Your Questions
Your Questions
Q: Dr. Eppley, I have some questions regarding facial slimming with buccal lipectomies and perioral liposuction.
I’m interested in doing the procedures and I’m wondering if you think that you could help me with this.
To give you the full background:
I’ve previously had some treatments done in my face in order to shape it in a pleasing way. I used to have so called “hamster cheeks” and where really heavy on the lower face (think reversed egg ) – so I’ve had cheek implants done and have had a buccal fat pad removal that resulted in success on the left side, but still with fat remaining on the right side, leaving the face to be uneven…
The reason why the plastic surgeon didn’t succeed on both sides is due to the buccal fat on my right side being scattered around (at least that’s what he told me).
So if possible I’d love to have the left and the right side be symmetrical (as much as possible, as I know this isn’t an exact science) – do you think it would be possible to “go in” on the right side again and correct it? Knowing it’s a very sensitive area with nerves etc.
I can also start seeing droopiness on the perioral mound area (the side of the mouth) due to excess fat – making me look sad when I’m really not. So this is something I really like to get rid of. I’ve inherited it from both my mom’s and dad’s side, and it’s something that I’d like to correct while the skin still heals an bouncing back easily.
A:Thank you for your inquiry. I have never seen or heard of the buccal fat pad being ‘scattered around’ as that is not how it is anatomically located. I suspect he just wasn’t able to locate the buccal fad capsule as it is often deeper than what most surgeons think it. Thus trying to ‘redo’ the left buccal lipectomy which seem appropriate. But on both sides perioral liposuction can be done to complement the buccal lipectomies and provide some further facial slimming effects.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Overall, I am looking for sharp angular model-like features.
As in the custom jawline implant design:
- Is the chin square?
- I am unsure of the exact terms to describe the features I am looking for, but I would like the resultant jaw to be square, sharp, and chiseled.
- I would like this sort of square jaw angle if possible/suitable.
As in the custom infraorbital-malar-maxillary implant:
4) I would like a bottom part to the implant covering the area to make it into a full mask implant in order to get as much forward maxilla/midface projection as possible (within your guided measurements) to get that LeFort effect.
5) I just wanted to make sure the zygomatic arch part of the model cheekbone is included as there are different lengths on different skulls shown on the website. Not sure if there is any difference on the lengths and the cheekbone effect.
6) I would like zygos/cheekbones with both forward and lateral projection meaning I would like to add slightly more forward projection to the zygomatic area (if possible/appropriate).
7) I have concerns about removing a Negative Orbital Vector and negative canthal tilt, just wanted to ensure that the implant will tackle this.
8) As I believe the custom midface implant is going to be inserted through the eyelids and closed using a lateral canthopexy and we are using spacer grafts to lift the bottom eyelid – is it possible to change the outer corner of my eyes slightly to fix their asymmetry and eliminate excessive scleral show and to give the eyes a slightly positive canthal tilt or “as almond as possible”?
9) Reading anecdotes from others who have gotten infraorbital rim implants is that though the support under the eye is a significant improvement but there is still a bit of hollowing due to the lack of fat under the eyes – is there a solution to this such as under eye fat bag repositioning or fat pocket transfer? Is it possible to do it at the same time as adding the spacer grafts? Should it be done post implant healing? Could it be recycled fat from the buccal liposuction?
10) I would like to get my whole mouth area improved – this includes mouth widening, lip corner and lip projection. I asked you asked about this via email and you said I would need to wait a minimum of three months post jaw surgery. As I believe this can be done under local anesthetic, I believe seeing you in person will be the best gage on what to do with that. Same thing with a possible fat transfer to the upper eyelid area. I’m not sure if I have Ptosis of the eyelids or not – can this be evaluated in person and done under local anaesthetic at another point in time as well?
11) In case there is emergency, should I have a local surgeon kept in the loop about the surgery before I go to the states?
12) What should I do in case I believe there is an infection or something wrong?
13) Do I need to clean shave for surgery or is having a light beard okay?
A: In answer to your custom infraorbital-malar-maxillary and jawline implants:
1) The current design of the custom jawline implant has a square chin. Whether it should be more sharply square in the design can be debated.
2) The ability of any custom facial implants design to show through depends on the thickness of the overlying tissues. Thinner facial tissues allow these designs to show their defined designs, thicker facial tissues do not. So the patient has to appreciate what is possible within the limits of their own facial tissues.
3) The squareness of the jaw angle design must be considered very carefully. If it is over squared on the design the implant can protrude beyond the posterior edge of the masseter muscle causing what is known as implant reveal, an aesthetic deformity.
4) A midface mask implant design can replicate a LeFort-like effect but a more complete one.
5) A zygomatic arch component can be added to the design to go back as far along the arch as aesthetically desired.
6) Forward and lateral projection at the zygomatic area is common in these implant designs.
7) A custom infraorbital-malar implant is the most effective approach to correction of the negative orbital vector and negative cantonal tilt.
8) Such an infraorbital-malar-maxillary implant can NOT be solely inserted through just the lower eyelid incisions. This will need to be combined with intraoral incisions as well. In addition, while the implant may be designed as one-piece, it can neither be manufactured as one piece nor inserted as one piece. There would be a split in the implant design at the level of the infraorbital-malar and maxillary portions to allow both manufacture and surgical placement. But it will fit together int surgery like a puzzle piece.
9) Recycing the fat from buccal lipectomies for additional volume augmentation over the infraorbital area can be done at the same time. But the risk of infection is increased since the vascular fat grafts are placed on top of an avascular implant surface.
10) With the stretch on the lips from the surgery delicate soft tissue procedures such as mouth widening are not advised at the same time. Postoperative facial swelling will adversely affect the appearance of the resultant lip/mouth scars.
11) There really won’t be an emergency per se.
12) Infection is the only real semi-emergency. But that is treated initially with oral antibiotics to get it under control which gives us time to decide how to further manage it if needed.
13) You will need to be clean shaven the day of surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, does clavicle lengthening push the shoulders out and back or just out? It seems like if the scapula was pushed back as well as out, this might put it in an awkward or unnatural position with enough added width. Is this something to be concerned about?
A: In regards to clavicle lengthening, since the clavicle is not a completely horizontal linearly shaped bone, expanding its length will have primarily a horizontal movement but also a bit of an outward movement as well. This is not of any functional concern and actually adds to the aesthetic benefit of shoulder masculinization. This is the opposite effect in clavicle reduction…the shoulder move inward and rolls in a bit…which also causes no functional issues and has an aesthetic benefit for a shoulder feminization effect.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I got a chin reduction and it left me with a bit of a bulbous Witch’s Chin which seems slightly off center. I’d be interested to understand if there is a way to refine the bone underneath the chin to give it a slightly thinner and more square appearance like I used to have.
A: If you had any form of intraoral chin reduction by bone removal, this is exactly what I would anticipate to happen….the soft tissue chin pad sags because it has been released from the bone and has lost structural support. As the front end of the bone has been burred down it will also look flatter/wider. The only method to address both issues is a submental approach where the bone can be tapered and the soft tissue excess can be removed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in buccal lipectomy and perioral liposuction surgery.
- Have you ever had any complications with these surgeries?
- Everything of course comes with a risk – which ones are the most likely once with these procedures?
- Knowing this is a very sensitive area with a lot of important facial nerves, and with anatomy not being an exact science but rather coming with certain individual differences to each patient – do you feel confident going through with these procedures? I have a great respect of the face anatomy 😊)
- Would we be able to do it with just local anesthesia? Not a big fan of general anesthesia (quite scared of it 😉), did my rhinoplasty without it and that worked great. I’m a tough cookie and are really still and tractable – eager to do what’s needed for the best results.
- How does the aftercare process look like? Is it something I need to think about beforehand?
A: In answer to your questions about buccal lipectomy and perioral liposuction:
1) I have not had any complication with these surgeries such as infection or nerve injuries.
2) The only real risk is in how much of a facial slimming effect could it have.
3) There actually are no ‘important’ nerves in the buccal space or perioral facial region.
4) it could be done under local anesthesia.
5) There really is no after case that is needed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My objective with surgery is to look more attractive. I talked to one surgeon in my area and he suggested orthognathic surgery treatment. What is that and is that sometime you offer? Thank you
A: Orthognathic surgery is jaw surgery done for the primary functional purpose of improving one’s bite relationship. It is not done to change aesthetic facial proportions or improve one’s level of ‘attractiveness’ although in some cases there may be some aesthetic facial improvements if the imbalance is caused by skeletal disharmonies from the misaligned bite. I see no obvious benefit of this issue in your case based on pictures alone.
What you really have is some facial imbalances caused by a shorter lower jaw and a midfacial flatness. By proportion your nose is also larger. As shown in the attached imaging creating a more projecting and stringer lower jaw combined with rhinoplasty and infraorbital-malar augmentation can provide a male facial masculinization effect.,,,.which what I think you mean by being more attractive.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley ,I have small shoulders and all the workout I do, doesn’t help. I want to increase of +/- 3cm each side my shoulders with mplants and not fat transfer.I wonder if you can reach this result. Thank you
A: Thank you for your deltoid implants inquiry and sending your picture. For deltoid/shoulder augmentation fat grafting was never an option for you due to your very lean body frame. You have correctly identified deltoid implants as the most viable option for your shoulder augmentation. Given your also leaner upper arms I would think that a 3 cm wide deltoid implant would be too big and disproportionate to the rest of your arms and chest width. Deltoid implants in the 1.5cm to 1.75cm width would appear to be more proportionate for you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m strongly considering going ahead with the cheek implant and vertical orbital dystopia (VOD) correction this year. I have a few important questions.
1) You said we can address the VOD at the same time as the cheek implants. I’m still deciding if I should do that, or just the cheek. Based on measurements on the CT scan/implant design, I guessed that my right eye socket and cheek are approximately 2mm lower. Could you possibly look at my CT and tell me the exact amount of this asymmetry?
2) It is possible to mitigate the eye asymmetry rather than completely correct it? Because my right brow is also lower, I’m concerned about the effect of pushing my eye up without pushing the brow bone up. I’m wondering if “something in between” might be a better solution? Half the current eye asymmetry will not be perfect, but it will likely be unnoticeable.
3) Is there a significant chance I will need more revisions on the eye structures? Or could this go wrong and create a negative outcome? To me (as a non-expert) it seems quite complicated to adjust the eyelid (ptosis repair), adjust the lower eyelid, and the position of the eye, all in unison.
4) How hard is it to get the cheek implants properly placed compared to the jaw implants? I.e. what is the chace I will also need a revision of these?
A: In answer to your questions:
1) In looking at your 3D CT scan, it was taken just high enough up that it includes the woes half of the orbits which is sufficient for vertical orbital dystopia (VOD) assessment and implant design. It is evident that the right orbital floor and infraorbital rim is lower and I would estimate that 2.0 to 2.5mm is the amount. That would correspond with what is seen externally. (see attached)
2) You are correct in that in the treatment of VOD one has to always consider the position of the overlying structures of the upper eyelid and brow bone as you don’t want the eye to become buried under the upper eyelid or look disproportionate to the brow bone. But more commonly the aesthetic ‘culprit’ that must be considered is that of the lower eyelid. Increased scleral show (iris moves up but the horizontal lower lid level remains the same) will always be more easily seen. This is addressed by both elevation of the infraorbital rim by the implant design as well as a lateral canthopexy and possibly lower eyelid spacer graft.
3) In my experience about 30% of VOD surgery patients undergo a revision of one of the eyelids later. But that depends on the extent of the original problem and the magnitude of the surgery done to treat it.
4) Orbital, cheek and combined orbital-cheek implants have a lower rate of implant revision because of more direct visualization of their placement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a CT scan of my head after skull implant surgery. Is it a 3D CT scan and what does it show?
A: I have reviewed the CT and can make the following comments:
1) It is indeed a 3D CT scan which has beautiful images of her skull and the implant on it.
2) The implant is perfectly positioned and, IF one was just looking at the 3D CT scan, the head with the implant shows a good shape.
3) Having an implant in place and knowing its aesthetic outcome is a huge advantage in knowing how to get a more desired head shape. This is not the advantage we have the first time whether the implant was custom made or chosen from a stock design.
4) In making a new implant shape for a more desired aesthetic result, you can take tracings of the side profile and draws what you think is a better shape in both the side and front/back views. That is the information I need to start a new design. Or take the side pictures of your self and draw what is a better profile head shape.
5) The good news is that replacing the existing implant has a much better recovery as much of the pocket already exists.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have several questions/comments about facial asymmetry surgery I would like for you.
1. While this is not out of my budget, I am curious if insurance would cover part of this surgery? I imagine that most plastic surgery is considered cosmetic and thus not covered, but would this be a case of reconstruction since I am doing this to fix asymmetry/deformities in the facial area? I was researching online and saw that reconstructive surgeries may be covered, but was instructed to first contact the doctor and ask.
2. You asked me during our consultation to make a list of the features that bother me most about the facial asymmetry. While the cheek volume is still certainly the top priority, a close second would be the asymmetrical mouth and eyes/eyebrows. The third feature is the uneven asymmetrical eyes/eyebrows. That said, I am curious about pursuing those as well.
I also understand that you may advise doing just the cheek first, and then the mouth at another time, as that may be a lot of features to target during one operation. On the flip side, it may save a lot of time, which is why I wanted to ask.
A: In answer to your facial asymmetry surgery questions:
1) I do not participate in any health insurance plans so I can not say what insurance may or may not cover.
2) I will need to the 3D CT scan to determine the bony anatomy from which I can then address what may need to be done for the cheek, eyes and eyebrows. Since the shape and position of the mouth is not a bony structure any adjustments of its corner would be a soft tissue based procedure such as a corner of the mouth lift.
3) Most facial asymmetry surgery usually takes a comprehensive approach (multiple procedures at once) as opposed to separate surgeries for each issue.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had my chai implant shaved about 6 weeks ago. I have been patient with the healing and for the most part, it has been uneventful. As discussed, I hate the outcome. However this question pertains to the healing.
I have had a slightly uncomfortable nerve like feeling on under and around the chin. A few weeks back, it felt like a burning feeling almost like bones have been scraped. I am starting to wonder if I have slight damage to the mental nerve. Is this sensation common with a shaving and does it go away? It can also feel almost like an arthritic feeling I get in my bad knee.
Getting ahead of myself. If I have slight nerve damage from a shaving, what can I expect with a replacement? Again, I am trying to make sure that I do not make matters significantly worse trying to correct my shaving mistake.
Any insight would be appreciated.
A: Such mental nerve changes are typical from it being stretched, which would be common when trying to perform a shave in a limited and tight tissue pocket. Depending upon how close the implant is the mental nerve and where it is attached by scar tissues, I would expect such nerve changes to be significant when doing a replacement. In most cases such mental nerve changes are temporary and self-resolving over time….which could be as long as 3 to 6 months after surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hey Doctor, I saw your instagram post about shoulder widening by clavicle lengthening.. I had a question about lengthening the clavicles.
If I remember my anatomy correctly, the clavicle is connected to the upper part of the scapula. How does clavicle lengthening contend with the position of the scapula? Put another way, how do you create the space to widen the clavicles, so to speak? Does the scapula move outward when the clavicle is widened or do the clavicles adopt a more inwardly slanted position to make room for the added width? Is it something else I hadn’t considered?
Speaking of which would there be any performance loss (athletic/range of motion/load bearing) after the surgery was complete?
Pardon my lack of knowledge on this subject. It seems like an excellent surgery, I’m just not certain of the ramifications of expanding bones in that way.
A: The clavicle is connected to the scale by the acromioclaviclar joint.The clavicle pushes out the scapula some what no differently than when you pull your shoulders back. The end of the clavicle pushes on the acromion process of the scapula across the joint interface.
Dr. Barry Eppley
Indianapols, Indiana
Q: Dr. Eppley, I came across the below case studies on your website and would like to find out more about these procedures?
https://exploreplasticsurgery.com/case-study-testicular-enlargement-with-specially-design-implants/
https://exploreplasticsurgery.com/plastic-surgery-case-study-scrotal-enlargement-with-custom-testicular-implants-in-a-side-by-side-technique/
I have been on testosterone replacement therapy for the last ten yrs which has unfortunately caused my testicles to atrophy. From 5cm down to 2.5cm which now looks very unsightly. I have researched extensively but our local doctors cannot help me with testicular enhancement surgery. So I’ve decided to search abroad and hope you can assist?
I have a few questions:
1) What is the estimated all-in cost for consultations, surgery, hospital costs, cost of testicular implant prosthesis (wraparound implants, and standard oval implants) and any other costs?
2) Given that my natural testicles are small 2.5cm would the side-by-side (prosthesis together with natural) option be better than wraparound implants?
3) Is the side-by-side option with standard implants cheaper?
4) What are the risks involved and what % success have had with these type of surgeries?
5) Are there any long term complications with wraparound implants as they encase the natural testicle. Does the silicone shell not eventually adhere to the natural testicle?
6) How long does the procedure take and what is the typical recovery period? How long would I need to stay in Indianapolis before I could fly back home?
 A: In answer to your testicular enlargement questions:
A: In answer to your testicular enlargement questions:
1) My assistant Camille will pass along the cost of the surgery to you.
2) Given the very small size of your testicles, the best option would be side to side with new implants of 5.5 or 6 cms size.
3) Standard testicle implants are more cost efficient than custom ovals or wrap around designs.
4) The only real risk is infection….which I have never seen yet. With the wrap around method I have seen one case of chonic fluid buildup on one side. But no such occurrences in the side by side technique as the tunica albumin is not disrupted.
5) Given your testicular size you need to stay focused on the side by side technique and forget about the wrap around method.
6) This is a one hour surgery.
6) You should be able to return back home in a few days.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, When you have a Medpor implant and remove it after 5 years, will the face come back the same as when you didn’t have it?
A: That would depend on many factors such as facial implant location and size and style of the implant. But as a general statement it is not likely to return to exactly the way it was before the implants were placed as the tissues have been elevated off of the bone and stretched out. It is more a question of how closely will it get to the pre-implant shape but a complete return is to likely.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m interested in having facial implants surgery. As you can see from my photos, I have flat cheeks and hollow nasal base. I actually had paranasal implant surgery two years ago but I realized the thickness of the implant is not enough. (5mm) Before I read your articles, I was only considering having cheek implant and pyriform implant separately to make more volume to my midface. But I just saw another option on your website that is having custom facial implant which can cover cheek and nasal base areas together.
Could you give me advices on which approach I should take to make my midface better looking. And I would also like to know the cost and material used of each approach.
Thank you very much and have a good day.
 A:You are referring to what is known as the Midface Mask Implant which can cover the entire midface and provide complete anterior projection. For the patient with a flatter midface development this is a more anatomic and effective approach to the problem than traditional ‘spot’ implants which only augmentation smaller areas of the problem. By having existing paranasal implants in place you have some good knowledge as to what dimensions of the implant may be effective at the lower nasomaxillary level. Such an implant is made from the patient’;s 3D CT scan of which solid silicone is the most versatile material that permits a completely intraoral approach for its placement.
A:You are referring to what is known as the Midface Mask Implant which can cover the entire midface and provide complete anterior projection. For the patient with a flatter midface development this is a more anatomic and effective approach to the problem than traditional ‘spot’ implants which only augmentation smaller areas of the problem. By having existing paranasal implants in place you have some good knowledge as to what dimensions of the implant may be effective at the lower nasomaxillary level. Such an implant is made from the patient’;s 3D CT scan of which solid silicone is the most versatile material that permits a completely intraoral approach for its placement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Overall, I am looking for sharp angular model-like features.
As in the custom jawline implant design:
1) Is the chin square?
2) I am unsure of the exact terms to describe the features I am looking for, but I would like the resultant jaw to be square, sharp, and chiseled.
3) I would like this sort of square jaw angle if possible/suitable.
As in the custom infraorbital-malar-maxillary implant:
4) I would like a bottom part to the implant covering the area to make it into a full mask implant in order to get as much forward maxilla/midface projection as possible (within your guided measurements) to get that Lefort effect. Such as in these examples:
5) I just wanted to make sure the zygomatic arch part of the model cheekbone is included as there are different lengths on different skulls shown on the website. Not sure if there is any difference on the lengths and the cheekbone effect.
6) I would like zygos/cheekbones with both forward and lateral projection meaning I would like to add slightly more forward projection to the zygomatic area (if possible/appropriate).
7) I have concerns about removing a Negative Orbital Vector and negative canthal tilt, just wanted to ensure that the implant will tackle this.
8) As I believe the custom midface implant is going to be inserted through the eyelids and closed using a lateral canthopexy and we are using spacer grafts to lift the bottom eyelid – is it possible to change the outer corner of my eyes slightly to fix their asymmetry and eliminate excessive scleral show and to give the eyes a slightly positive canthal tilt or “as almond as possible”?
9) Reading anecdotes from others who have gotten infraorbital rim implants is that though the support under the eye is a significant improvement but there is still a bit of hollowing due to the lack of fat under the eyes – is there a solution to this such as under eye fat bag repositioning or fat pocket transfer? Is it possible to do it at the same time as adding the spacer grafts? Should it be done post implant healing? Could it be recycled fat from the buccal liposuction?
10) I would like to get my whole mouth area improved – this includes mouth widening, lip corner and lip projection. I asked you asked about this via email and you said I would need to wait a minimum of three months post jaw surgery. As I believe this can be done under local anesthetic, I believe seeing you in person will be the best gage on what to do with that. Same thing with a possible fat transfer to the upper eyelid area. I’m not sure if I have Ptosis of the eyelids or not – can this be evaluated in person and done under local anaesthetic at another point in time as well?
11) In case there is emergency, should I have a local surgeon kept in the loop about the surgery before I go to the states?
12) What should I do in case I believe there is an infection or something wrong?
13) Do I need to clean shave for surgery or is having a light beard okay?
A: In answer to your custom infraorbital-malar-maxillary and jawline implants:
- The current design of the custom jawline implant has a square chin. Whether it should be more sharply square in the design can be debated.
2) The ability of any custom facial implants design to show through depends on the thickness of the overlying tissues. Thinner facial tissues allow these designs to show their defined designs, thicker facial tissues do not. So the patient has to appreciate what is possible within the limits of their own facial tissues.
3) The squareness of the jaw angle design must be considered very carefully. If it is over squared on the design the implant can protrude beyond the posterior edge of the masseter muscle causing what is known as implant reveal, an aesthetic deformity.
4) A midface mask implant design can replicate a LeFort-like effect but a more complete one.
5) A zygomatic arch component can be added to the design to go back as far along the arch as aesthetically desired.
6) Forward and lateral projection at the zygomatic area is common in these implant designs.
7) A custom infraorbital-malar implant is the most effective approach to correction of the negative orbital vector and negative canthal tilt.
8) Such an infraorbital-malar-maxillary implant can NOT be solely inserted through just the lower eyelid incisions. This will need to be combined with intraoral incisions as well. In addition, while the implant may be designed as one-piece, it can neither be manufactured as one piece nor inserted as one piece. There would be a split in the implant design at the level of the infraorbital-malar and maxillary portions to allow both manufacture and surgical placement. But it will fit together int surgery like a puzzle piece.
9) Recycing the fat from buccal lipectomies for additional volume augmentation over the infraorbital area can be done at the same time. But the risk of infection is increased since the vascular fat grafts are placed on top of an avascular implant surface.
10) With the stretch on the lips from the surgery delicate soft tissue procedures such as mouth widening are not advised at the same time. Postoperative facial swelling will adversely affect the appearance of the resultant lip/mouth scars.
11) There really won’t be an emergency per se.
12) Infection is the only real semi-emergency. But that is treated initially with oral antibiotics to get it under control which gives us time to decide how to further manage it if needed.
13) You will need to be clean shaven the day of surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have some questions regarding facial slimming with buccal lipectomies and perioral liposuction. I’m interested in doing the procedures and I’m wondering if you think that you could help me with this. To give you the full background:
I’ve previously had some treatments done in my face in order to shape it in a pleasing way. I used to have so called “hamster cheeks” and where really heavy on the lower face (think reversed egg ) – so I’ve had cheek implants done and have had a buccal fat pad removal that resulted in success on the left side, but still with fat remaining on the right side, leaving the face to be uneven.
The reason why the plastic surgeon didn’t succeed on both sides is due to the buccal fat on my right side being scattered around (at least that’s what he told me).
So if possible I’d love to have the left and the right side be symmetrical (as much as possible, as I know this isn’t an exact science) – do you think it would be possible to “go in” on the right side again and correct it? Knowing it’s a very sensitive area with nerves etc.
I can also start seeing droopiness on the perioral mound area (the side of the mouth) due to excess fat – making me look sad when I’m really not. So this is something I really like to get rid of. I’d like to correct while the skin still heals an bouncing back easily.
A:Thank you for your buccal lipectomy and perioral liposuction inquiry. I have never seen or heard of the buccal fat pad being ‘scattered around’ as that is not how it is anatomically located. I suspect he just wasn’t able to locate the buccal fad capsule as it is often deeper than what most surgeons think it is. Thus trying to ‘redo’ one buccal lipectomy side which seem appropriate. But on both sides perioral liposuction can be done to complement the buccal lipectomies and provide some further facial slimming effects.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested I knowing more about the iliac crest reduction procedure. What is the healing process like for an iliac crest reduction? What are some of the potential risks? What does pricing look like?

 A: In answer to your questions about iliac crest reduction:
A: In answer to your questions about iliac crest reduction:
1) The maximum width of the iliac crest is due to its convexity where is greatest at its middle third. (see attached) It is this area that can be reduced which is about a 9 to 10cm length segment of 1 cm thickness. Most of the significant muscles that attach to the iliac crest are located more at the anterior and posterior iliac spine areas which are not in the bony area of removal. It is necessary to remove some of the attachments of the tensor fascia lata (TFL) but its muscular portion remains intact as it is located at the anterior iliac spine area.
2) In many ways the recovery is similar to an iliac bone graft harvest with the exception that it is bilateral. Reading about iliac bone graft harvesting recovery will provide good insight. The most difficult part of the recovery is in the discomfort in walking which takes some time to recover.
3) The risks of the surgery are the incision/scar, contour irregularities and chronic pain
4) My assistant Camille will pass along the cost of the surgery to you tomorrow.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, How much would an orbital box osteotomy cost for eyes that are too close together performed at your clinic? I am extremely motivated to have one, because my face is dramatically disharmonic due to this defect: my interpupillary distance is only 5.9 cm, my intercanthal distance is shorter than an eye breath and my face appears long and narrow. What are the effects of such an operation in the cheekbones area? Thank you,
A: Thank you for your inquiry. The most important issue to recognize about orbital box osteotomies is that they require a frontal craniotomy to perform. As a result the following sequelae exist: 1) a full coronal scalp incision is needed, 2) it must be performed in a hospital with several days of stay, and 3) there will be resistant bony irregularities/edges n the cheek and forehead areas around the osteotomy sites where secondary revisional surgery is likely. All of this together means it is highly expensive (patients only do it through insurance) and there are aesthetic tradeoffs that one must consider very carefully. This is why this is a procedure that is almost always only performed in craniofacial deformities where the magnitude of the deformity justifies the aesthetic tradeoffs and surgical risks.
I would need to see pictures of your face to determine how the above statement falls in line with the extent of your inter orbital concerns.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was told that implants can be added to the scapula to assist in shoulder broadening. I am curious about the mechanics of this.
Is the implant placed under the cartilage at the shoulder joint, meaning that the humerus will attach farther out from the body, or is it merely placed at the acromion and broadens the shoulder from above the joint?
Both, neither? Does it have any long term impact on shoulder function? I’m curious to know a little bit more about this procedure.
A: I am not certain where your information comes from about scapular implants as they do not have an effect on shoulder widening per se. They are placed in the subscapular fossa underneath the posterior deltoid, teres and infraspinatus muscles. Their purpose is to augment the fullness to the posterior shoulder area not to widen it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had otoplasty surgery done as well as an earlobe reduction a few years ago and then returned a few months later to have a revision done on the pinning of my ears. I can see a difference, but slowly the tops of my ears have gone back and continued to stick out and make me feel insecure. I am wondering if I have another revision done, what are the chances of it holding this time? Can it be done under local anesthesia?
In the pics you can see the tops of my ears stick out- not terribly, but enough to bother me. I would like for them to be pinned closer to my head & in (forward) Also, if we could make my earlobes more detached. I took some pictures of how I would like them to look when I shape them with my hand. Hopefully all of this makes sense, and If you need other photos I would be glad to send them. Thank you for your time and I hope to hear back from you soon!
A: Further improvements can be done to setting back the top of the ear through revisional otoplasty. But if the traditional cartilage suture techniques did not hold over time, a more ‘aggressive’ technique would be needed which involves suturing the cartilage to the temporalis fascia with skin removal.
Detaching the earlobes from the face further involves deepening of its inverted-V shape attachment by skin release.
Both procedures can be done at the same time under local anesthesia.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I recently made a post on Real Self, about the possibility of reduction of the iliac crest. You response was very helpful, and you said focusing on the augmentation of the hip was probably a better idea. I am still curious if reducing the iliac crest is possible? I want talk more about that. I find that even if I get a hip augmentation, my pelvic area squares me out too much, making my waist area non existent. I look forward to hearing back from you.
A: I would not disagree that your iliac crest bone position is actually the ‘problem’. Hip augmentation is a camouflage approach for making the iliac crests appear less wide and was only suggested because it is a less traumatic procedure. But I would agree that it is actually not the best procedure. Iliac crest reduction can be done but the incisional burden to do it and the postoperative discomfort from it makes it a questionable aesthetic procedure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, If the clavicle is lengthened by an inch on each side, does that translate into two additional inches of broadness in the shoulders, or is the actual gain in width reduced somewhat by the slightly inward pointing, S-shape of most people’s clavicles?
Related question. Can this procedure be used to create straighter clavicles?
A: Since the clavicle is not a completely horizontal bone, there is roughly a 110% correlation between bone lengthening and shoulder width increase. Conversely the opposite is true in clavicle reduction…there is a 90% correlation between the bone removed and the reduction in shoulder width.
Because clavicle lengthening is done an s-shaped curved bone, changing its length does not alter its shape. In short you can not make a clavicle a straight bone.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, How much does back of head surgery cost? I also have indentations on the side of my head. Not sure what caused it, but I suspect some kind of bone loss and it really bothers me. the back part more than the sides. Do you use OsteoBone?
A: 1) If you want to use OsteoBone this will require a large scalp incision to place and contour, known as a full coronal scalp incision from ear to ear across the top of they head
2) Using custom skull implants made of solid silicone these can be placed with much smaller incisions, usually a low horizontal one of less than 9 cms on the back of the head.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, How much time will the custom wrap implant take to settle (heal)? How durable are the implants(what if some hits me hard or I fall down)?
A: In answer to your custom jawline implant questions:
1) The setting or healing from a custom jawline implant involves multiple phases which to the patient is only judged by what they see on the outside. The worst of the swelling takes about three weeks to subside but full healing and judging the final results takes up to three months after surgery.
2) The material used is permanent, will never break down or degrade and will never needed to be replaced due ti material failure. The material is impossible to fracture or break due to trauma and thus it is like putting a bumper on the jawline…which makes it very difficult to develop a jaw fracture later from just about any amount of trauma.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley: I understand that with this type of osteotomy, the shoulder broadening effect is capped at about two inches.
Would undergoing this procedure now mean that I am unable to undergo any further broadening of the clavicle later in life as the technology progresses?
As an extension to that, can the surgery be undergone twice? Is the broadening effect capped at two inches at a time, or two inches total?
A: Your question is a good one but there is not a known answer because it has never been done or requested. You are correct in that clavicular lengthening is done at 2 cms per side due to the need to have bone grow across this bone grafted site. Once healed it would be fair to assume that further lengthen could be done later but I can not verify that based on personal experience. But you are also correct in that technology will advance and there is no reason not to believe that larger and secondary clavicle lengthening procedure will be done in the future as the technology advances.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am strongly considering getting a custom jawline implant.
I have a few questions, the first is: will I be prescribed painkillers afterwards or is it possible to forego this?
Also, how long would I need to be out of work after this procedure? Could I get any sort of doctor’s note and do employers usually recognize this as medical leave?
Would there be any sort of discount to get cheek implants put in at the same time? I assume the cost of getting anesthesia once rather than two separate times (once for jaw, once for cheek) would save some money.
Finally, how far in advance does this need to be planned? I get my schedule only one month in advance. It’s not a big issue because I can potentially move things around or call out sick, but just wondering.
Also, I know costs vary but can you give me some idea of the cost of a custom male chin and jaw implant and also the cost of a custom cheek implant?
Also, I know this is an even more speculative question but what are the chances someone could go from average appearance to “attractive” or “hot” with these types of surgeries?
Thank you,
A: In answer to your custom jawline implant questions:
1) The use of narcotic medications after surgery is optional.
2) How much time you will be off work is highly dependent on your facial appearance. Most patients probably don’t truly feel comfortable being seen in public for 2 to 3 weeks after surgery.
3) Doing multiple procedures is always more economical than doing them separately.
4) My assistant Camille would know better about the scheduling process as well as the cost of the surgery.
5) The interpretation of appearance change from any type of cosmetic surgery is as a highly personal one in which I could not provide a quantitative answer based on a theoretical question.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am planning on skull reshaping surgery with reduction on my head in the future and am wondering is it possible to have both sagittal and temporal reduction and how much of a difference does it make on the head? Also do you have to shave your head for the procedure? Another question I had is are is procedure out of pocket.
A: In answer to your skull reshaping surgery questions:
1) Both sagittal crest and temporal muscle reduction surgeries can be done at the same time.
2) It is not required to shave your head for the surgery.
3) To preoperatively determine the effects of the surgery I always try to do computer imaging. That can be more challenging with a full head of hair but there to do so still has value.
4) The procedure would be out of pocket as I do no participate in any health insurance plans
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m interested in a custom forehead implant as my brow should look much better with a bit more projection. My forehead has to much backward slope and it is narrow. Perhaps I would also need custom temporal implants or fat grafts, but I’m not sure. My biggest concert is that it looks natural and, for example it is not too curved towards the midline, mantaining a natural shape for the glabella, temporal ridges and orbital rims. I have also the concern for permanent numbness or long-term complications due to the implant material.
A: Thank you for your inquiry and in answer to your custom forehead implant questions/concerns:
1) Permanent forehead numbness is not a problem that I have seen in any patients who has reduced custom forehead or custom forehead-brow bone implants.
2) The key to having any custom facial implant achieve a natural look is to not overdo any of its dimensions. Getting a good shape is achieved through 3D computer design looking at all angles to ensure that it has a natural flow into the surrounding facial features.
3) I would need to see some pictures to do some computer imaging for a better idea as to the type of result you are seeking.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello. Is it possible to completely augment the front of the face. Just front of the face like the complete maxilla. See attached example. So I need infraorbital and complete front of face down to and around the nose and nasolabial area. Can you do that? What material would you use?
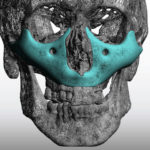
A: Yes it is possible to augment the entire midface from the infraorbital rims down and around the nose. This is what I call the ‘Midface Mask Implant’. It is best made of solid silicone which allows it to be placed from a completely intraoral approach in most cases. It is important to place perfusion holes into the implant to allow for tissue ingrowth between the midfacial soft tissues and the underlying maxillary bone.
Dr. Barry Eppley
Indianapolis, Indiana