Your Questions
Your Questions
Q: Dr. Eppley, Good afternoon, I have a chin implant from about 34 years ago. It was done when i was a teenager. It was made out of cartilage. I would like to have it replaced. Could you please advice on different options?
A: Thank you for your chin augmentation inquiry and sending your pictures. The piece of lyophilized cartilage you had placed was likely very small and many even be in the soft tissue and not down on the bone. The small size of the implant is reflected in how your chin looks today in profile which is still fairly recessive even with a graft in place.
Your options for secondary chin augmentation depends on how much change you are seeking in the profile view as well as what shape you want in the frontal view. I will work on some imaging and get that back to you tomorrow to see what degrees of change you prefer. But based on what I am seeing in your pictures a standard chin implant would seem to suffice.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have orbital bone asymmetry that I am looking to correct. Your website shows similar case in another patient that was able to be correct. I live out of state from your location and am trying to look into pricing for this procedure and also how to plan for an out of state procedure.
 A: Thank you for your inquiry and sending your picture. You have a left vertical orbital dystopia. In such cases the ideal approach is a custom orbital floor/rim implant made from the patient’s 3D CT scan. Such a scan will help also determine if the magnitude of the deformity requires a true custom implant or whether another material, like hydroxyapatite cement, could be effective by intraoperative placement and shaping. With this orbital bone augmentative approach, many times eyelid adjustments may also need to be done as the eye raises up.
A: Thank you for your inquiry and sending your picture. You have a left vertical orbital dystopia. In such cases the ideal approach is a custom orbital floor/rim implant made from the patient’s 3D CT scan. Such a scan will help also determine if the magnitude of the deformity requires a true custom implant or whether another material, like hydroxyapatite cement, could be effective by intraoperative placement and shaping. With this orbital bone augmentative approach, many times eyelid adjustments may also need to be done as the eye raises up.
The 3D CT scan can be obtained where you live and you can then mail the disc to me for review. My assistant Dawn can provide information as how to find an imaging center close to you. Once an imaging center has been located, we will fax the order to them for you to get it done.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in fat injection for bony shoulder / separated ac joint. I am curious also about what I should do to prepare for such a thing, for example which muscles to work on, etc
A: I assume you are wanting fat injections over the AC joint to mask its prominence after the separation. If so there is no need for any preop muscular training. Fat injections are done to build up the soft tissue around the bony prominence. Thus there is no benefit to either deltoid or trapezius muscle exercises which like to the side and behind the AC joint.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had infraorbital rim implants placed 6 weeks ago, and my cheeks (especially the right one) still looks pretty bloated. The thing is that I only had about 1.5mm-2mm of augmentation. Additionally the area below my eyes is still badly discolored (reddish, blue etc.) and it’s not noticeable improving day by day. My doctor tells me that the under eye area is very delicate and it takes a long time for the swelling/bruising to resolve. However, based on your posts it seems that most swelling should resolve by six weeks. So here are my questions:
1) how long should it take for the bruising to resolve? At the rate I’m going now it feels like it’ll be months
2) at six weeks am I in a position to accurately judge the outcome, or is there still a material amount of swelling that will go down?
3) if I’m unhappy at the end, how long do I have to wait to get them taken out or replaced?
4) will the recovery for taking them out be as long as the initial recovery?
5) if I get them taken out, will the implants have created a pocket that will prevent my face from returning to how it was before?
Thanks a lot
A: In answer to your infraorbital rim implant questions:
1) Whether the augmentation is 1mm or 5mms the amount of swelling and bruising will be the same.
2) It takes at least 3 months for all swelling and bruising to resolve in most cases. I would not pass any judgment on the aesthetic outcome until at least then.
3) If unhappy at three months out then you have the confidence to stay the effort was not worth it. You certainly don’t want to pull the plug before you really know what they look like and you have had time to adjust to them.
4) Recovery for removal or exchange of implants is always a lot easier than their placement….unless they are implants that have a high tissue adhesion. (e.g., Medpor)
5) It is fair to assume that any implanted site in the face or body is never going to return 100% to the way it was. It is only a question of how close to the preop state will it be.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to know which technique you would recommend if I want to make my forehead and my brow bone more like the photo illustrated below?
A: If I interpret your forehead-brow bone goals properly from your submitted pictures, this appears to be an augmentation of which only a custom implant design to achieve such. change predictably and smoothly. The complex topography and shape needed for a satiisfactory forehead brow bone augmentation is best done by a custom implant done by computer design on the patient’s 3D CT scan.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I want to reverse a sliding genioplasty I did over 2 years ago. Is it possible and what are possible complications?
A: Just like the way the original procedure was done, the same bone cut can be made and the bone moved back. (sliding geniplasty reversal) Because the soft tissue chin pad remains attached to the bone there is no risk of chin pad ptosis when the procedure is reversed unlike that of a chin implant.
Such sliding genioplasty reversal procedures are not uncommon and can be done either completely (total reversal) or only partially. (subtotal reversal)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a cranitomy ten years ago and a correction surgery of issues arising from the earlier surgery six years later. As much as the said surgery was successful, the surgeon removed a muscle on the right side of my head in what he termed as ‘wasted muscle’. As a result, I have bumps and depressions on the scalp. Further, the surgery affected hair growth which is scanty.
My query therefore is, is it possible to correct the bumps and depressions on my head/scalp. Also, is there a way I can have a normal hair growth?
A: Contour deformities are not uncommon after craniotomy surgery. While surgery can be improve the contour of the bone (get rid of the lumps and bumps through skull reshaping surgery) only hair transplantation can restore near normal hair growth in the affected scalp area.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m interested in the rib removal surgery for ribs 11 and 12. I’m wondering, do patients have any long-term pain associated with this? Have any patients ended up with nerve damage from the surgery or intercostal neuralgia? I’ve been told that that is a risk, so I’m wondering about the experience of your patients. And are patient able to exercise after having muscles detached from those lower ribs?
Doesn’t seem that there are many surgeons that are doing this, so I really haven’t been able to find any information or reviews from patients after having the surgery. Im very interested, but I feel like I want to know what their outcomes are like before committing to this.
A: Thank you for your inquiry in regards to rib removal surgery to which I can answer your questions as follows:
1) No patient has ever reported any long-term discomfort or pain from the procedure.
2) Similarly, no patient has had any intercostal neuralgia now would I ec pe t them to as the intercostal nerves, which run on the bottom of each rib, is preserved.
3) All patients can return to full activities after the surgery whenever their comfort level for doing so permits.
4) In terms of aesthetic outcome (improved waistline shape/reduction) that is the most important criteria I try and assess before surgery. In other words, based on the patient’s goals can the surgery have a chance to be reasonable successful.
5) For more definitive information on this topic I would refer you to www.exploreplasticsurgery.com and place in the search box the term Rib Removal. There you will find a lot of information about the particulars of the surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I can’t help but feel that my lips are excessively “pouty” or too thick. It’s as if to me my entire lip structure juts out too much and overpowers my face. I don’t know if this is due to weak facial bones or it’s just because my lips are too big. Is there a way to do a full thickness lip reduction without causing disfigurement?
Will making my nose longer and jaw and chin bigger cause my lips to appear smaller? (This would be a positive change in my view).
A: Lip reduction is a common procedure and generally reduces lip size by about 1/3. If facial features around the lips get bigger by definition the lips MAY appear somewhat smaller.
Dr. Barry Eppley
Indianapolis, Indiana
Do I Need To Dissolve Any Injectable Fillers Before Getting A 3D CT Scan For Custom Facial Implants?
Q: Dr. Eppley, I see that a referral for a CBCT has been made at my local clinic and I’ve made the appointment on Feb 3rd. My questions are:
1) How long is this CT scan valid?
2) Do I need to dissolve the fillers in my face first?
3) How are the custom facial implant designs sessions done?
A: In answer to your custom facial implants questions:
1) The 3D CT scan would be valid forever as long as the bones inside have not been changed.
2) You do not need to dissolve any injectable filler that is present.
3) The implants are designed in a virtual/electronic manner.
Dr. Barry Eppley
Indianapolis, Indiana
 Q: Dr. Eppley, If you were to look at a side view x-ray of several different Caucasian women, how far forward would the maxilla extend from the eyes?
Q: Dr. Eppley, If you were to look at a side view x-ray of several different Caucasian women, how far forward would the maxilla extend from the eyes?
I have maxillary protrusion and would like to get a flatter/softer and less full mouth. I’d just like to get an idea of how many millimeters is within the normal range for a woman of Northern European descent. (horizontally not vertically, so from where the eyes sit to the most prominent point of the maxilla/front teeth)
I know the standard is to draw a vertical line from the forehead to the maxilla but if someone has an overdeveloped forehead and nose which are going to be reduced to soften the overall appearance, based around orbital projection, I’d like to know where the maxilla sits.
If you ever have time to take a look at a few random x-rays to get an idea, please let me know if you get the chance.
A: The question you are asking can not be determined by x-ray. You are demonstrating in the picture the vertical distance from the corner of the eye to the soft tissue lip position…neither of which is seen on an x-ray nor are there any anthropometric standards for that vertical facial linear distance.. Such soft tissue structures are only seen on pictures, x-rays can only show the bony infraorbital rim and the upper teeth.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a webbed neck and I would like to remove it because i don’t feel comfortable and confident at all.
A: Based on these two limited pictures what you appear to be demonstrating is not a true webbed neck but the posterior border of the sternocleidomastoid muscle. Unlike the traditional webbed neck which goes along the superior border of the trapezius muscle and can be addressed with a more hidden incision on the back of the neck, removing this anterior ‘web’ or posterior border of the sternocleidomastoid muscle requires a more visible anterior incision which would be considered a questionable aesthetic tradeoff.
Dr. Bary Eppley
Indianapolis, Indiana
Q: Dr. Eppley, you have quite rightly said the only suitable options for a bicep implant are the Implantech contoured carving block as I do not want to go down the custom implant route.
1) Why is CCB style 3 more suitable than CCB style 1 for sub-fascia bicep implants? Is just the feather edges that make it more suitable not it’s shape?
2) And do you tend to use CCB style 3 for subfascial bicep implants instead of CCB style 1 if the patient opts not to go down the custom implant route?
I do recognize that CCB style 3 already has feathered edges whereas style 1 would require a hand made feather edge to be made with a scalpel.
 A: In answer to your bicep implant questions:
A: In answer to your bicep implant questions:
1) The preformed featured edges of the implant are key. You just can’t hand carve those into the implant in any smooth and even fashion. That is why CCB style 3 is used as a standard bicep implant.
2) Also CCB style 3 has the maximum height centered on the implant which is how a bicep implant should be shaped. CCB 1 does not.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question about buccal lipectomies to which I could not find the answer online. Since you are expert on buccal lipectomy and other facial procedures I know you would know. Can the removed fat pads ever grow back once buccal lipectomies are done. I know fat can grow back or go to other areas after liposuction fat removal so I am wondering if it is the same for buccal lipectomy facial fat removal?
A: The buccal fat pads are a unique collection of fat whose role is not a metabolic one. Once the main body of the fad pad is removed it is permanent and will not return with weight gain. The small volume of the buccal fat pads (3 to 6ccs) is not significant enough to result in a visible fat redistribution effect. (fat homeostasis)
Dr. Barry Eppley
Indianapolis, Indiana
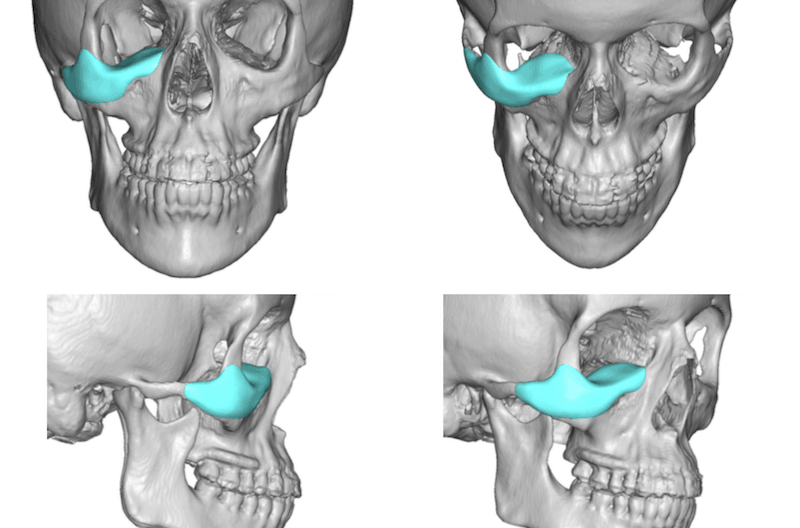
Q: Dr. Eppley, I like how I look from the front mostly (except for my bent nose), and from the left angle. But absolutely hate how I look from the right angle. Part of this is due to bad nose asymmetry. However, a large part of it also seems to be due to how my face is from the right structurally. I was wondering if I could get an infraorbital implant or something like that to maybe fix this issue? I had cheek implants along with other facial surgeries last year. And I actually like the results the cheek implants give from the front and left side and would really not like to remove them or change them if possible (but i’d definitely be fine adding to the under eye area or adding on the implants if that would fix the issue). Would it be possible to have this bad asymmetry/ugliness from the right fixed without altering my current cheek implants too much? Help would really be appreciated as fixing this issue is extremely important to me especially given how my cheek implants (although helpful overall) did not change this particular problem at all. I would also like to buy a lip lift along with whatever can fix this issue, depending on the price of the main treatment. Attached please find my photos.
A: Thank you for your inquiry and sending your pictures. Between your description of concerns and your pictures it appears that the issue is a right infraorbital deficiency. Short of a custom imply approach, the use of standard infraorbital implants may suffice. If placed through a lower eyelid transconjunctival incision the right cheek implant can be completely avoided. This can certainly be combined with a subnasal lip lift.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I wish to achieve a more square head shape around my temporal lines and get my sagittal ridge reduced. Can this by done with sagittal ridge reduction as well as a silicone skull implant?
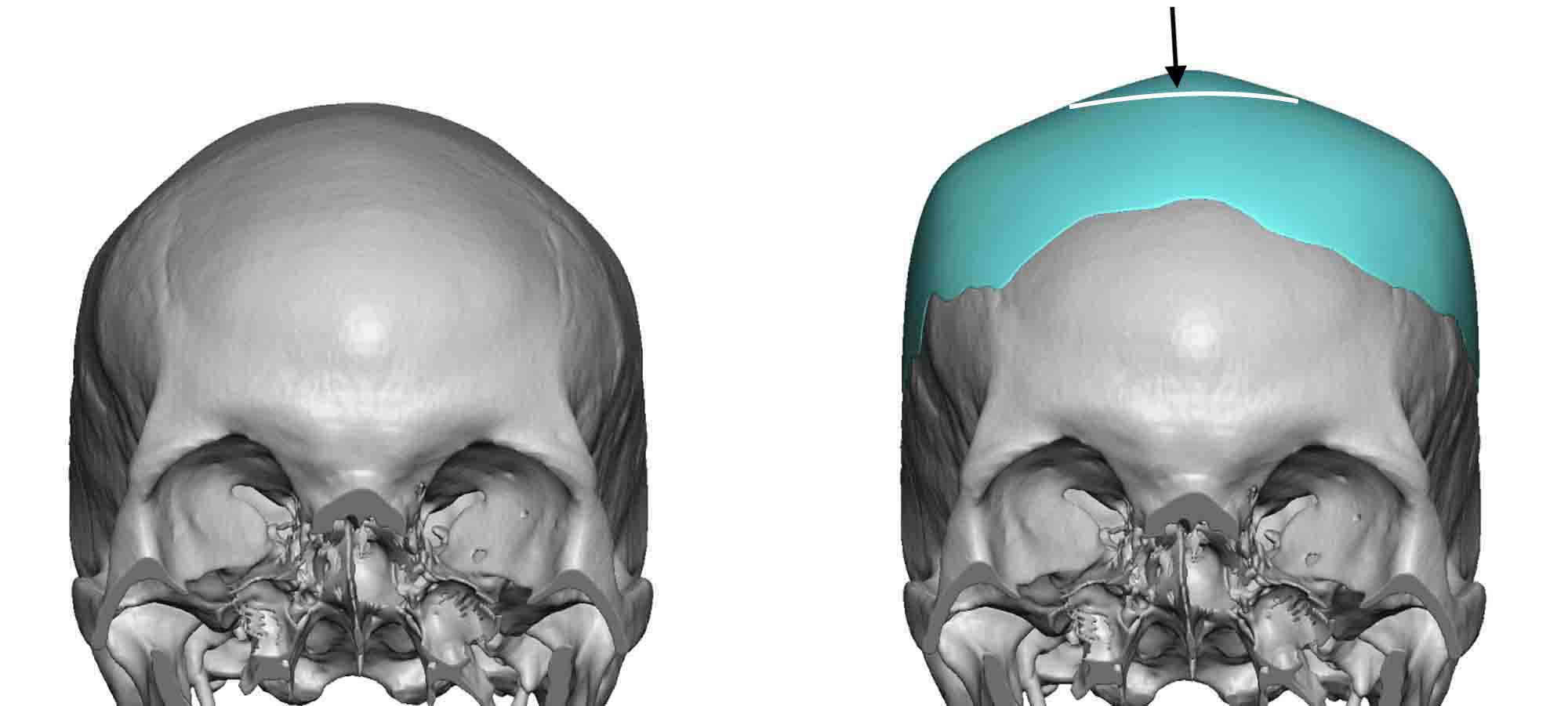 A: Thank you for your inquiry and sending your picture. The pertinent question is whether your sagittal crest is present because the parasagittal area to the sides is too low (not square) or whether you need a combined square-shaped custom skull implant with a sagittal crest reduction. You may just need a modification of the attached custom skull implant design to achieve your desired effect. It will take some computer imaging to help make this determination to compare how these two types of skull reshaping changes would look.
A: Thank you for your inquiry and sending your picture. The pertinent question is whether your sagittal crest is present because the parasagittal area to the sides is too low (not square) or whether you need a combined square-shaped custom skull implant with a sagittal crest reduction. You may just need a modification of the attached custom skull implant design to achieve your desired effect. It will take some computer imaging to help make this determination to compare how these two types of skull reshaping changes would look.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I want to have bigger testicles to fill out my scrotum. What are My options here?
 A
A : Thank you for your inquiry and sending your picture. The scrotal skin/sac has very elastic skin and for some men there is a great disparity between the size of the paired testicles and the scrotal soft tissue containment. To fill the capacity of the scrotum there are two testicular enlargement approaches….a side by side custom testicular implant placement which can hide the editing testicles or custom wrap around testicle implants which envelope the existing testicles. Each approach has its advantages and disadvantages and the exiting size of the testicles also plays a factor in the choice between the two scrotal-filling approaches.
: Thank you for your inquiry and sending your picture. The scrotal skin/sac has very elastic skin and for some men there is a great disparity between the size of the paired testicles and the scrotal soft tissue containment. To fill the capacity of the scrotum there are two testicular enlargement approaches….a side by side custom testicular implant placement which can hide the editing testicles or custom wrap around testicle implants which envelope the existing testicles. Each approach has its advantages and disadvantages and the exiting size of the testicles also plays a factor in the choice between the two scrotal-filling approaches.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a 6mm genioplasty but i dont like how it brought out the imperfections in my jawline. My side profile looks good and overall an improvement, but my chin is naturally weirdly shaped and my mandibles are inward so my jawline is not smooth. I want to look into maybe moving the genioplasty back 3mm and getting a custom jaw implant to make my chin more symmetric and smooth, as well as my mandible and full jawline.
A: What you have is a very common sequelae from sliding genioplasty which is a natural result of the geometric shape change at the front of the lower jaw. As the chin is brought forward the wider U-shape of the chin can develop a more pinched shape at the back end of the osteotomy lines. While his usually does not occur at just a 6mm bone advancement it can if the osteotomy lines are significantly angulated.
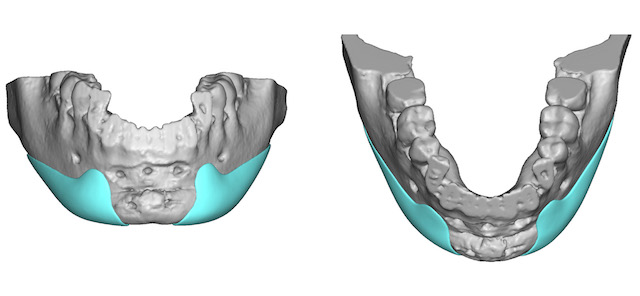 There are two approaches to smoothing out the existing inferior border indentations at the back end of the sliding genioplasty osteotomy lines. While certainly the sliding genioplasty can be reversed that would throw away any of the good aesthetic improvements you have obtained from the initial surgery. The alternative approach is to fill in the bony indentation which can be done by a variety of materials from standard ePTFE sheets to small custom interior border implants. (lateral chin implants)
There are two approaches to smoothing out the existing inferior border indentations at the back end of the sliding genioplasty osteotomy lines. While certainly the sliding genioplasty can be reversed that would throw away any of the good aesthetic improvements you have obtained from the initial surgery. The alternative approach is to fill in the bony indentation which can be done by a variety of materials from standard ePTFE sheets to small custom interior border implants. (lateral chin implants)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am looking to get an implant of the style provided by the picture that I have attached. (Medpor lateral and infraorbital rim implant) I have two questions about this kind of implant:
1) Is it possible to maneuver this implant to sit higher up on the face? You’ve made comments before about elevating the infraorbital rim with implants, is it possible to just shift an implant like this upwards; and then screw it in place, in the same fashion as is done with a custom implant?
2) Is it possible to actually fine-tune the shape of an implant like this by shaving certain parts in order to give more fullness in a particular area?
Thanks
A: I believe the framework of your question is whether to avoid making a true custom infraorbital implant can this preformed Medpor implant be used instead. The answer is yes with the following caveats:
1) There will be irregularities at certain points as no matter how it is carved it is impossible to adapt it perfectly to your own bony anatomy. This is not a very easy material to hand carve as it is very rigid plastic. The thin tissues of the eyelid is very aesthetically unforgiving for an irrgularities..
2) Because of its rigidity, a larger lower eyelid incision is needed to place them than with other materials.
3) Should a revision be needed be aware of the traumatic nature of its removal due to the tissue adhesion.
4) Given the high risk of irregularities around the eye area I would be very cautious about trying to ask any preformed implant to do too much. This is what custom designed implants do better.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley – I have a few questions about custom jawline implants and custom infraorbital-malar implants:
1. After the implants have been secure, I understand that swelling will occur for a few days and maybe weeks after the procedure. How many weeks after the surgery do you suggest that one must wait before they engage in heavy weightlifting? I don’t want the implants to have any shifting.
2. How many days after the surgery should you wait before you can head back into the office?
3. In the event that something occurs like infection or implant shift, what would be the best course of action?
Thanks in advance,
A: In answer to your custom facial implant surgery questions:
1) One can engage in any strenuous physical activity after surgery when one feels capable. The residual swelling and implant positions can not be harmed by these activities. So it is really up to the patient’s comfort in returning to any non-contact strenuous physical activity.
2) I think your question is when will you be seen in followup after surgery. That will depend on when you plan on returning home but I see patients ever few days while they are still here locally. But if you are referring to returning to work that is going to depend on the amount of facial selling you have and when you would feel comfortable having it be seen.
3) Oral antibiotics is always the first course of action in an infection and that will usually last up to 30 days after they are started. Thereafter one goes off them and we see what happens. Should the infection return the implant will have to be removed. This potential issue is a lot more relevant in custom jawline implants than orbital implants where I have never yet seen an infection in all my years of practice.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, After giving careful thought to the imaging and other considerations, I would like to further seek your expertise. I’m seriously considering scheduling a procedure soon, but need to make sure I ask your advice on some things, first.
Accordingly, at your earliest convenience, would you, please, advise on the following:
1) With the custom wraparound jawline implant, I have concerns about the likelihood of desired change from the front view. I have been advised that when one lowers the jaw angle, the masseter muscles (that predominantly contribute to the appearance of the jaw from the front view) sometimes fail to stretch with the implant, accordingly. Moreover, it is argued, the masseter muscle often still sits where it originally inserted, and the jawline implant extends below the muscle; yet, the implant isn’t really visible, so one attains this kind of rounded look at the angle of the jaw from the front view.
Would you please advise on the likelihood of either of these outcomes, with regard to my surgery, specifically?
2) Considering that the imaging projections present a “worst case scenario,” as you say, what elements of the surgery could turn out “better” than the imaging? Does the imaging show what I would look like with the liposuction or without?
Thanks.
A:In answer to your custom jawline implant questions:
1) There is always a risk of masseteric muscle dehiscence in any surgery that involves the jaw angles whether it be standard jaw angle implants or a custom jawline implant. An important element in the surgery is to lift the masseteric muscle sling off of the bone so that it stays over the implant after it is placed. But this sling attachment is thin and tenuous and the risk of a tear and muscle retraction always exist. The risk is higher in jaw angle implants that lengthen the jaw angles as opposed to those that just widen them.There is no absolute predicting who will or will not get it. Most of the time it does not occur but the risk is always present.
2) The purpose of the imaging is to show the least amount of change which should serve as the stimulus for surgery. (not the best case scenario) No one can say whether it will or what parts may turn out better.
Dr. Barry Eppley
Indianapolis, Indiana
Dr. Eppley, I wanted to follow up on my previous question regarding skull width reduction. You said that the bone above the temporal muscles can’t be narrowed very much. I’m curious to know how much it can be thinned. I assume it varies depending on the width of the bone, but is there a percentage rule of thumb?
Also, you seemed to say that the removal of the muscle is an all or nothing procedure, meaning the muscles have to be entirely removed and can’t be partially removed for only minimal thinning. Here’s the dilemma I have: because the bone on top of my temporal muscles is just as wide if not wider than the area below with the muscles, I’m concerned that removing all the muscles (say it’s 7-9mm) but thinning the bone by say 3mm (if that can be done) will cause it to have a curved appearance. Meaning it would curve in right above my ears and then curve out on the top by the bone. Obviously that would not be an ideal outcome.
So I’m worried if my concerns are justified, and if so, if there’s anything I can do to make the thinning of bone and muscles proportionate.
Here are my thoughts:
1) to get Botox to thin the muscles, and if it produces a noticeable effect, to just thin the bone equal to the reduction Botox caused to the muscles. Essentially this way no muscles would be removed.
2) to thin the bone everywhere by an equal amount and not remove any muscles. Essentially to thin the bone behind the muscles and on top of the muscles.
The purpose is to make the thinning equal everywhere.
Thanks for the help,
A: In answer to your skull width reduction questions:
1) The temporal bone can only be thinned 1 to 2mms. But regardless of what can be reduced the only way to do so is an incision along the side of the head. It can’t be done from an incision behind the ear.
2) While you can do Botox to the temporal muscles, it is such a large surface area of muscle and the dose injected is likely to be very inadequate that this will not replicate a surgical effect for either bone or muscle reduction.
3) If you want to thin the bone you have to lift the muscle off the bone. To do so which will cause it to undergo some atrophy even if no muscle is removed.
4) While I can understand what you are trying to achieve the concept of ‘even reduction everywhere’ is not as simple or straightforward as it may seem.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have questions regarding skull width reduction.
1) Can the bone on the side of the head be thinned, or just the muscles? I’m asking because I think the top part of my head above the muscles might need to be thinned also.
2) Is skull width reduction predictable? Meaning if the muscles on the sides of the head are extracted, is it possible to remove say 4mm and keep some of it (maybe by thinning the muscles instead of completely removing them) or does the entire muscle have to be removed?
3) Is the result usually smooth, or are the noticeable bumps after the procedure?
A: In answer to your head width/temporal reduction questions:
1) The temporal muscles on the side of the head make up the majority of its width. Bone reduction has little width reduction effect. However, if the temporal line at the top of the muscle needs to be reduced that is done by bone burring.
2) Temporal muscle removal is largely an all or none approach as predictable thinning of the muscle can be not done, particularly from the hidden incision behind the ear.
3) Because what lies under the muscle is smooth bone the contour of areas where the muscle is removed will be smooth. The only potential contour issue is the transition of the cut edge of the muscle along the line of cut from the top of the ear up to the bony temporal line. Usually this muscle cut line is not seen, as it typically flattens out over time, but there is always a risk that some area of transition may be seen with movement. (jaw opening) This is really only a potential relevant issue in men who completely shave their head.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hope you are are well. It was good to visit you last summer to have a one on one session about mouth widening surgery – I believe it was well worth the traveling costs.
I have one question before proceeding to confirm the surgery – Is ingrown hairs on the mouth corners a concern?
Looking forward to your feedback.
A: While I have not yet seen that to be a problem in mouth widening in males, since males have beard skin it is always a potential possibility. Around the mouth area in men when the vermilion borders are advanced out further into the face, the vermilion-cutaneous junction is now going to involve the hair follicles. This creating an entrapped hair follicle (iatrogenic ingrown hair) is always possible.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Two years ago I had an orthognathic surgery with a sliding genioplasty. One month later a second bimaxillary surgery was done to correct the errors of the first. At this surgery the chin was brought back to its original position and the mentalis muscle. Six months later I underwent a third bimaxillary surgery at which a resuspension of the mentalis muscle was attempted but I believe that due to the huge swelling it was not reattached at the right height.
From pictures and video you can see the lip incompetence and the descent of the tissues which creates a strange projection of the chin and a descent of the upper and lower lip. What can be done to resolve the situation?
A: Thank you for your inquiry and detailing your extensive bimaxilary and chin surgery history. Between the three chin surgeries and the expansion and secondary set back of the bony chin, this strikes me as more of a tissue excess issue not a lack of adequate soft tissue suspension. Having had a failed mentalis muscle suspension x 2, this does not speak well for what any further suspension procedure would do. Mentalis muscle suspension works best when there is a true chin ptosis with visible sagging of the chin pad which can be seen to hang off of the chin. Your chin, however, looks more like an overall excess of chin tissue for the bone not a true ptosis. Between the trauma and soft tissue degloving from the three bimaxillary procedures as well as that of the chin surgeries, I think you have an overall chin pad soft tissue excess and laxity for which a suspension procedure is not going to solve.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a receded jaw and because of this my cheekbone is behind the line of my eye. (negative orbital vector) This causes my cheeks to sag and I am developing sagging and dark under eyes. I am wanting cheekbone augmentation to correct this and stop the progressive sagging. I was lined up to see a local surgeon who has developed a surgery using a coral extract called hydroxyapatite that he uses to build up the bone structure by making an incision through the under eye. Once he has done this he also says he will remove some of my sagging under eye skin and seal it up. I was wondering if you have heard of this surgeon or procedure, whether you think it’s safe and what you would recommend to combat my condition?
A: The use of hydroxyapatite blocks and granules for facial bone augmentation have been around since the 1980s. There is nothing new or novel about its use or any surgeon that still uses it. Various HA granule concoctions have been used over the years with agents such as blood or PRP to turn it into a more workable putty or a semi-injectable material. While seemingly a great idea twenty five years ago because of its bone compatibility and bone ingrowth which does occur into it, it has almost completely fall out of favor because of contour problems and secondary revisional difficulties with it. Potential contour problems such as irregularities, lumps/bumps and lack of smoothness are all the result of the difficulty with creating an absolutely smooth contour with a material that is a collection of granules. I am certain any surgeon that still uses it will say that is not a problem with their technique but having treated numerous hydroxyapatite granules patients with inadequate results and secondary irregularities this is clearly not always the case.
While hydroxyapatite offers the most biocompatible material for facial bone augmentation, this biologically appealing feature is overshadowed by its aesthetic limitations. The same can be said today for hydroxyapatite cements which can be applied in a much smoother fashion but adequate and assured contouring of it requires good visualization like an open skull site not in the limited confines of the face where discrete incisions are used often remotely placed from the site of actual augmentation.
In short there are today far superior methods of precise facial bone augmentation that can be properly planned before surgery. Having the surgeon whip up a mixture of a material and place it using an eyeball technique is really outdated and almost of historic significance in my opinion. While no facial bone augmentation is perfect the unforgiving nature of the thin tissues of the eyelid and cheeks requires good preoperative planning (3D design) and a material which allows for a good fit to the bone, a smooth other surface and the desired amount of augmentation and contours.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am enquiring about skull reshaping for my son who is very self conscious about his receding hairline which has highlighted a ridge bump on his scalp. We would like to explore possibility of reshaping.
Many thanks in advance.
A:Thank you for your inquiry and sending pictures of your son’s skull issue. He has the classic posterior sagittal crest deformity which typically ruins from the beginning of the sagittal suture at the coronal suture line junction back to the original location of the posterior fontanelle. It its typically raised 5 to 7mms and is thickest as it approaches the back part off it. In most cases the sagittal crest can be completely taken down provided that the bone is of adequate thickness. Most of the time the ridge exists because the bone is thicker along the crest not thinner but a preoperative CT scan is needed to assure that is so.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am looking for improved upper lip symmetry. I would like to show my upper teeth more when I smile. As of right now my left side is droopier than the right. As well as when I smile, I would like my teeth to be exposed more.
I wasn’t born like this. Never had trauma. Started to notice this 3-4 years ago, when I started to use Juvederm fillers (root cause of the problem?). No fillers for the past 2 years. I even did a reversal around 9 month ago to make sure there is no residue. Never had botox in the area.
Considering direct lip lift (maybe in conjunction with bull horn) but tissue needs to be lifted laterally vs in the middle. NOT looking for Botox or fillers.
Most in surgeons here are not trained to perform modified or direct lip lift and are concerned about scarring along vermilion border. They suggest bullhorn lift, but that alone will only exacerbate the problem. As a young caucasian female, I noticed scars heal well on me, almost unnoticeable.
A: Thank you for your inquiry and sending your illustrated pictures. For cases of lip asymmetry where the vermilion borders are at different vertical levels, only a vermilion advancement (wha you are calling a direct lip lift) will be effective. By directing relocating the vermilion-cutaneous border on the left side can you have sustained improved lip asymmetry. You are correction in that fillers and a bullhorn lip lift will not effective as the pull of a subnasal lip lift is central and not lateral. And while this does result in a fine line scar at the vermilion border it does heal in most cases fairly well and is an acceptable tradeoff for the improved lip symmetry.
You may be correct in that the cause may be well be the use of injectable fillers since your lip asymmetry did not exist before their use and there really is no other case for it without a traumatic injury history.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am currently considering getting a mouth widening surgery but would like to know more information about it. My main question is about the pain of it. I’m assuming you are not awake when you get the surgery, however what is the pain like afterwards?
A: While one can have a sedation or general anesthesia for an isolated mouth widening procedure, that has never been needed in my experience. This is a procedure that can be done fairly comfortably under local anesthesia in all cases I have ever done for any isolated corner of the mouth surgery. But that being said it is all about making the patient feel most comfortable and if some sedation will help in the regard then that approach would also be appropriate. Pain after the procedure is not something that I have heard patients say much about.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I want to have scrotal reduction. I’m an athlete and I am use to working out. For the last sic months I have been having trouble from the stretched out skin on my scrotum and I’m not able to workout as I used to do.
Please help me as I love working out and I’m not able to workout because of this discomfort. The main reason for choosing scrotal lift is to remove my discomfort while doing exercise and I also don’t like its appearance. I am vyoung and not married and want to know if this will it affect my sex life if I have scrotoplasty? I have heard that it effects sperm quality and testosterone hormone levels which will be not good. Please clarify my questions.
Waiting for your reply, thank you
A: Scrotal reduction is a skin removal procedure that tightens and lifts up the scrotum. Such skin removal is done along the medial raphe which is a natural midline skin crease of the scrotum. There is no negative effect on sperm production or testosterone levels as the testicles are not affected in the procedure.
Dr. Barry Eppley
Indianapolis, Indiana