Uncategorized
Uncategorized
Q: Dr. Eppley, I am interested in pubic liposuction. I had a tummy tuck over ten years ago and my pubic area is rather puffy and i would like to get liposuction to remove the fat that completely sticks out on each side of the seam in my pants or it is disgusting in my bathing suit. I have an appointment with another plastic surgeon but I like all that you have said about this after tummy tuck problem so you seem to be experienced in what I am looking for.
A: It is very common after a tummy tuck that residual fullness of the pubic region is seen. This is because the fat content of the pubic region has not changed (tissue thickness) while what lies above it has. Since the narrowest portion of a tummy tuck is usually the scar line this makes the unaltered pubic region more evident after surgery. While many patients think that the pubic fullness is persistent swelling from the tummy tuck, this potential cause can be eliminated once one is six months after their tummy tuck. Pubic liposuction is the solution to the puffy mons and is tremendously effective at reducing its profile and making it flatter.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a facial artery pulsation on my face near my nose that has been bothering me for quite some time now. After reading your case study of facial artery ligation, I would like to get it ligated if possible. It is around the region of my cheek near my nose. I do have a hard time believing its possible to ligate such an important artery as it supplies blood to the skin and tissue of the cheek. If ligation is not possible, I would love to explore the alternatives. Maybe a fat transfer over the artery might work? I would be grateful for you opinion.
A: Please show me a picture of the area on the face where the pulsations exist. The facial tissues have such an extensive blood supply that any single artery ligation does not have a compromising effect. It is more of an issue of how easy is it to get to and would a single point of ligation be effective. Most likely you are talking about a branch of the facial artery as it courses upward around the mouth and the side of the nose. While it can be safely ligated there is the issue of back flow from the tissues that it supplies. Fat transfer for coverage is a good alternative consideration.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Thank you for your website which provides an extremely useful series of information on most areas of plastic surgery.
In relation to custom jaw angle implants, I understand there are a number of choices of material including MEDPOR and Silicone. If one is going to carve custom lateral jaw angle implants, to account for hemifacial microsomia, what sort of durometer of silicone is the best to use in this area – soft, medium or firm? Clearly, one would not want the same sort of flexibility or softness that one would expect of a breast implant for example, in the jaw area. Also, which material is better to use, silicone or MEDPOR?
A: When it comes to custom jaw angle implants, there is currently only material that is available to be used…silicone. It is my understanding that custom facial implants are no longer available as the manufacturer has chosen not to provide that service anymore. In using silicone for facial implants, the standard durometer would be firm or extra firm. Even the softest durometer for facial implants is much firmer than what is used in silicone gel breast implants. (that is for a soft tissue reconstruction not a bone reconstruction)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, These are a few pictures of my crown and a short video of my head. The hair on the ridges is sparse but in the furrows there is some. I’m not sure if I’m losing hair in this area due to mail pattern baldness or the cutis verticis gyrata. I just want to know my options for conceiving this. Wether it be a hair transplant over it or cutting it out.
A: Thank you for sending your pictures and the video. What you should do is based on how large of an area is involved in your scalp and how progressive or stable the cutis vertices gyrate is. If the area is small and stable and is not causing any other symptoms, it be left alone. I do not think it necessarily is causing hair loss but may just be spreading the follicles out further as it expands. (although I can not say for sure whether it is) The involved scalp area should only be excised if it can all be removed and should first have tissue expansion. The scalp is not very flexible and will leave a wide scar if it is all removed at once. If the scalp area is larger and it seems to be growing, then excision would not be advised. You may consider fat injections or PRP injections in an effort to treat it although such treatment is theoretically beneficial but not yet proven.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have read about your custom jawline implants (wrap-around style) on exploreplasticsurgery.com and was wondering if these implants can increase the width of the jaw angle as well as the vertical height or is it just the vertical height that these can change? I’m also trying to establish the drawbacks (apart from cost) of these wrap around implants over the separate jaw/chin implants.
A: Custom jawline implants can be made to any dimension that is aesthetically desired in either height, width or shape. The actual cost difference between a custom implant and standard implants is much less than one would think, with only about a 20% cost difference at best. While the cost of the custom implant is higher, it takes only 1/2 of the operative time to do…thus explaining why the cost difference is not that extreme. Having done hundreds of combination chin and jaw angle implants, I now find that single custom jawline implant produces a better aesthetic result with a very low risk of malposition/asymmetry compared to using three separate pieces. (1 chin and 2 jaw angles) In fact, it is virtually impossible to have a malposition of a custom implant because of the precision fit and design.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was wondering if you have and do perform surgery on cutis verticis gyrata. If so I was wondering some of the details and and maybe some idea of the length and width of a post op scar.
A: I have performed surgery on this exact scalp condition in the past and can make the following comments about it.
Cutis verticis gyrate (CVG) is a most unusual although not rare scalp condition of which its cause is unknown. But how it presents with ridges and creases is well known and that the scalp tissue thickens to create it. Treatment options are very limited with the most common approach in limited scalp areas of excision. This may be satisfactory if the rolls are limited to the back of the scalp in a horizontal orientation. But for many cases of cutis verticis gyrata the scarring is likely prohibitive. A more innovative approach is the use of subcision (release) of the creases combined with fat injections. This ‘scarless’ approach has no real downside other than its effectiveness and would be the preferred approach in larger areas of scalp involvement in which excision is not an option.
I would need to see some pictures of your scalp CVG to see which, if any treatment options, may be worthwhile for you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am currently looking to have a rhinoplasty later this year. I had a discussion with an anesthesiologist about my needle phobia who advised I speak to the anesthesiologist who will be taking care of me during the procedure. As much as I want to say I don’t have a problem with my needle phobia I do. The last time I had my blood drawn I panicked and passed out. Obviously I don’t want any of that to happen which would make my surgeon’s job harder. He suggested maybe a prescription of Valium before the procedure or something of that nature. I will let you give me your professional advise on this matter. Looking forward to hearing from you.
 A: Needle phobia issues are not uncommon in surgery. Known as trypanophobia, it is estimated that about 10% of people have it. While having to get a needle sick is unavoidable since an IV will be needed for your rhinoplasty surgery, there are numerous ways to get past this fear. Your apprehension can be remedied by taking 10mgs of Valium and 25 mgs of Phenergan orally orally one hour before arriving for your surgery. (as there will be someone driving you to and from surgery) Your surgeon can write that prescription for you. Make sure that you have signed your operative consents and had all your questions answered days before the surgery as consent can not be obtained from a mildly sedated patient.
A: Needle phobia issues are not uncommon in surgery. Known as trypanophobia, it is estimated that about 10% of people have it. While having to get a needle sick is unavoidable since an IV will be needed for your rhinoplasty surgery, there are numerous ways to get past this fear. Your apprehension can be remedied by taking 10mgs of Valium and 25 mgs of Phenergan orally orally one hour before arriving for your surgery. (as there will be someone driving you to and from surgery) Your surgeon can write that prescription for you. Make sure that you have signed your operative consents and had all your questions answered days before the surgery as consent can not be obtained from a mildly sedated patient.
The other management issue that can be done is to apply a topical numbing cream prior to actually putting in the needle. This will minimize needle insertion discomfort.
Dr. Barry Eppley
Indianapolis, Indiana
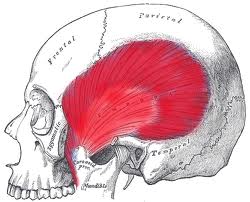
Q: Dr. Eppley, I have some questions about temporal reduction surgery.
1 What is the thickness of the temporalis muscle?
2. I have been searching for the this kind of surgery on the Internet and I have not found many surgeons who deal with this, why? Is it because it’s the most difficult operations of all or is it because there is no big demand for this procedure?
3. Do you have any materials (video, pictures) of this kind of operation?
4. When the temporalis muscle is removed , would it influence any other muscle or anything related to that section of head?
5. In your message to me you wrote : ” A vertical incision is made and the entire posterior temporalis muscle is removed and the underlying bone burred as much as possible” What is burred?
6. Is there any chance that you can make a picture for me of how I would look like after the surgery ?
7. This operation can not cause any damage to my brain?
 A: In answer to your questions:
A: In answer to your questions:
1) The thickness of the temporalis muscle differs depending on its location. The average thickness of the temporalis muscle above the ear is usually around 7mms or so.
2) Temporal muscle reduction surgery is not commonly practiced due to lack of awareness and patient demand, it is not complex surgery.
3) I do not have any videos of this type of surgery but do have intraoperative pictures of it.
4) Removal of the posterior portion of the temporalis muscle has no functional effects on the workings of the muscle and its jaw opening/closing function.
5) Some temporal bone burring is done is some cases.
6) I can do some computer imaging if I have a frontal view picture of you.
7) This is an extra cranial procedure not an intracranial one so there is no risk of any brain injury.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in Earwell ear reshaping. I have a two month old son who has prominent cup like ears. I am emailing you to ask if it is too late to possibly use the Earwell product to prevent possible cosmetic surgery in the future. His ears are still pretty soft and fold over on themselves very easily. Please let me know if this is still an option for him or would even still be successful in treating his prominent ears!
 A: Technically, Earwell ear reshaping works best when initiated within two to three weeks after birth. The ear cartilages do not yet have any memory so they will stiffen up around the molded plastic Earwell framework over the next month or so of use. While this is the ideal time to start Earwell, the reality is that many parents only start to think about therapy for their infant’s misshapen ear(s) weeks to months later. So your request at two months of age is not rare. Having initiated ear reshaping therapy in some cases at 6 to 8 weeks, there usually is some improvement in ear shape but not to the extent of that is seen when the external reshaping framework is applied within a few weeks after birth. The ear may seem floppy and without much cartilage stiffness at two months of age but the cartilage has already started to develop some stiffness (memory and thus is more resistant to cartilage molding forces.
A: Technically, Earwell ear reshaping works best when initiated within two to three weeks after birth. The ear cartilages do not yet have any memory so they will stiffen up around the molded plastic Earwell framework over the next month or so of use. While this is the ideal time to start Earwell, the reality is that many parents only start to think about therapy for their infant’s misshapen ear(s) weeks to months later. So your request at two months of age is not rare. Having initiated ear reshaping therapy in some cases at 6 to 8 weeks, there usually is some improvement in ear shape but not to the extent of that is seen when the external reshaping framework is applied within a few weeks after birth. The ear may seem floppy and without much cartilage stiffness at two months of age but the cartilage has already started to develop some stiffness (memory and thus is more resistant to cartilage molding forces.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in Liposuction of the Dorsocervical fat accumulation. I am curious if you do this procedure and what ball park of cost would this procedure be in. Please advise as I need your help.
A: Liposuction is an excellent option and often preferred treatment for neck fat. I believe when you refer to the dorsocervical fat accumulation, you seek the classic ‘Buffalo Hump’ reduction. This is a procedure that I have done numerous times (most commonly in the HIV patient although not always) and I have found that the use of laser liposuction (Smartlipo) can give a very effective reduction without the need for an open operation with a long incision. This is a procedure that takes less than an hour to do, often under sedation or general anesthesia. (it is helpful to have the patient have a good anesthetic depth so the liposuction procedure can be aggressive) Buffalo humps consist of a very fibrous type of fat (often looking more white than yellow) as opposed to a softer and more buttery type of fat more commonly seen in many areas of the body including the anterior neck. This is why laser liposuction or power-assisted liposuction (PAL) is used as it is more effective at breaking up this more dense fat that is held together by fibrous tissue bands. Buffalo humps can be very effectively reduced by this liposuction approach. In my experience, patients have not reported a recurrence of this posterior neck fat accumulation. The ballpark cost would be in the $4,000 to $4,500 range.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, If I went with buttock implants under the muscle what is the largest size I could go?Here are a few photos I would like to know your thoughts about the previous question and what would get me to my dream buttocks. I know my butt is very flat. But is there anyway to see how different sizes would look with out coming to the office since I do live out of town?What would you think the safe option is? I don’t have to have a butt like the pictures but I do want one that I can be proud of and wear certain clothes and feel good about myself. But I also want it to look natural and be a size that fits my body and my new additions up top.
 A: When buttock implants are placed intramuscular (inside the muscle, not under it), the largest size for most patients is usually in the 300 to 350cc range. (which is likely not what you are demonstrating in these pictures) From your pictures, I can certainly see why you seek buttock augmentation given that your buttocks has no projection. (flat) There is no question intramuscular implants (you’re only choice since you have no real fat to harvest) will make a significant difference just not to the degree of projection like the pictures of celebrities you are demonstrating. That can more likely be obtained with buttock implants above the muscle where implants of much larger size can be placed (up to 600ccs) but there is the potential for a higher risk of complications in that location. (although an easier recovery) When it comes to intramuscular buttock augmentation, the rule of thumb is you just put in the biggest size implant possible. (e.g., 350 – 400ccs) Why?…because it will never be too big as that is the limitation of that buttock augmentation approach. The intramuscular pocket will only allow so much volume. In some cases, and you might be one, you can also inject some fat in the subcutaneous space under the buttock skin at the same time. That adds a little extra volume (50cc to 100ccs) and gets one a little body contouring as well.
A: When buttock implants are placed intramuscular (inside the muscle, not under it), the largest size for most patients is usually in the 300 to 350cc range. (which is likely not what you are demonstrating in these pictures) From your pictures, I can certainly see why you seek buttock augmentation given that your buttocks has no projection. (flat) There is no question intramuscular implants (you’re only choice since you have no real fat to harvest) will make a significant difference just not to the degree of projection like the pictures of celebrities you are demonstrating. That can more likely be obtained with buttock implants above the muscle where implants of much larger size can be placed (up to 600ccs) but there is the potential for a higher risk of complications in that location. (although an easier recovery) When it comes to intramuscular buttock augmentation, the rule of thumb is you just put in the biggest size implant possible. (e.g., 350 – 400ccs) Why?…because it will never be too big as that is the limitation of that buttock augmentation approach. The intramuscular pocket will only allow so much volume. In some cases, and you might be one, you can also inject some fat in the subcutaneous space under the buttock skin at the same time. That adds a little extra volume (50cc to 100ccs) and gets one a little body contouring as well.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am really interested in one of the facial procedures (cheek augmentation I think) to improve my smile. I make an effort to smile only to find out that people don’t find it compelling. I am confused and this makes my self-esteem very low. I have small(weak) cheek bones which some how make me look like I am frowning all the time. It was after me noticing my self-consciousness that I started being aware of all the people I found very approachable or had friendly faces, in other words their cheek bones were gently protruding and noticeable from a profile(side view of the face). This, them having strong cheek bones, really made them appear to be ‘ever smiling’ and smile effortlessly even when it is just a grin their evoking. I looked at myself talking in the mirror lately and was evidently stunned, because I would say things but my facial expression was not corresponding with what I say or the way in which I respond to things I said to myself. For instance, when I am surprised my eyebrows don’t rise and no lines on my forehead show, because my eyebrow bone is also flat and I seem not to send my messages across to others other than verbally. A stronger cheek bone with lines on the corners of my lips and bigger eyebrow bones will make my smile sensible.
A: It sounds like you have a good grasp on how to improve your facial appearance. By your own description you know that cheek augmentation by implants, possibly combined with brow bone augmentation, would help your smile both outside and in.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I know I need rhinoplasty but am not sure what else I need. I would like you to analyze the attached photos in order to determine the ideal procedures to bring better balance to my face. These are my own assumptions about my facial appearance, both what I see as out of proportion and how to go about fixing it along with the objectives I hope to achieve
1. Droopy asymmetrical nose – It would be optimal to both straighten the entire nose and strengthen the tip (add cartilage). The tip would look best projecting forward more. I would still want to keep a high strong nasal bridge, so little shaving should be done there. Tip should still be turned down slightly a few degrees further than perpendicular to the face.
2. My eyes are too prominent relative to my other features and I would like a stronger, masculine look to eyes. I have looked at everything from malar to inferior, lateral, and superior orbital rim implants. I am less sure what would prove ideal for this issue, so your own suggestions here would be much appreciated (though if you think it is a bad area for me to augment please let me know as I want your complete objective opinion). Be as specific as possible, referencing both the individual anatomy and procedures that are possible.
A: Based on the one side view picture that you have provided, I did some imaging for the rhinoplasty based exclusively on tip rotation and elongation with minimal reduction of the middle vault height and no reduction of the nasal bridge bone. With this change I see no reason for chin augmentation which is the first other facial feature to think of when the nose becomes derotated.
From an eye standpoint, the only consideration you want to make is for infraorbital rim-malar augmentation. While superior and lateral orbital rim augmentation can be done, the effort to do does not justify the minimal benefits and risks. The focus for making the eyes less prominent should be on the recessed infraorbital-malar complex. I have factored this into the imaging.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in lower buttock lifts. Ten years ago I had liposuction on my buttocks, banana rolls, and inner and outer thighs. The gluteal band was broken and a double crease created. I have been searching for a solution. Have you have any successful buttock lifts due to botched lipo? Thanks

A: About half of all lower buttock lifts that I have done have been for liposuction deformities. Liposuction of the banana roll of the buttocks almost always makes it worse if the roll is on the lower end of the buttocks as the ligaments are released and a worsened skin roll results. This creates the double crease to which you refer which is a skin problem created by the removal of fat volume. Buttock lifts remove the excessive skin roll and create a new and more tucked in buttock-posterior thigh demarcation. At the least it always removes the double crease and converts into a more normal and desireable single lower buttock crease.
Dr. Barry Eppley
Indianapolis, Indiana