Your Questions
Your Questions
Q: Dr. Eppley, Is a silicone facial implant durable for a lifetime? I have heard silicone can erode the bone if attacked from certain sources.
A: In answer to your silicone facial implant questions:
1) Solid silicone is a stable material that can only change physical form at 375 degree F. Otherwise it does not degrade or breakdown.
2) Anything written on solid silicone and bone erosion is inaccurate and biological misinterpreted. All implant materials, anywhere on the face or body, cause what is known as ‘implant imprinting’. This is the relief of the pressure caused by the introduction of an implant as it extends the natural biological boundary of the surrounding tissues. It does this, in the case of chin implants for example, by settling into the bone a bit to relieve the pressure. This causes a natural imprint of the implant on the bone. This is a self-resolving issue that is not inflammatory in nature. It actually occurs with every type of implant material in the face including Medpor, PEEK, titanium etc. I have seen it in all of them.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have attached a couple of files below– I was wondering whether or not the facial reshaping changes done on the right of each image could be achieved, and if so, through what means. I see that the bizygomatic width and the width of the jaw are both reduced. Secondly, the jawline is more defined and the chin is more robust. Could this be accomplished through implants?
A: As best as I can tell from that facial reshaping morph the following changes have occurred: zygomatic arch width reduction, jaw angle width reduction, and chin/anterior jawline extended. For these type of facial changes the following are needed:
1) Cheekbone reduction (standard anterior and posterior osteotomies)
2) Jaw angle shaving (outer cortical removal), not to be confused with v-line surgery where the jaw angles are cut off.
3) Custom chin/anterior jawline implant OR extended sliding genioplasty (modified chin wing) for the vertical lengthening effect needed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, One surgery I’m very interested in is clavicle lengthening. I’ve been told the common amount of lengthening is close to an inch per clavicle, but I’ve also read more can be done. Is it possible to lengthen each side by 1.5 inches/3.5cms? I’d love to get this surgery but I want the best possible result. I have very narrow shoulders to where my arms roll in.
A: Clavicle lengthening is very different than clavicle reduction. Collapsing the length of the clavicle is more structurally stable and has a virtually 100% rate of solid bony union because of the two blunt cut ends compressed against each other, almost regardless of the length of bone removed. Such solid bony consolidation also occurs quickly in the 6 to 8 week time period.
Conversely in clavicle lengthening a bone gap is created which, although an interpositional bone graft is placed, is more structurally unstable. It requires a long period of bone growth to occur through the graft and across the bone gap created until solid bony consolidation occurs. This is in the 12 week range of healing. Thus one must be very careful about how much lengthening (width of the bony gap) that is created. While in clavicle reduction an extra .5 or 1.0cm is not that consequential, in clavicle lengthening it is. I would not push that gap past 2.5cm or one inch per side to avoid the risk of a non-union.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have some practical questions regarding mouth corner lifting?;
-Can a corner lift be combined with a lip lift to achieve lifting of the entire span of the upper lip?
-Can you use a corner lift on a person who has a congenitally long upper lip or only on people who have saggy mouth corners due to aging?
-Which is the best technique/-s?
Direct excision (Corner lift with muscle)? DAO release (surgical/botox)? Mucosa resection? Plication of upper muscles (Zygomaticus major, Levator anguli oris) (During full face lift)?
A: In answer to your mouth corner lift questions:
1) A corner of the mouth lift can be combined with an upper lip vermilion lift, this is commonly done.
2) Corner of the mouth lifts can be done for downturned mouth corners to make them level or in horizontally oriented mouth corners for more of an uplifted look or to complete a more even vermilion line from one mouth corner to the other.
3) The technique that I use and developed is the pennant technique which combines skin removal and orbicularis wedge muscle resection and lifting. There is no role for mucosal resection or zygomaticus/levator muscle plication.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, A picture is worth a 1000 words
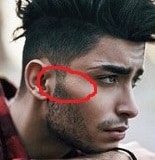 I found this picture with the red circle drawing where I think the actual cheek augmentation would be. Is this correct and does this show the length of the widening? It seems that this would make higher cheekbones laterally plus significantly increase the width in that area. Is this correct or is only part of the length Of the circle that is widened?
I found this picture with the red circle drawing where I think the actual cheek augmentation would be. Is this correct and does this show the length of the widening? It seems that this would make higher cheekbones laterally plus significantly increase the width in that area. Is this correct or is only part of the length Of the circle that is widened?
If I recall correctly you had mentioned that there can be some quite significant widening achieved, and the amount of widening is something that can be chosen by the size of the implant.
Would the temporal implants plus the chin reduction alone give a noticeable facial widening if we can get at least 7 mm, or would it likely just help some.
Also during the last botched surgery, the surgeon ended up pushing the lobes of my ears forward. Is it possible to just excise the lobes? I would want to make my ears look smaller anyway.
Finally, in this article there is something called ZSO, and I don’t know what this is but they’re saying that this procedure will produce a widening that is more round and typically suited for women’s faces, but I think I already have a lot of angles (correct me if I’m wrong) and a more around widening maybe what I’m looking for. maybe I’m wrong, and I certainly need your opinion, but it seems like my face already has a lot of angulation.
A: In answer to your facial questions:
1) You have illustrated what the lateral cheek/zygomatic arch implants are generally located. They not be quite that far back as the shown example has prominent bone anatomy in which the zygomatic process of the temporal skull bone is naturally enlarged. But you can get implants quite that far back unless one does a direct sideburn incision to do so. (which is not a bad thing as it avoids an intraoral approach)
2) Temporal implants sit above the zygomatic arch and their intent is to decrease tenurial hollowing, not create facial widening. Facial widening as to be done down at the cheek/arch level.
3) You are referring to an inferior helical rim earlobe reduction which is commonly done tor reduce the size of the earlobes and the overall vertical ear height.
4) The ZSO is the zygomatic sandwich osteotomy which means the anterior cheekbone (right to the side of the eye is cut vertically and the cheekbone is pushed out and a graft placed to hold it out. (hence the term ‘sandwich’) While it is a facial widening procedure it is way forward from the posterior facial widening effect seen in the picture. For anterior cheek widening the ZSO is the autologous option over an onlay cheek implant But fir what you are looking for…and you have found a visual example of the widening effect you are seeking….that can only be done by an inlay implant over that portion of the arch.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a sliding genioplasty 18 months ago to replace an old chin implant. My lower gums are still largely numb and I have a lingering pain on the underside of my jaw on one side, radiating up to my ear, where I can feel a gap in the bone. (Note: I developed an abscess in this spot after surgery which healed about a month later.) Can these functional problems be fixed? And are they indicative of the surgeon’s lack of skill, or are they unavoidable complications?
A: In answer to your postoperative sliding genioplasty questions:
1) At 18 months after the surgery I would think that any further improvement in the numbness symptoms would improve. Nerve recovery is usually peaked by 12 to 18 months after surgery.
2) Bone gaps at the inferior border at the end of the osteotomy cut are common. They can be filled in/smoothed out.
3) The radiation of pain up to the ear is not a postoperative sliding genioplasty symptom I have heard before and I don’t have a good explanation for it.
But for #2 and #3 what would be very helpful is to see a postoperative panorex x-ray to evaluate the osteotomy lines/bone gap/nerve foramen location.This would allow me to make a more informed commentary on these issues.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have high set eyebrows can a brow bone implant make this better? Also are you able to change the eyebrow shape with these to make them more straight? Is it possible to get eyebrow hair transplant after to get the desired shape? Can this make my little upper eyelid exposure disappear? The first picture is my current eye area, the second picture I morphed the eyebrows a bit lower and thicker. Thanks in advance and hope to speak to you soon!
A: Thank you for the inquiry and sending your pictures. A brow bone implant can not usually lower the eyebrow position or make it straight as you have morphed. Such eyebrow changes are more reliably done with hair transplantation. That will also help decrease the amount of upper eyelid exposure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a young man very unsatisfied with his facial appearance, because my face is extremely narrow. In particular, I have a very low facial-width-to-height-ratio and my eyes appear too close together. For what I have understood on Internet, an orbital box osteotomy with facial bipartition would be extremely expensive and dangerous to perform. Can custom cheek implants increase the facial width? Is there the risk that they could make the eyes appear closer together? In addition, I have a bulbous and large nose: could a rhinoplasty improve my facial appearance? Thank you very much.
A: Thank you for your inquiry and sending your picture. You are correct in that orbital ox osteotomies with facial bipartition is not remotely the correct procedure for you. That is not because it is dangerous but because it is a ‘solution that is way too extreme for the problem’. There are many aesthetic liabilities with this surgery whose tradeoffs would be worse than he original problem.
I think the single greatest maneuver to help the eye distance is a rhinoplasty. With narrowing of your wide nasal tip that alone will help make the eyes seems a bit wider.
While I don’t think that any form of cheek implants will make the eyes look closer together they would definitely addd facial width particularly in the cheek implant design had a substantial zygomatic arch component to them.
I will work on some imaging of your picture to demonstrate the effects of these procedures and get that back to you in a few days.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hey there! I was wondering if you could run me through the implant options. Could I get my whole face done? And is there a way you can make the proportions more manly and attractive? Is there anyways you can project my midface and make it look shorter/ more in proportion?
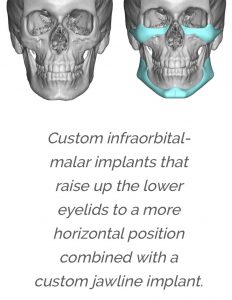
A: Thank you for your inquiry. There are implant options for every part of the face. I would refer to this website to review many of those options. (www.eppleycustomfacialimplants.com) The most common options fo me are custom jawline, infraorbital-malar/midface and brow bone implants.
How any of these changes would look on your face would require computer imaging of which pictures are needed to do so.
While the midface can be projected, there is only one limited procedure (subnasal lip lift) that can create some vertical midface shortening. But there are no procedures that can create a midface shortening effect from a structural standpoint unless one has a gummy smile in which a LeFort I impaction can be done.
Dr. Barry Eppley
Indianapolis, Indiana
 Q: Dr. Eppley, I’m thinking of getting implants to fix my under eye circles and to create hollow cheeks with an ogee curve. Would this be achievable with cheeks and infraorbital implants, also would the result looks natural if I didn’t add lateral width as my eyes are already too close together and wouldn’t want to amplify this. I’ve noticed u have gone considerately higher up with the infraorbital. Is this the way to fix the under eyes and does it touch the eyeballs? I’ve included an original and a morph of whats I’d want to achieve with u. Thanks you
Q: Dr. Eppley, I’m thinking of getting implants to fix my under eye circles and to create hollow cheeks with an ogee curve. Would this be achievable with cheeks and infraorbital implants, also would the result looks natural if I didn’t add lateral width as my eyes are already too close together and wouldn’t want to amplify this. I’ve noticed u have gone considerately higher up with the infraorbital. Is this the way to fix the under eyes and does it touch the eyeballs? I’ve included an original and a morph of whats I’d want to achieve with u. Thanks you
A: Thank you for your inquiry and sending your pictures. Your have correctly surmised that vertically augmenting the infrarorbital regions and the anterior cheek area would be the only assured and effective way to simultaneously treat under eye hollows and create more shape to the anterior cheeks for an Ogee curve effect. Like all custom implants, they are designed to what the patient’s aesthetic goals are and aren’t. (in your case avoiding lateral cheek width) How much the infraorbital rims are raised superiorly is open to debate but they never go up as high as the lower eyelid lash line. (which most likely is what you are referring to when you use the term ‘eyeball’.)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I appreciate that Dr Eppley responded to my RealSelf post and understand that a submentoplasty would be the best option. From some of the research that I’ve done, I worry that because of the location of my hyoid bone, the operation would not be that beneficial to me. I had a genioplasty a couple of years ago and the surgeon told me they removed a small amount of fat under my chin area, as best they could but that there wasn’t much to begin with – therefore, there may only be some loose skin.
I have attached a number of images as requested. Do let me know if you need anything more. The morphed image shows me pulling back the skin to show the potential amount of possible change.
A: As stated in my answer on Real Self the only way to potentially achieve that change, realistic or not, is by directing changing the cervicomental angle as previously described. This is not going to be achieved by removal of excess fat or skin, neither of which you have. Most patients with low hyoid bones have much more obtuse cervicomental angles and less lower jaw projection.
I trust that you realize what you are asking is to take the perfectly normal and make it ‘supernormal’ anatomically. This is not always easy or necessarily attainable.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in some ways to possibly enhance my cheekbones/zygomatic arch due to them been really flat. I am interested in which options I’d have, custom implants or some kind of fillers?
Also if you can recommend any other procedures for any other parts of the face I’d be open to hear, thank you!
A: Thank you for your inquiry and sending your picture. The only effective and permanent method to enhance the cheek area in young men who seek a high cheekbone look is with custom infraorbital-malar implants. Injectable fillers may offer a bit of a ‘test’ but they can not replicate the definition that an implant design will create.
In terms of their effects and as well as a good assessment of the rest of the face done by computer imaging I would need two additional pictures…a side profile and a three-quarter view.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello sir,I wanted to know whether you can change shape of my forehead?? I want a wider forehand!…Basically I want an oval face ! I have an oblong one now!!….My facial bones are wider than my forehead and it looks quite uneven… I want evenness to my face?? Is that possible? If yes let me know sir.
What are the complications ??
How much am I gonna suffer while treatment??
Any precautions ??
Is it permanent or temporary ??
A: In answer to your forehead widening questions:
1) Forehead widening can be done by a custom implant design that extends the sides down into the temporal area.
2) I would need to see a front view non-smiling picture so I can do some computer imaging to show you its effects.
3) Such a computer designed implant is placed through a small scalp incision. Recovery is largely about swelling that will develop around the eyes but it is not painful. It takes about 10 to 14 days for most of the swelling to subside.
4) The implant results are permanent.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I hope you both and everyone else in the clinic are okay. When the coast is clear from coronavirus, I plan to come in soon for a procedure. I have a few more questions because I’m still undecided about the cheek implants but am leaning in that direction.
1) How long are the lateral cheek implants are and exactly where they are they placed?
2 ) For instance, do they begin and go up from the angle of the jaw to the bottom end of the temporal implants? ) Do they go up straight creating a square widening to The bottom of the temporal implant, or are they angled out to make more of a “round V shape”, so to speak.
3) If the temporal implant is continuous with the cheek implant is it difficult to make a smooth transition? I want to be able to get a general picture of where they would widening The face.
4) I know that you have done many of these over time. How frequently have you needed to take them out and re-do the procedure , Because there is not enough or too much?
5) Do pictures when I’m younger help? ( You told me that it is not easy to judge what the actual outcome would be during surgery.)
6) Can I return the second day after and begin work?
Thank you kindly!
A: In answer to your zygomatic arch cheek implant questions:
1) and 2) By your own description you call them lateral cheek implants which are anatomically better known as zygomatic arch implants….thus they are placed on the zygomatic arches.
3) The temporal and zygomatic arch implants can not be continuous as their tissue pockets do not merge. That confluence is prevented by where the frontal branch of the facia nerve crosses.
4) Like all facial implants anywhere the never ending question os how much is enough or too little…even patients don’t really know that answer until they ‘wear them’. For this reason as well as asymmetries the global revision rate for these aesthetic concerns on facial implants hovers around the 20% range.
5) Younger preoperative pictures don’t hurt. But the canvas we have to work with now is your current face.
6) Like all facial surgery there will be considerable swelling when all three facial areas are combined. So it is not a question of whether you can physically work but whether you have the facial presentation to be comfortable doing so.
Dr. Barr Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, I just saw your post on revising a scalp scar using running w plasty. I have a scar from a hair transplant that runs across the back of my head. It’s mostly thin and straight. The left side of the scar particularly bothers me because I feel it is more indented. Anyway, I was wondering if w plasty is something that would benefit me? I’ve read that a straight line scar attracts attention, while a zig zag w plasty scar is less obvious. I’ve attached images of my scar, please let me know what you think, thank you.
A: Thank you for your inquiry and sending your pictures. While geometric scar revisions of the scalp can be beneficial, and I think you would benefit by some form of scar revision, in a very long scalp scar like yours I would be cautious. While a few selected areas may benefit by a non-linear excision pattern, I would do the bulk of the scar with linear excision. (the long part that goes across the back) You want to be certain that whatever you do you don’t make the scar worse or more obvious looking. The linear excision is aesthetically safer because, even in the worse scenario, it could only end up looking the same or just slightly better.
There is a good rule to remember about scar revisions….they are a gamble. There s no assurance that they will always end up looking better. While they usually do it is not a guaranteed outcome.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, May I ask about the ear when plagiocephaly is present. Is it possible to move the ear even a little bit? If the bone behind the ear will be reduced?
A: The answer is no asthe ear is fixed by the external auditory canal so no anteroposterior movement is possible. The protrusion of the cartilage can be setback if it exists but you can’t physically move where the ear is positioned on the side of the head.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I wanted to ask you about my smile. I show very little or not enough upper teeth when I smile or talk. You recommended a smile lip reduction. My question is, is it lifetime after surgery? How long is the downtime? Whats the exact procedure called? Thank you and God bless.
A: Thank you for your inquiry. As the name implies (smile line reduction/elevation), it is an excisional procedure which removes a strip of dry vermilion. (very similar to a lip reduction procedure) Thus it raises the lower edge of the upper lip as seen along the teeth behind it. Because it is an excisional procedure it is permanent. Other than some lip swelling it has a minimal recovery time as it relates to work or any physical activity. The sutures used are resorbable and no specific after care is needed other than some care when drinking or eating.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I been looking into your chin reduction procedure and I am a big fan of your work. Here are some pictures of my chin from the front and side view. My chin bone specifically doesn’t need a reduction. I would say I would need a submental soft tissue chin reduction procedure since I have a small chin bone and more soft tissue comes out as I smile. I am looking to get rid of a lot or at least a majority of the soft tissue. Please get back to me when possible if you are capable of working with any of the information I’ve stated. I appreciate your work very much.
A: Thank you for your inquiry and sending all of your pictures. As best as I can tell from your pictures and description of concerns you have a soft tissue chin pad excess when smiling. (dynamic chin ptosis) I would agree at rest that your chin appearance is normal. You are correct in that the only treatment would be a soft tissue chin pad reduction from a submental approach. How successful that procedure would be depends on how pliable or mobile your chin pad is at rest. A tight chin pad is not going to allow much soft tissue removal and/or will result in a wide submental scar. A mobile chin pad (the real sign of chin pad excess even at rest) will permit soft tissue to be excised with a vert acceptable scar outcome.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, good day I wanted to ask if the lower third can be lengthened in a narrow face with a small lower third total height (6.5cm) and if yes by how much. Also can the mandibular region also be supported by an implant for a better result?
And are you familiar with procedures that aim to create a better lower third without making it masculine by making it aggressively looking but just making it look less underdeveloped? (in my opinion a more developed lower third can also be more masculine even if it’s not a very broad chin compared to a overly undeveloped chin, but i think it’s important to get that across well to avoid miscommunication)
thanks and hoping you stay safe
 A: If I interpret what you are describing correctly, you are referring to primarily vertical lengthening of the lower jaw. This is not an uncommon design for a custom wraparound jawline implant. The usual amount of vertical lengthening that the tissues will permit is most limited in the chin area in which up to 10mms of vertical lengthening can be achieved. More can be achieved behind the chin but the tight tissues of the soft tissue chin pad will allow stretch so far to be able to get the incision closed over the implant. Attached is a representative example of such an implant design. To provide implant stability on the inferior border of the lower jaw some implant material must come up along the side of the jaw but this adds minimal width.
A: If I interpret what you are describing correctly, you are referring to primarily vertical lengthening of the lower jaw. This is not an uncommon design for a custom wraparound jawline implant. The usual amount of vertical lengthening that the tissues will permit is most limited in the chin area in which up to 10mms of vertical lengthening can be achieved. More can be achieved behind the chin but the tight tissues of the soft tissue chin pad will allow stretch so far to be able to get the incision closed over the implant. Attached is a representative example of such an implant design. To provide implant stability on the inferior border of the lower jaw some implant material must come up along the side of the jaw but this adds minimal width.
For patients who require more than 10mms of vertical lengthening in the chin, that is done by an opening wedge sliding genioplasty where 10 to 15mms of vertical opening can be done combined with implant augmentation for the vertical lengthening of the jawline behind it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Following jaw surgery five years ago which corrected an anterior open bite and opened my airway to resolve sleep apnea, I am left with some aesthetic issues, including a deep labiomental crease, slight lip asymmetry, and lip incompetence (see photo).
Is it possible to get an idea of the all-in cost for surgery to reduce my labiomental fold? Would this be an in-office procedure? I realize a more in-depth consultation may be necessary but any general information you can provide would be helpful at this stage. Thank you.
A: The best procedure I have found to correct a really deep inverted-V type labiomental fold is a dermal-fat graft placed through an intraoral approach where the graft is placed directly under the released skin crease but above the muscle. This will also help the lower lip incompetence. This is not an office procedure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had my appointment with my ENT today (virtual consult). He said it seems like a nasal valve collapse. I have to go in physically once the covid-19 lockdown ends. He said there’s an option to have an implant called Lateral or I would need another rhinoplasty to fix it. Is this something that you could fix? He said I’d have to pay out of pocket regardless as insurance doesn’t typically cover it so I wanted to consider my options.
A: When it comes to nasal valve collapse, the first question regardless of the treatment is whether adding internal nasal valve support will help. This can be confirmed if one as a positive response to either Breathe Right strips or the physical Cottle manuever. (pulling out on the cheeks will pulls the nostrils out wider). With nasal valve collapse there are two treatment approaches, cartilage grafting and the Latera resorbable implant. Cartilage grating is the gold standard treatment and involves the placement of cartilage grafts between the septum and the upper lateral cartilage which if done in isolation (which is all you need) can be done through a closed rhinoplasty. The Latera absorbable nasal implant strives to open the internal nasal valve and is placed inside the lateral (side) wall of the nose to lift the nasal cartilages outward. (like an internal Cottle manuever) It is very effective but is made of an absorbable material that will go away over a period of year or so when its effects will be lost as the material is absorbed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi! I just had a quick question. I have a slight maxilla prognathism. As a teen, I had braces that basically moved my upper teeth back in the maxilla, but the excess “bony-ness” remained between the base of nose and top of teeth. Basically, it creates a “monkey mouth” effect. Anyways, my teeth are actually in good position because of the braces, but I was curious if it is possible to shave the gum bone down to give a flatter look between the base of the nose and top of the teeth. Thanks!
A: That is a good question but the answer is no. Right underneath that bone (1 millimeter or two) lies the tooth roots which is what it is called the alveolar bone. Only the bone that lies above the tooth roots can be safely reduced but not the alveolar process. (maxillary alveolar reduction is not possible)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, All right, doctor, congratulations on honesty. In fact, I thought I had a double chin and I needed liposuction under my chin, but now I understand, thanks to you , what I really need.
Forgive me, if I may seem inconvenient with questions, but I am trying to figure out what to do with you , just , we are all free from this quarantine again.
I ask you, in fact, if I need paranasal implants to create that ‘male model effect’ or maybe in that area , is better for me , use something else ?
-Finally , what do you think of implants for my eyebrow crest / brow ridge and temples ?
I noticed and read on your blog, that a prominent brow crest/brow ridge is very masculine and is an attractive feature and for my temples I wouldn’t really know , what would be better to do.
For the paranasals, I’m afraid, of nerve damage or that my nose is raised exposing too much of my nostrils and especially that my smile can change , looking fake .
For the eyebrow crest/brow ridge and temples , I read, that you do, a visible incision in the area of the hairline and that here too, there may be permanent nerve damage , making sure that is little sensitive that area.
I don’t want to seem unnatural or fake, so doc I ask you, if I need these plants in these areas or there are other better and safer solutions.
A: In answer to your questions:
1) I don’t recall ever discussing any need for paranasal implants in your face. I have discussed custom jawline and infraorbital-malar implants only.
2) The third level in facial masculinization is brow bone augmentation. (not temples) When custom brow bone implants are placed they are done endoscopically through a small scalp incision. They are no issues with the potential for permanent motor nerve damage.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley: Hi, I am interested in getting a wraparound jaw implant (chin/jaw). I am interested in widening my jaw angles and having a stronger lower half of my face. The first photo attached is of my chin/jaw, and the other photos after are of what I hope to achieve. Please let me know an approximate cost range and what route you recommend taking. I was also looking into chin/jaw osteotomy surgery, but came across a couple comments made by you indicating that this type of surgery does not widen the jaw, despite what I was told by another surgeon. Thank you.
A: Thank you for your inquiry and sending your pictures. You are correct in that no form of mandibular osteotomy (sagittal split advancement, chin wing or sliding genioplasty) can wide the jaw and most certainly not in the way you want it to look.. These are mainly sagittal or anteroposterior bone movements. Jaw widening and/or creating a more defined jawline which has width requires a custom implant to really do it well in a predictable and smooth fashion. While I don’t know what your requirements are in the side view in terms of dimensional change that will await further pictures/analysis.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’ve been reading a lot on your blog how you mention that some degree sagging is likely to occur after cheek implant removal because the ligaments do not reattach.
I was hoping I could get some clarification on this.
In a 2013 RealSelf answer, I see you wrote the following in reliance to someone who has concerns after his implants were removed:
“ It will likely take at least 6 months or more for all the effects of having had cheek implants to subside. The capules will usually go away completely and the tissues will stick back down to the bone. What effects having had these cheek implants will have on your long-term facial aging is unknown.”
What confuses me is here you mention that the tissue will stick back to the bone. But elsewhere I understood you to say that the tissue does not stick back because the ligament attachments are lost. Maybe I’m misunderstanding. Perhaps I’m confusing the ligaments with the soft tissue (that is to say that the ligaments don’t reattach but the soft tissue does?)
I was also wondering if it’s impossible for the ligaments to reattach, or merely unlikely?
Thank you for the help.
A: While the tissues will eventually stick back and the capsule will be resorbed, this will be longer after the initial tis slide has occurred when the implants are removed. In other words the cheek tissues willfully heal in a LOWER position than where they were initially.
Once ligaments have been released they re not going to reattach. That applies to whether the ligament is big or small.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, does you perform any procedures for adults suffering from untreated brachycephaly that can help reduce the width of the head? I am not sure if reducing the temporal muscle will be enough…
I am this person, my head circumference is quite big (66 cm)… I cannot wear any helmet. If I could somehow reduce the big bulges on the sides of my head, I imagine the circumference would reduce which would then make it possible for me to wear some helmets. I cannot state how much of distress this has caused in my life. I feel like I am the only person in the world suffering from this condition. It has made my personal life very difficult.
A: Thank you for your inquiry and detailing our head shape concerns. In brachycephaly it rally requites a combination of posterior temporal muscle removal and bone reduction of the parietal bones. The parietal bones in posterior brachycephaly are always more flared and represent a significant part of the problem as well. It would be very helpful to see a 2D CT scan and check the slicing through this area to see how much of the bone thickness can be removed. It is not a question of whether this surgery can be done but how effective it would be.
In addition, while it may seem that you are the only one in the world with this problem I have heard your exact story numerous times.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Do you think it would be possible to transfer a large area of skin (full thickness graft) from a forehead reduction to the cheek that’s about 2 cm in height and 4.5 cm long and then reduce the scars of the borders left behind with lasers (as an alternative to individual punch grafts)? Most of my pits are concentrated in an area that size on my right cheek. If so, or if you think there’s another way to possibly fix my skin I’d like to schedule a consultation with you in person sometime in the next month or two. Please let me know if you think there’s a way to improve my skin, as I mentioned several dermatologists I’ve seen won’t do punch grafts to those areas, because they’ve told me they do not believe that they would heal properly. Thanks for your help!
A: This is definitely the type of skin grafting you don’t want to do. That wold look like a patch sitting on the cheek and would be much much worse in appearance than how your acne scars look like. Punch grafting would still be a much better option than composite excision and all thickness skin grafting.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I like your facial morphs very much.! I agree with you, in fact I wanted to ask you, whether it is better to use fillers or implants with regard to the zygomatic and orbital area? I ask this because, with my friend ,we looked on the web and we think that the implants for the cheekbones are better for women and for men maybe temporary fillers for the cheekbones are good. I repeat it was a supposition made so ‘after a little analysis but maybe you can explain the issue implants vs filler for the cheek bone area (I’m afraid the implant for the cheekbones is too big and that may have damage to the facial nerves )
Other thing I ask you ; Do you use PEEK? or some other even safer material? I read on the internet that PEEK is the one that causes the least infections.
Finally, to get me closer to a celebrity, what else would you do to my face to make me better, without looking unnatural ? I trust your opinion, I hope to meet you soon doc.
A: In answer to your male masculinization questions:
1) Given the degree of severity of your infraorbital-malar hypoplasia, fat grafting would be a far inferior choice of treatment. Besides the fact that fat grafting would never persist in a young thin person like yourself it would also not create the well defined cheek contours that you seek.
2) The reason standard cheek implants don’t look good on men is because they are made for women and not men. But forget about the use of any standard cheek implants as that is not what the morphs are showing. They are showing the use of custom designed infraorbital-malar implants…which is the implant design you need and the one that works best for most men. https://exploreplasticsurgery.com/achieving-the-hi…ek-implant-style/

The male cheek augmentation patient seeks a masculinizing effect on their appearance which is typically described as a ‘higher cheek look’. This term is liberally used but its exact definition has never been clearly explained.
3) All implants carry the same risk of infection, no implant is better in that regard. A foreign body is a foreign body regardless of its material composition. I have never yet seen an infection with infraorbital-malar cheek implants put in through a lower eyelid incision.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi, I already have a chin implant in place. But it doesn’t give me the length and definition I was hoping to get. With a custom chin implant can I get a much longer and tighter (square) chin which is protruding.
Can you also give me an estimate of the recovery period?
Thank you!!
A: Thank you for your inquiry and sending your picture. Based on your picture and stated goals, you need a 45 degree type of additional chin augmentation with a very square design. I would estimate that an additional 5mm vertical length and 5mms horizontal projection with a 35mm square width would probably suffice. How much more that is than your current implant achieves I can not say since I don’t know what you have implanted. And there is always the issue of what you see as more significant which is going to require some computer imaging to determine the actual magnitude of change you seek. To do so I would also need a front view picture to at least do two dimensional chin prediction imaging.
The recovery from a chin implant replacement should be identical to your initial chin implant placement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, About 9 years ago I had a chin reduction in which they used a titanium plate and screws to hold it together. These screws and plate were not removed. I’ve had some complications and just don’t want them in my body anymore. I had a few questions for you.
1. Is it possible to remove the hardware after 9 years? And is it possible to remove all of it?
2. If the bone has over grown on the hardware can it be removed to rechieve the hardware?
3. Would you put biodegrable screws in to fill the area or would the bone be strong enough by now even if the hardware is removed?
4. Is this a hard procedure or have you done this before?
5. What is the longest someone has had the hardware in for and were you able to extract all of it?
I am trying to receive my x-rays from my local dentist to show you but hoping you could answer these questions for me. Thank you for your help
A: Thank you for your inquiry. In answer to your questions about chin fixation removal:
1) Whether hardware has been in the chin for 9 months, 9 or19 years, its removal is possible. The ability for it to be completely removed is not dependent on time of implantation. It is actually dependent on whether the screw heads have been stripped during their placement.
2) One can safely assume that bone has overgrown much of the hardware, this is common and predictable. The overlying bone growth can be removed and the hardware exposed.
3) Your bone is well healed and strong enough that it not longer needs the indwelling fixation you have or any need further fixation once it is removed.
4) I have removed fixation hardware all of the craniofacial skeleton many many times over the past 30 years, the chin bone is no exception. When you do a lot of chin osteotomy revisions managing the indwelling hardware is just part of it.
5) I once took a fixation plate out of a 78 year old lady’s lower jaw that was initially placed to fix a fracture in 1972. She has lost enough bone height from not having teeth that the plate became eventually exposed.
Getting an old or recent panorex x-ray would be helpful to see the type of the screw heads that were used. That way one has the right type of screwdriver available that will fit the screws.
Dr. Barry Eppley
Indianapolis, Indiana