Your Questions
Your Questions
Q: Dr. Eppley, I have severe plagiocephaly and It is difficult for me to live with it, so I would be very interested in your services.
But I have a few questions, because this is not a operation that has to be taken lightly.
So if I understood correctly, to correct the plagiocephaly, you use an implant that you put over the skull. Meaning that you don’t cut, move the bones of the skull, right ?
So does that mean the technique of the implant over the skull has less risks to fail than the operation where they move the bones of the skull to position them in a bettter way ?
If it fails what are the consequences? (Brain problems?)
Other questions, what is the durability of the implant ? Does it last forever ?
Is it solid ? Will it not move ?
And how is the implant fixed to the skull ?
A:In response to your adult plagiocephaly surgery questions:
1) You have correctly surmised that in adult plagiocephaly it is treated by an extracranial implant augmentation.
2) Extracranial operations have none of the risks associated with intracranial procedures. They are typical implant-associated risks like any other aesthetic solid face or body implant.
3) Skull implants are solid, do not undergo material degradation, will not move and will last the patient’s entire lifespan without needing adjustments for any of these issues.
4) Skull implants are permanently secured into position by small screws, perfusion holes and an encapsulation process.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m interested in having my Perioral Mounds removed. Am I a candidate for that procedure?
A:Thank you for your inquiry and sending your pictures. While your ‘perioral mounds’ can be treated by liposuction that is not the best treatment for them. They are actually tissue that has drifted forward as part of the aging process, creating mounds of skin in the perioral area. Thus they do not represent isolated fat collections with good quality overlying skin which is the requirement for a good liposuction reduction result. Rather the far superior procedure is a lower facial tuckup procedure (lower facelift) which moves these sagging tissues back along the jawline/lower face for a smoother and rejuvenated appearance.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I wanted to please ask if you could assist me with forehead reshaping surgery. I find the profile of my forehead very straight, and I’m looking for it to be more convex and backward sloping. Is this an achievable goal?
A: Thank you for your inquiry and sending your pictures. Your forehead profile is very straight for two reasons, 1) the upper forehead is very developed and 2) the brow bones are not. Thus in changing your forehead slope to a more retroclined angle the options include upper forehead reduction and brow bone augmentation. Upper forehead reduction alone is helpful in that regard but because of the limitation of the thickness of the frontal bone it will only change the slope so much. (see attached imaging) Adding projection at the lower end of the forehead (brow bone augmentation) helps tilt the angle back more. (see attached imaging) In the examples you have provided both of those men have more pronounced brow bones.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to give to my scalp a more asymmetric and rounded shape. From my analysis i just needed to fill some spots to achieve the goal.
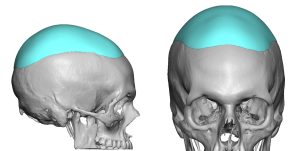 A: Thank you for your inquiry and sending your pictures. As a general rule you don’t try to ‘spot’ augment a skull shape unless it has only one small area that is the problem. A far more predictable skull shape is assured when the entire surface is covered with a single implant even if it is very thin. Attached is an example of the general concept as well as the type of change you may be seeking.
A: Thank you for your inquiry and sending your pictures. As a general rule you don’t try to ‘spot’ augment a skull shape unless it has only one small area that is the problem. A far more predictable skull shape is assured when the entire surface is covered with a single implant even if it is very thin. Attached is an example of the general concept as well as the type of change you may be seeking.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I got a sliding genioplasty on July 6, 2022. Since I saw my face I thought that it looks long and I look older, also my lower lip is smaller now, it feels very tight when I talk and when I smile my face looks way longer which I hate because I used to have a very pretty and proportional smile. I talked to my surgeon and he said that the proportions are fine so I talked to another surgeon who also said that it looks great and that he would not change it because it would make more harm than good since I had the surgery not so long ago. The Dr moved 7mm and I feel like it was way too much, as a matter of fact I have cried nearly every day since I saw my face and I regret ever doing this procedure.
I wanted to talk to you before scheduling an online appointment to know what you think. I spent extra money getting a CT scan and X rays for the other surgeon that saw me and in the end he told me he wouldn’t suggest me doing a reversal procedure. I read online that you have experience with this issue and I wanted to know what you think, if it’s possible to reverse it at least 4-5mm, how long I should wait and if you think it may have a good outcome. Thank you for reading.
A:Thank you for your inquiry and sending your pictures and x-rays. I have seen many females in your chin augmentation situation. Yes it is true that you are just two weeks out from surgery and still have a lot of swelling. But I have not yet seen a female who feels the way you do every change their perception of their result months later when all of the swelling has dissipated.
So let’s review what is relevant in your case.
1) You had a well performed and executed sliding genioplasty as per the x-ray. Thus the operation was a technical success.
2) Despite being a technical success, it was an aesthetically flawed operation as the final position of the bone was further forward than what you could aesthetically tolerate. I don’t know how the number of 7mms was chosen or the basis for it. But i would wager you were not given options before surgery using computer imaging to try and determine what looks best to you. On paper and by traditional aesthetic norms bringing your chin out to a line dropped down from the lips is supposed to be the ideal position (see attached)…but for many females with short chins that is simply too much change. Surgeons may look at it and think it is great but the patient may never really adapt to it. Usually a projection less than ‘ideal’ is really ideal for most female patients. (see attached)
3) Since there was a reason you had the original surgery reversing it completely seems counterproductive. A subtotal reversal seems more logical (e.g., 7mms back to 3 or 4) but that is a personal choice of yours.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I dont have pictures of my case right now, but my case is quite similar to this one “Plastic Surgery Case Study – Custom Deltoid Implants for Shoulder Contour Restoration After Muscle Atrophy From An Axillary Nerve Injury”. I am so excited to find a documented procedure for this deltoid athrophy. Currently, I am living in Europe and I would like to know if there is some chance to do the surgery in Europe. While I am now in my mid 40s and I have this issue since I am 20 (date of my shoulder surgery), so just thinking about finding a solution makes me quite happy. Thanks for the time and I hope you can help me find a solution for this issue that I have been carrying for more than 2 decades.
A: The good news is that the muscle atrophy from your axillary nerve injury can be aesthetically improved by a custom deltoid implant design. Unfortunately I only do surgery in the U.S.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had double jaw surgery to correct a severe underbite three years ago. An 8mm sliding genioplasty was also performed at that time. While I look and feel much better now, my jawline still lacks definition from the sides, and my chin falls slightly short of what I believe is the optimal position (the pink of my lip). I would love to discuss custom jaw implants and the options which may exist for me.
A: Thank you for your inquiry and sending your pictures. Orthognathic surgery provides a good skeletal foundation but it’s effects are largely in the sagittal dimension and thus can never create improved jaw definition, it only creates better chin projection. But now you are seeking the proverbial ‘icing on the cake’ so speak for the lower jaw of which a custom jawline implant is the better procedure to do so. (see attached imaging as one potential type of change) Your fixed deep labiomental sulcus is an issue to be aware of and may need to be addressed as any further chin projection is going to magnify its depth.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to have my lips lengthened via lateral commissuroplasty to have each corner of my lip come directly under my pupils as I feel my lips are too narrow and not ideal.
A:Thank you for your inquiry and sending your picture. I would certainly agree that your mouth width is small compared to the rest of your facial features. In my experience with mouth widening surgery the primary risk is adverse scarring. In such surgery the scars usually do well out to width increases of 5 to 7mms. Beyond that scarring becomes more of a problem. Based on your picture I would estimate you would need 10mms per side to reach a good mouth width on each side. That puts you at great risk of poor scarring which would be my concern for you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I recently found you while searching for temporal reduction, And hoped you can answer my query. I have brachycephaly which I had surgery for to fix the flat spots on the back of my head, however the side of my head is round, I was wondering if temporal reduction by Botox can change the shape of it and make it flatter and reduce the size simultaneously. I understand with brachycephaly The skull bone plays a part, but I was wondering if Botox can give me a less convex shape when viewed from straight on. The width of my head does not bother me as much as I’m a pretty tall and big guy but the round shape does. If Botox can achieve a significant result, I would like to set up a treatment plan with you.
A: The wide back of the head or the temporal-parietal region is the location of the posterior temporal line were the temporalis muscle is the very thinnest. I would doubt that Botox or even surgical removal would make much, if any, difference in this part of the head. There is however one way to know for sure…do it and see what happens. Since it is a non-surgical procedure you can easily find out.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in jaw augmentation for my short lower face. What can be done?
A:Thank you for your inquiry and sending your pictures. You have a fairly severe chin deficiency due an underdeveloped lower jaw. Ideally you should have lower jaw surgery first before any efforts are done from an aesthetic standpoint to create a better chin/jaw foundation. But I will assume for now you are aware of the ideal initial approach of jaw surgery and are bypassing that and are just going to do the best with the shape of the jaw the way it is now.
In that regard the best approach is a maximum sliding genioplasty for the chin. Whether you should try and add on jaw implants with the sliding genioplasty is a subject up for further discussion. Normally I would do some computer imaging to demonstrate some of these potential lower facial changes but your facial hair creates enough distortions that it partially obscures those potential changes.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Interested in forehead contouring, specifically glabellar furrow excision with placement of ePTFE bone implant. Please can you advise on the scar left following this surgery and does it fade?
A: The scar from glabellar furrow excisions usually do quite well since the furrow is already very much like a scar and a vertical scar line is in the natural relaxed skin tension of that area of the forehead. So yes th scar fades/blends in pretty well in the cases I have done.
Please send me a picture of your glabellar area so I can see how these comments may apply to you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have two very distinct bumps/horns on my forehead. Only directly noticeable with “above-lighting”. Is there a proven surgery method for evening my forehead?
A:Thank you for your inquiry. Forehead horns are a common forehead concern, particularly in males, that I see for reduction. To fully understand how they are reduced I would refer you to one of my websites, www.exploreplasticsurgery.com and search under Forehead Horn Reduction on the home page. There will a number of cases studies that show the surgical techniques to reduce them.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, The marked part of my chin is too long in the downward direction. Is there a chin implant that can show this part higher? or can this jawbone be filed from below.Is there an implant to cut the bone or show it higher?
A:Thank you for your inquiry and sending your picture. What you are referring to by your marked picture is a low prominent jaw angle…even though you refer to chin in your description. I assume this is a translation issue/error. The low jaw angle can be treated by two different jaw angle reduction approaches. The first is to reduce it by cutting the bone if the goal is to make it less visible. Whether this is better to be done from an intraoral or external approach can be debated. The other approach is to burr it down slightly and place a widening jaw angle implant above it which is done completely intraoral. Which approach is best depends on the exact aesthetic jaw angle result one finds looks best to them.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I wanted to inquire about the removal of my medium medpor chin implant that was placed submentally four years ago with one or two screws used for extra adherence. This request would be for removal only, and not replacement with another implant. It’s my understanding that due to the nature of the implant’s material, removal comes with a higher risk of disfigurement and other complications. I was interested in gaining more information regarding your experience with removing these types of implants, how often you’ve seen long-term issues as a result of removal. I know certain deformities can be mitigated with filler however, I am not interested in filler.
Another issue I’ve had, which is important for me to address, is that the incision site has intermittently presented with soreness/swelling internally just below the scar. I spoke with the surgeon who initially placed the implant and he seems to think that is a result of scar tissue– i’m unsure if that’s accurate. I would be curious if any old scar tissue could be removed during the implant’s removal procedure.
A: In answer to your Medpor chin implant removal questions:
Q: Dr. Eppley, I recently had bimaxillary surgery for sleep apnea and TMJ issues, but I was worried if I was advanced too much? I worry about a “chimp” like look, but strangers online and people I know in person say this isn’t the case.
| Either way, I was worried that my cheekbones were left behind in the process and now lack forward projection, though I believe my cheekbones have good width. What would be my options in terms of increasing the forward projection of my cheekbones? Also I’m only a couple weeks out from surgery with swelling and splints, hence the swollen lips that can’t close yet, so that can be kept in mind. |
A: As you have stated you are early in the recovery process so there remains a lot of swelling yet to resolve. It is probably very unlikely that you will look over advanced when all the swelling subsides.
By definition a bimaxillary advancement always leaves the infraorbital rim and anterior cheekbones behind and is the one significant aesthetic tradeoff of the procedure. There are a variety of implant augmentation methods to augment this newly created area of facial recession secondarily.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, When previously researching the sliding genioplasty procedure locally, I have been told to achieve the best results a neck lift would be best compared to submental liposuction that Dr. yourecommended. Can you explain the difference?
A: I would never do a necklift in a young male with no real skin laxity. Quite frankly that would never be an option given the scars that would result and that is simply isn’t necessary. The debate can be made between submental liposuction vs submentoplasty in treating your neck but not a formal necklift. But whomever made that recommendation has no understanding of how much improvement the sliding genioplasty alone will have on your neck.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My philtrum length is roughly 1.7 – 1.8cm long, and so I think I would be an ideal candidate for a lip lift. My concern is that having the procedure would deform my nostrils. I have attached both side profile and front on images of my face. My nostrils are already quite prominent. I read that minor change in the nose can be a very real side effect. I was wondering whether it was likely the procedure would alter my nose for the worse? I have also heard of vermillion advancement surgery, but I’m unsure as to whether this shortens the philtrum length to give a lifted effect (which is my main reason for the surgery). Could you provide insight here? Thanks a lot.
A:While nostril distortion is not a side effect that I have ever seen from a subnasal lip lift, that risk is undoubtably dependent on how much upper lip tissue is removed as well as the surgical technique used to do it. (wrapping the excision/scar line around the nostrils is a sure way to potentially distort the nostrils) But the way to avoid that risk completely is a vermilion advancement which is also a more complete procedure as it changes the entire vermilion exposure from one mouth corner to the other. Men do exceptionally well with this procedure from a scar standpoint because of their beard skin. You are not an ideal candidate for a subnasal lip lift because of your thinner upper lip at the sides in which an isolated fuller central upper lip may create a A frame deformity appearance.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m looking at the website, but it’s not like most plastic surgeon websites. Does the doctor actually perform the surgery? Or does he supply the custom implant to a surgeon of my choosing?
A: I assume you are looking at www.eppleycustomfacialimplants.com in which after 1,000 custom facial implants performed I show the many different types of types and styles that are available and in which I have done. I do not design or supply custom facial implants to other surgeons.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m currently undergoing orthodontic treatment for a Lefort I + SARPE surgery in the future. I have a class 3 malocclusion. This surgery should help (though not completely fix my bite). The lower portion of my maxilla is very narrow, and my mandible has shifted and become asymmetric so that my molars connect. However, it’s really my entire maxilla which is quite recessed, and not just the lower portion. I have a very/flat recessed eye area as well (hardly any cheekbones). I’m concerned that a lefort 1 is not addressing the whole problem, and really won’t do much to help me cosmetically. I have been researching lefort 2 as an alternative, but can hardly find any surgeons who perform this operation in the USA. Since I came across your site in my search, I was wondering if this is something you offer. Thanks for your time.
A: When the entire midface is recessed a Lefort I osteotomy, as you have correctly surmised, will provide an incomplete aesthetic correction. By only addressing the dentoalveolar part of the problem the nasal base is primarily aesthetically improved. Anatomically a LeFort III osteotomy provides the most complete correction. (although limited to the sagittal plane)
While more anatomically complete there are quite a few differences (tradeoffs) between a LeFort I and III osteotomies. The latter requires eyeid incisions (technically a coronal scalp incision is more ideal) and osteotomies across the orbital floor and cheek areas. These invariably heal with irregularities and some palpable bony stepoffs. In contrast the LeFort I is a far more aesthetic operation with an intraoral approach only with no evident bony stepoffs.
While LeFort procedures above the I level may be appealing in diagrams, there are aesthetic tradeoffs with their use that are not obvious in such drawings and should be very carefully considered and undertaken with caution. There is a reason they are primarily used in younger syndromic patients with more substantative bony deformities.
While these LeFort II and III procedures can be done in the highly motivated patient a more prudent and effective approach is to employ both a LeFort I osteotomy with custom midface implants above it, either done concurrently or staged.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, how much clavicle lengthening in shoulder widening surgery is safe?
A: t is not a question of safety but what the regional anatomic limitations are. The amount of clavicle lengthening that can be achieved on each side is 20mms. More lengthening would still be safe but the attached shoulder and scapular tissues will not let the clavicle to be pushed out further. (I have yet to see a patient who can get beyond the 20mms as I would love to get 25mms per side)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in making my brow bones more symmetrical, especially in bringing the higher brow to a lower position, can this be done through custom brow bone implants, and I don’t want to have to raise the position of the lower brow because I think it is more aesthetic than the higher one. I have attached my pictures. I’m waiting for your reply.
A: It does appear that your left brow bone is smaller than that of the right which would explain the higher eyebrow on the left side. Because of the underlying bone asymmetry it may be possible to lower the higher eyebrow with an implant design that makes a better structural match to the other side.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have read online that I could wear a garment to improve outcomes of rib removal waist reduction? Will that help? I need some curve!! And for shoulder reduction when can I get back to the gym for lower body then upper body/ do a push up like yoga?
A: Compression garments, like real corsets or even shapers, can only benefit rib removal surgery in the short term by helping reduce swelling earlier and providing ideal soft tissue shaping. So am I am for their short term postoperative use. More compression is better than less as long as it is tolerable.
For shoulder reduction surgery it will be at least 8 weeks before more strenuous upper body work can be undertaken.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had PMMA cheek and chin implants placed 6 years ago. I’m looking to go the custom route now to address the asymmetry caused by the implants. As such, I have a couple of questions:
– Can the PMMA implants be removed easily without damaging soft tissue?
– Will the existing implants make it impossible for new implants to be designed? Do they have to be removed first?
Thank you!
A: In answer to your facial implant questions:
1) Since the bone nor the soft tissue bonds directly to PMMA their removal should be successfully done. However whether there is bone overgrowth on them, or more importantly, bone resorption under them (most relevant to the cheeks in which there may be maxillary sinus exposure on their removal) it would be important to know what the surrounding bone looks like by a preoperative 3D CT scan.
2) As a general rule I don’t find the need to first remove any facial implants for either custom facial implant designing or their placement. But the need for a preoperative 3D CT scan remains to have more insight into the indwelling implants and the tissue reactions around them.
Dr. Barry Eppley
Indianapolis, Indiana