took a vacation one week after surgery and I was fine. Well exactly two weeks after my procedure I noticed my left breast was bigger, swollen, tender, painful, and very warm. I thought nothing of it and my doctor said it was normal. When I questioned why my right breast didn’t feel that way he said each breast healed differently. Well the next day after my symptoms got worse and I felt dizzy and weak. I woke up soaked and noticed a yellowish pinkish discharge leaking from my left breasts incision. I ran to the ER and was admitted for 6 days. I had an abcess and required surgery for drainage. I was given a lot of antibiotics and I’m now having to clean and change dressing twice daily. This has been a total nightmare! How long will it take for my infection to go away and for pus to stop leaking? When will my incision close if I have no stitches? I’m afraid my breasts will now look deformed and different in size but im terrified to get another procedure done for correction. What caused my infection? Why only my left breast? Could too much sun exposure, drinking, and pool have caused my infection?

A: Sorry to hear of your very unfortunate complication. While using your own fat for breast augmentation is a natural material, that does not exclude it from the risk of infection. (although that risk is probably lower than with implants) Because the injected fat has no blood supply and must acquire it after being transplanted, there is a period of time after surgery when infection can develop. That is usually between 10 and 21 days after surgery, the time when you are off antibiotics and bacteria have had time to multiply and grow.
Almost all infections that occur close to surgery, regardless of the procedure, occur because some bacteria go into the wound during surgery. Why it occurred in one breast and not the other will never be known but fortunately it was just one breast.
Once you have developed an infection around injected fat, there will be fat loss or less take in that breast. Probably what you have coming out of your wound now is mostly liquified fat rather than pus which is injected fat that is breaking down due to the infection.It will probably two to three weeks until this clears up and heals.
That breast should be allowed to heal for a year, get soft to the feel, and see what the final amount of fat take will be. I suspect there will be some breast asymmetry due to different amounts of fat take per breast. Correction of that breast asymmetry, if it occurs, will be by additional fat injections. Just because you have had this complication does not expose you a subsequent or higher risk if you have the procedure done again.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in some type of forehead reduction. I am a young woman and I’m not happy about my face at all. The biggest problems I have are with my jawline and my frontal bone. I also have really deep insetted eyes. I’m kinda chubby but I used to be skinny and I had to exact same problem. I have big cheeks , something like squirrel cheeks and jowls on the side of my face. I really want a nice tight jawline. When I tighten the skin together and pull it through my ears I see it the way I would want it to be. I was wondering if that is possible for me without having a jawline surgery.
I have a very big frontal bone and I would love to have a nice flat forehead like most women have. I was wondering if that is possible for me to get it flattened. Maybe there is also someting you could do for my deep insetted eyes. I want to send you some picture’s and I’m wondering if you could look at them yourself and if you have any tips for me to make me as beautiful as possible.
A: Thank you for your inquiry and sending your pictures. The most effective procedure that you could do for your face would be a combined orbital/forehead reduction and hairline scalp advancement. This would reduce the depth of your eyes, lessen the brow ridge prominence, and make the forehead look smaller.
Only a jowl lift can create the desired look you are after along the jawline and you are too young for that procedure. There are no non-surgical methods that can create the same effect.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in scar revision surgery. I have a transverse abdominal scar from surgery I had as an infant. It is “socked in” . My skin is adhered to my muscle and there is an overhanging lip above the scar. I am 27 years old. I also have a vertical 4.5 inch scar below the belly button I would like to have lightened. It is two years old.
A: It is very common to see scars from abdominal surgery done as an infant to be completely adhered to the muscles. This is because at such a young age there is little to no subcutaneous fat between the skin and the muscle. The incision line scars down to the muscle (as there is little to no fat interface) and appears as an indented fixed line as fat tissue develops between the skin and muscle around it as the patient gets older. This can be dramatically improved by scar revision surgery by cutting out the scar, releasing the surrounding tissues from the muscle and advancing and closing the skin edges together. While a scar line will still be present, it will be leveled and a much narrower scar. Such scar revisions can often make for a dramatic change in the appearance of such scars.
When it comes to scar lightening that is a different matter. There are not many effective therapies for scar discolorations other than to cut (excise) out the scar.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have two issues: 1) a birthmark the full length of my cheek which I’ve had my whole life and 2) the facial hair covering the birthmark is substantially thicker than that covering my other cheek. Can you help with either of my two issues? Photos attached.
A: What you have is a congenital nevus of the face. Its characteristics are well known and include being born with it, the involved skin is thicker and more pigmented and the hair that grows from it is often darker and thicker. The key concept to understand about congenital nevi is that involve the full thickness of the skin. Thus they can not be removed or reduced by laser resurfacing or treatment method. The entire full-thickness of the skin needs to be cut out (excised) either through serial reductions or as a single surgery and then covered with a skin graft. While this would cure the nevus, it would result in a worsening of the aesthetic appearance of the face and I do not believe you would consider it an improvement. This is a long way to say you are better off to leave it alone as the treatment of it is worse than the problem.
Dr. Barry Eppley
Indianapolis, Indiana