Uncategorized
Uncategorized
Q: Dr. Eppley,About the bump that is seen and the length of the clavicle, well I was thinking about doing both. (Clavicle reduction and shaving that bump) I am not sure if both are done from the exact incision spot or 2 different incisions would be made for each.
 A:The bump on the end of the distal clavicle requires a small separate incision over it for reduction. The incision for clavicle shortening osteotomies is ‘miles away’ so to speak from the distal clavicle bump.
A:The bump on the end of the distal clavicle requires a small separate incision over it for reduction. The incision for clavicle shortening osteotomies is ‘miles away’ so to speak from the distal clavicle bump.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I came across your studies recently and saw that you did a full midface mask implant using peek and it just so happened that the patient also didn’t want any or minimum lateral expansion in the malar I find myself in the same position recessed maxilla recessed infraorbitals and bad cheekbones which makes my nose appear way bigger than it is as it’s on a flat maxilla I was hoping to ask you how much or a general estimate of such a procedures cost as I Heard it can get quite expensive. Thank you
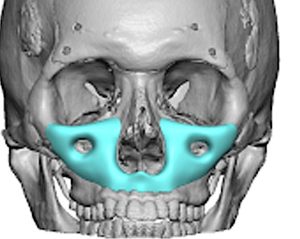 A: I have made many custom midface mask implants, mainly from solid silicone and a few from PEEK. In the US PEEK is twice the cost to manufacture as silicone and its size must be a bit more limited due to difficulty in placing it due to its very rigid construct.
A: I have made many custom midface mask implants, mainly from solid silicone and a few from PEEK. In the US PEEK is twice the cost to manufacture as silicone and its size must be a bit more limited due to difficulty in placing it due to its very rigid construct.
Dr. Barry Eppley
Plastic Surgeon
Q: Dr. Eppley, I am writing to ask for your professional opinion regarding the appropriate timing of a skull implant surgery in relation to a possible eye surgery.
I am planning to undergo a skull implant procedure in approximately two years. I have a history of strabismus, for which I had two successful corrective surgeries during childhood. Under normal circumstances, my eyes are well aligned; however, in the past, a minor head impact temporarily caused my strabismus to recur for a short time. Since then, I have also had a rhinoplasty involving significant bone manipulation, yet I experienced no issues with my eyes afterward.
My question is, in your opinion, which sequence would be more appropriate: having the eye surgery before the skull implant procedure, or after it? Additionally, I would like to ask whether there would be any risk or problem if the eye surgery were performed prior to the skull implant surgery.
A:Since I am not aware of any adverse effect on the eyes from a skull augmentation procedure I don’t think the order would matter. However in the unexpected event that there is some adverse connection then logically you would do the skull implant procedure first because it is a larger procedure that causes a lot more surrounding head swelling.
Dr. Barry Eppley
Q:Dr. Eppley, I have a pulsating bulge on my upper lip that I this is a vein. It is gradually getting bigger. How can I get rid of it?
A: Every symptom you describe as well as the picture suggests that this is an aneurysm of the upper labial artery, patrticularly its pulsatile nature. Surgical resection/ligation is the definitive treatment for such a lip aneursym.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in reducing the bump on the back of my head. My questions are:
- It is safe?
- How much of the skull protrusion can be reduced?
- What are the risks?
- How long for full healing?
A: In answer to your occipital skull reduction questions:
1) Occipital skull reduction is both safe and effective provided preoperative CT skull thickness analysis shows that the bone has adequate thickness.
2) Depends on the thickness of the bone.
3) Fine line scalp scar
4) Recovery is a week at most, full healing is 6 weeks.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Do you do drop-down supra-orbital implants that make the eye area more compact? For a low brow ridge / hunter eye look.
A: Yes but how much the brows may be able to be lowered is not exclusively the function of the implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is it possible to widen the mouth ever so slightly with a corner lip lift? Or is a commisuroplasty the one and only way? Would there be a difference in achievable width in different cases? For example would there be more width for someone with a downturned mouth than someone with a “normal” mouth?
A: All of your suppositions about the effects of corner lip lifts and widening are correct.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, in the pictures I just woke up so the veins or whatever it is it is still sort of flat it gets worse as the day goes on. This is the result of a short scar lower lift. when I went back to the plastic surgeon she said there was nothing she could do
it has been about 31/2 months since I had it done, will it get any better is there any way to shrink those veins or whatever they are???? because by night time it does get a lot worse.
A: Those are not veins but a branch of the facial artery. This is evident by three factors:
1) its serpiginous course
2) It gets worse as the day gones on
3) The temporal correlation with its occurrence after a short scar facelift. (compression)
This is treated by multi level ligations under local anesthesia
Dr. Barry Eppley
World-Renowned Plastic Surgeon.
Q: Dr. Eppley,I like to know more information in looking to getting a reduction of my brow bone because I’m not happy with the appearance of my forehead. Thank you.
A:Thank you for sending your good quality pictures which makes it clear as to your desire for a brow bone reduction. You have very strong brow bones that involve not only the frontal sinus medially but the tail of the brow bone laterally. But like many men who may seek the brow bone reduction the issue is where to place the incision to do so. I see no good place to place any form have a scalp incisional approach due to the concerns of visible scarring. There are other non-traditional brow bone reduction approaches which include a central mid forehead incision as well as eyebrow incisions. While the fine line scarring from these approaches it’s better than any scalp approach there’re still some scar concerns. Like many aesthetic surgeries a basic principle to follow is that many such surgeries are merely trading off one problem for another. You have to be certain that the trade off, in this case the scar, you would view better the\an the problem you now have (brow bone protrusion). Only the patient can make that judgment.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am 25 years old, my IPD is about 6.5mm, and my ICD is 37mm. This is the average value corresponding to the Korean average of 34mm~37mm. However, as you know, I am Asian, so I have Mongolian folds, which are characteristic of Northern Asians, and unlike Westerners, my inner canthus is covered by skin, which makes my eyes look stuffy. That is why inner canthal surgery is often performed in Korea. However, I need to excise my outer canthus to reveal more than 2mm of my inner canthus on both sides, which makes my ICD look extremely crowded, which is less than 3.3mm… But I heard that you are very famous on Google. But I am worried because 360-degree orbital box fracture is so invasive. But I am asking you because I think you are familiar with lower orbital box fracture. Are there any restrictions on the surgery? I think you don’t have to worry about scars because you are Asian and your dermis layer is so thick. I think it would be enough if my IPD and ICD increased by more than 5mm. If you are able to have surgery or are willing to do it well, I would really like to get it done right away. I am so stressed.In Korea, Lefort 1 is widely performed. However, some surgeons do not accept Lefort 2 or higher surgeries, and some have already retired. I feel like this surgery will be my last hope… Thank you for reading
A: The key question is not whether inferior orbital box osteotomes can be done but whether they could really increase your IPD by more than 5mms. That may or may not occur but what I do know is that it will definitely not increase the ICD by that amount if at all as the problem does not include the medial orbital wall. (only a 360 orbital box osteotomies does which is more invasive than you should undergo)
Dr. Barry Eppley
World-Renowned Plastic Surgery
Q: Dr. Eppley, I am interested in lower facial artery ligation. I have been experiencing pulsating stinging, soar and painfully arteries just above my both sides of my lips, center area between nostril and lip. Feels like damaged area on artery of about (1cm) this area stings non stop as like it is damaged from some sort of trauma, because of this it pulls on the artery which feels very soar and like a tight string that runs up the side of my nose, up into the inside of each eye. I had a bad infection/disease in my nasal maxillaries that I seen a ENT for and was cleared out by penicillin antibiotics and cortisol steroids 1 year ago. But the stinging and damage in my artery has never stopped in this small area above my lips. I have seen two vascular surgeons and have received dye injected CT scans, but they have said the CT scans wont show the damage or inflammation on those arteries, and they said they do not remove or do procedures on those arteries. This is where I came across your article on the exact area of my problem. Is there a procedure of a four point ligation of this area or can I get a full removal of about a 1cm of artery in this area, as this is causing me massive problems with not being able to do any physical work not being able move around, as if I do it causes pulsating pain and stinging in that area of artery. You are the only Doctor that I have seen that has talked about this area. Could you please help.Thank you
A: In my limited experience with ligation of the facial artery for aesthetic purposes (visible pulsations) it has been a single area of treatment for either double ligations or resection on one side only. In other words for a very focused problem area that clearly could be identified with a treatment that is known to work. (bulging arterial resection = remove the dilated arterial section)
Your situation is very different in many regards. While it appears to clearly involve the facial artery branch there is bilateral involvement and has symptoms which are uncommon from any arteria problem that I have seen. It is uncertain with these symptoms as to whether arterial manipulations would be effective. In addiiton it is also bilateral and what should not be done is bilateral arterial treatment at the same time since this may have vascular compromise issues (necrosis) to the upper lip.
In short the question is not whether facial artery resection can be done but whether it would be effective for the unique problem that you have.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a right pectoralis major tendon tear in September of 2024. My orthopedic surgeon repaired the tendon and I am back to training chest however I have some deformity and am hoping to get xxl pectoral implants. I also have some bilateral nipple deformity from having pierced nipples. I’m wondering how much xxl (largest possible) pectoral implants would cost and if nipple augmentation could be completed at the same time. I like large pointy nipples and I’d like mine to look more uniform. Currently as you can see in the pictures they have scars from the piercing that’s almost looks like a 3rd nipple. I’m hoping the doctor can do pectoral implants and nipple correction while increasing the length and size and symmetry of the nipples as well. Thank you
A: The concept of XXL pectoral implants is open to interpretation as to what thet actual implant size is. But what is most relevant is whether the XXL implant is the largest standard (Powerflex II, 690ccs) or whether a custom implant must be made. I would need to see some pictures of your chest, know uyor height and weight and see examples of what you see as an XXL chest size.
When numerous forms of nipple plasty can be performed at the time of pectoral implant placements the combination of a pierced nipple repair and nipple elongation can be problematic. (as nipple elongation usually requires placing a graft.)I would have to see pictures of your nipples to have a better idea as to what is possible.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I feel like my face is very asymmetrical and imbalanced and lacks dimension. I feel like I need some sort of implants – cheek or paranasal. And a forehead augmentation – but I don’t know if fat grafting or an implant is more suitable. My right temple goes inward and my right jaw is narrower than the right, so I feel like I need an implant on my right jaw. But at the same time I feel like I need to shave my left jaw and my chin for more contour.
A:While you do have differences between the two sides of your face (see attached grid analysis) when it comes to surgical correction you have to have a very clear idea as to what exact procedures are needed so that the surgical efforts can help minimize the asymmetry. You have described deficiencies which are largely based on your right face which seems correct given that your pictures show a classic right facial vertical asymmetry. (shorter from top to bottom)….provided these pictures have not been reversed. But the first step in facial asymmetry is to get a 3D CT face scan so the bony differences, as most of the facial asymmetry is bony based, can be clearly identified and the properly treatment planned. In most facial asymmetry deficiencies this means custom implant designs.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Last year I had a malar and premaxillary implant put in as I had a very sunken face from previous pr molar extractions. My surgeon promised me that this would not have any effect on my nose and that if I didn’t like it I could remove them and everything would eventually go back to pre operative state.The implants completely further destroyed my face and really made my nose look wider and thicker so I took them out 4 months after. Now 13 months after I am devastated over how my nose is completely destroyed. I had the most perfect nose and I was very particular about not wanting any changes to my nose and if that would be the case i wouldnt want to proceed with the surgery. The surgeon further reassured me that it would not have a negative effect and would just serve as a filler in the area. The surgeon is gaslighting me telling me that he has not touched my nose during the procedure and that he doesn’t know what happened to it. He has been very strange with different answers and even stopped to answer me completely at one point. I don’t know where to turn for answers since he refuses to give me answers. Since he removed the implants e hasn’t even cared to invite me back to the office or take a look at my nose once and he just keeps saying that he doesn’t know what happend. I have only managed to find answers on your website so far and I am devastated to see that for this procedure you have to in fact detach the nose on several places to fit the implant and my surgeon just won’t admit to it. Please help me, what can I do to get my nose back?
A:In any form of intraoral midface surgery, whether it be a LeFort osteotomy or a midface implant where a complete soft tissue degloving from the bone is needed, there can be some potential changes to the nose particularly that of the nasal base. (premaxillary-paranasal area ) The nostrils can become wider as the soft tissues have become detached and retracted. This potential anatomic issue has been known for decades and is why a variety of protective procedures during closure from these procedures have been employed to try and prevent these adverse nasal base changes. (e.g., alar cinch suture, V-Y musculomucosal closure) Even in ‘simple’ paranasal implants the nostrils have been shown to increase in width by 1 to 2mms.
Postoperative management of the wide nasal base can be treated by external nostril narrowing techniques or even inraoral cinch sutures. Ironically they are more effective when combined with some pyriform aperture augmentation…even though that was the original source of the problem. (the soft tissue degloving was not the implant per se)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am seeking vertical jaw angle implants to get a result like the attached pictures.
A:Thank you for sending your pictures. Before deciding on what type of implant to use the first step is to determine what type of jaw shape change the patient is seeking and what amount of such change is acceptable. This is the role of pictures and computer imaging. In looking at your pictures I have significant concerns that with your fuller tissues any type of standard jaw angle implant is just going to get lost (not seen) and may just make the face fuller/heavier/fatter. If the goal is a more defined and visible jawline that does not appear likely to occur with the thickness/looseness of face and neck tissues you have.
Excess soft tissues can be overcome by jaw implants but it takes a lot of implant size to push the tissues out and then the issue potentially becomes ending up with too big of a result. With fuller faces concomitant soft tissue reductions are usually done at the same time to help the jaw augmentation result be better.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hey just wondering at what age would you perform skull reshaping surgery? Would it be 18 or fully grown or what age would you consider performing this surgery? Thank you
A: Adults age 18 and older is the minimum age for skull reshaping surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to lift my nostrils on both sides so that the base of the left and right sides that joins with my upper lip area is brought up to align horizontally with my central nasal area.so instead of my nose being ‘upturned’, it becomes horizontally straight. I have screenshot the photos from your gallery and can share them.
A:You cannot effectively raise the base of the nostrils by 5 mms, It is one thing to lower them by skin removal but raising them is a different and more challenging matter.
Dr. Barry Eppley
World-Renowned Plastic SurgeonCan My
Q: Dr. Epple, Hi doctor , thank you for your work!! What happened to me was that in my younger years I experienced a traumatic event . Now as an adult I’m still living with past trauma from my past . I’m highly self conscious of my head , in the back right side , as a result of that incident . I will send the pics and was wondering if I can correct that because it’s really hurting my life. Also , I’m self conscious of my nose and was terrified and concerned that if I get work done on the back of my head , that my nose is going to get more deviated because of the nature of the procedure in the back of my head . Since I will be laying face down . Is that true ? And also am concerned of the final results and any visible scars . Please comment
A:When back of the head skull augmentations are done the patient is in the prone position. But to protect the nose from pressure the head is placed in a special padded donut head rest that keeps the nose from touching the operative table. This is classic periooperative pressure sore prevention.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in the largest custom butt implant that I can obtain with or without fat transfer. Is 1,000 ccs the largest available? Do you place tissue expanders in the buttocks as an option? Thank you.
A:Unless you have indwelling buttock implants you have correctly surmised that first stage tissue expanders would be first needed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am very interested in decreasing the overall width of my head. I have been reading about both the anterior and posterior temporal muscle reduction procedure and I think both would be a suitable procedure to decrease overall head width. Although I am concerned about thickness of my bone on my forehead which still adds a substantial about of thickness to my head size. Would it be possible to know if I would be a good candidate to have both anterior muscle reduction and forehead recontouring (forehead burrowing) by assessing pictures of my forehead?
A:Your question about head width reduction is a good one since the sides of the forehead and the temporal areas share a similar developmental origin, so often both are involved. The only way to answer that question is with computer imaging to show temporal width reduction without any change to the bony forehead so you can be the judge as to whether forehead reduction is needed as well. (see attached)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have what I consider a receded chin, and I don’t care about anyone else’s opinion on it to be blunt. I want a more forward appearing lower jaw, and would like to get reconstructive jaw surgery, but if sliding genioplasty can create the profile I’m looking, then I would be willing to a less invasive surgery. My main concern with just genioplasty is the labiomental groove. Mine already bothers me a lot, and I need it to be much, much flatter. I’m also interested in Rhinoplasty but my main concern is my chin. I’ve attached a few pictures or my profile, as well as two edited photos to give you an idea of what I’m looking for.
A: When you a short chin, deep labiomental fold and lower lip eversion this is all a reflection of an overall short lower. What really improves the depth of the labiomental fold and the lower lip eversion is having the whole lower jaw come forward. As the lower teeth move forward this pushes the labiomental fold and the lower lip forward. Thus you ideally need a BSSO mandibular advancement…but it will not create by itself the chi projection you are showing. It would need to be combined with a sliding genioplasty also moving the lower jaw forward will not create that degree of chin projection.
The alternative to total lower jaw advancement is a sliding genioplasty combined with grafting of the bony stepoff with fat injections to the labiomental fold. This will not produce as good as a result of the labiomental fold correction as the combined lower jaw advancement and sliding genioplasty.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, The top back of my skull is depressed due to surgery as an infant. The depression is deep, wide and long so if plastic surgery was performed it would need to stretch skin or need a skin graft. I’m not sure of your capabilities but has your practice dealt with the issue described. Thanks.
A:What you are suggesting is the possibility of needing a first stage scalp expander procedure. (not a skin graft) That is a procedure I do regularly when more stretch of the scalp is needed for the amount of skull augmentation required.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in gynecomastia reduction surgery with nipple reduction at the same time. But did have one concern that another physician raised regarding a nipple reduction – specifically, the physician was very hesitant that such a procedure was worthwhile considering the risks (which he described as a 20% chance of necrosis of the nipple following such a procedure) – I would be curious to hear your assessment of this risk (or others) as pertains to a nipple reduction procedure before I make a decision.
A: I am not sure at all what is the origin of the statement by a surgeon of ‘there is a 20% risk of nipple necrosis when nipple reductions are performed with gynecomastia reduction’ for the following reasons:
1) Nipple reduction in a male almost always means nipple amputation, the complete removal of the projecting nipple, thus there is no nipple left to have any necrosis. I can only assume what this doctor is more likely referring to is ‘areolar necrosis’ or difficulty with the nipple reduction site healing. This has not been an issue that I have ever seen.
2) This ‘statistic’ is based on what I do not know since there has never been anything published in the plastic surgery literature in that regard or any other literature since the performance of male nipple reduction in gynecomastia reduction is so rarely done.
3) The relevancy of potential vascular compromise to the nipple-areolar complex is based on what type of gynecomastia reduction is being performed. If an open gynecomastia reduction is performed through an inferior areolar incision, where the nipple-areolar complex is left with a thin layer of tissue underneath it and it depends on vascular inflow from the surrounding dermis (where half has been cut off from the inferior areolar incision). then one would have reason to consider there may be the potential for vascular compromise from the healing nipple reduction site. But this issue becomes moot when the gynecomastia reduction is performed by liposuction without a direct areolar incision.
4) But when in doubt one can always delay the nipple reduction for a week or two after surgery since it can easily be done as an office procedure under local anesthesia. (where the chest is largely numb anyway for awhile)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am wondering whether to get a chin implant or a sliding genioplasty for chin. I want my chin to be wider and square from the front view I want vertical and horizontal projection.
In terms of front view of face, can the sliding genioplasty provide as much chin widening as an implant can for that masculine look? And for the side profile, I am aware that the genioplasty provides more projection.
A: Thank for your inquiry and sending your picture. You have numerous misconceptions/misinformation about what are the dimensional effects of chin implant vs a sliding genioplasty. So let me provide you with some clarifications:
1) A sliding genioplasty can effectively create more horizontal and/or vertical increases in projection. It, however, does so at the expense of width. Depending upon the degree of horizontal advancement the chin will always get more narrow. It has NO ability to make the chin wider.
2) A standard chin implant can effectively create more horizontal projection and width but can only create very minimal vertical lengthening.
3) The amount of horizontal projection between a standard chin implant and a solidify genioplasty is equal out to 10mms. Beyond that only a sliding genioplasty can add greater horizontal projection.
4) A custom chin implant can create horizontal, vertical and transverse (width) increases. It is the only option that can create a 3D chin augmentation effect.
By your own description you are seeking every dimensional increase possible which can only ideally be met by #4, the custom chin implant.
There is also an amalgamated approach to achieving a 3D effect with the two basic chin augmentation methods, a sliding genioplasty for the horizontal and vertical increases combined with a chin implant overlay to create the width.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Thanks for doing the imaging on my potential shoulder width reduction procedure. From the picture it looks like so much change. But I have the following questions.
If the clavicle is cut, will there be any backbone issues as I have to always have the shoulders moving forward? Will it not create a structural stress on my back in the future? How will my shoulder blades adjust to this pulling forward? Will it impact my range of motion?
A: As I discussed with your husband at length on the virtual consultation and to answer these questions to you directly:
1) Clavicle shortening of 2.5cms per side does not cause any spine or shoulder joint dysfunction. To potentially create such dysfunction it has been shown that it takes greater than 30% reduction in clavicle length to do so. With an average female clavicle length of around 14cms and a reduction of 2.5cms, this is only an 18% change in clavicle bone length….enough to make a visible difference in shoulder width but not enough to cause shoulder joint dysfunction.
2) The clavicle shortening is 90% horizontal reduction and 10% forward movement. Thus their is a very minimal anterior rotation which does not cause a substantial pulling of the shoulders forward.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, I have been looking to have chin surgery for a while now. My chin is my biggest insecurity. I never smile due to the way my chin pulls down when I smile. I also dislike the dimple in my chin and how wide my chin looks when I smile.
A: Thank you for your inquiry, sending your pictures and detailing your concerns. You have two specific soft tissue chin concerns, 1) hyperdynamic chin ptosis and 2) a vertical chin cleft. They may be anatomically related as a vertical chin cleft occurs due to a midline soft tissue deficiency. For improvement/correction a submental approaches needed as the size of the chin pad must b reduced and the chin cleft managed by a muscle repair in your case. Such soft tissue chin repairs, while not technically challenging to perform, are difficult to predict the outcomes since surgery is done in a static setting while your chin issues mainly appear with dynamic motion. (smiling)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a Occipital Crown Deficiency in my skull that’s why I feel really bad about this. Is there any chances to reshape it without risks. So i will look normal as others.
A: I would need to see some pictures of your occipital crown deficiency to determine whether a custom skull implant would be the correct solution. By description alone certainly sounds like it would. While no surgery is not without risks, skull reshaping surgery in general and custom skull implants in particular have the lowest risk of almost any plastic surgery that I know.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I hope this finds you well! I learned that my 3D CT scan copy is received and we will be able to move on to implant design process very soon, which is exciting.
At the same time, I was meaning to find out the following, if you may share your input, that would be great.
1. The following link from your blog shows that this case achieved a 15mm-20mm of augmentation, without a 1st stage augmentation involved. Is this amount of augmentation achievable in my surgery?
 | Case Study: Flat Back of the Head Correction by Augmentation Cranioplasty – Explore Plastic Surgery – Explore Plastic Surgery – Dr. Barry Eppley – Plastic Surgeon Background: The shape of the skull is affected by numerous factors including genetics, in utero skull pressures, post delivery head positioning and growth of the brain. In general, the skull has an oblong shape that is slightly wider in the back than the front. While there is no uniform aesthetic standard for a pleasing skull Read More… exploreplasticsurgery.com |
2. During the design process, how can we figure out what is the maximal augmentation level that is right below unduly tense (too tight) level while it is at a largest viable stretched amount?
3. For augmentation of the areas on which the head is in contact with a pillow while sleeping, e.g. the back of the head, the sides of the head, what are the chances for the implant be moved or loosened, caused by the weight from my head and neck pressuring on the implant approximately 8 hours a night over many years?
If this is a real concern, can we address to this risk during the design stage?
If implant loosening does occur at some point in the future, due to the weight from the head and neck during sleep, how will we handle it?
4. I highly regard your input in the design process of the implant. I replied Dawn’s email on what surgery outcome I would pursue. Please don’t hesitate to share your advice.
5. After surgery, I may choose to have a shaved head style some point in the future. When there is no any hair bearing for camouflage, will the skull shape still look natural and smooth, especially at the edge area where the implant ends and connects to my original skull area?
What makes a smooth and natural transition at the edge of implant possible?
6. Will the implant cause infection many years after the surgery is done?
7. Is an augmentation implant supposed to last all a life-time long?
If not, in what circumstances does the implant require what form of maintenance in the future?
8. After surgery, will it be ok to receive head massage? E.g. finger pressuring on scalp, which is provided by a regular message therapy store.
9. Will I need an additional revisional surgery? If one is needed, how long after the surgery will this happen?
Thanks for your attention Dr. Eppley : )
A: In answer to his custom skull implant questions:
1) No. That was done with a full open coronal incision which allows for some added expansion due to the mobilization of tissues.
2) There is no exact science as to how to know when the implant is too big or the tissues would be too tight to allow it to be placed and the incision safely closed. My design estimates are based on my experience of placing such implants.
3) Zero. While an understandable question it is never been a postoperative concern., I have never seen a custom skull implant move after surgery.
4) I still need to know what skull areas we are going to cover…back only, front only or both?
5) Due to the feather edging in the design there is a smooth transition from implant to bone.
6) No. Infection risks are in the perioperative period. (up two three months after surgery) Once last this time period the infection risk is negligible.
7) Custom skull implants are made of a solid silicone material which will never degrade or breakdown…thus no need for future replacement due to material failure.
8) Head massages are not needed or advised after surgery.
9) Revisional skull implant surgery would only be needed if you determine you want a bigger implant or a different design later. This is not done until six months after the initial surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, do I need to wait until the Radiesse filler in my chin is fully dissolved before getting a sliding genioplasty in order to minimize risks?
A: You do not have to wait until the Radiesse completely dissolves which could take a year or longer. In addition there is no reversal agent for the type of filler Radiesse is. There are no adverse consequences of having an injectable filler in the chin to performing a sliding genioplasty. Most, if not all, of the injectable filler is mainly in the soft tissue with a minimal amount on the bone. Whatever is on the bone will simply be removed as part of the surgery. I have seen lots of different fillers on the chin in performing this surgery and it has never been a problem during or after surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My daughter is 2.5 years old and I have been worried about her head shape since she was 10 weeks old. I brought it up at every wellness check but was dismissed by her pediatrician saying it was fine. Now it’s too late and I live with guilt and regret daily. I was reading on your site about the skull augmentation implants on toddlers. How invasive of a procedure is this and what are the risks? How many cases have you done on toddlers and what is the success rate? I have attached some photos of her head.
A: Skull augmentation is not an appropriate procedure for infants. The skull needs to grow a lot more and the earliest I could consider it is 4 or 5 years of age….but likely even later than that age.
Dr. Barry Eppley
Indianapolis, Indiana