Your Questions
Your Questions
Q: Dr. Eppley, I am a middle aged man who had cheek bone implant about surgery about 30 years ago in my early 20s . I had the implants removed about a year after the surgery as I felt they were to big. Unfortunately my face sagged when the implants were removed. I have learned to live with it as I did not know there was a remedy. As time goes by my face obviously has sagged more with age. I read that you can re suspend the tissue with a mitek suture.
A: The most effective treatment for cheek sagging after cheek implant removal is the placement of new cheek implants not cheek tissue resuspension. That is a poorly effective procedure for cheek ptosis.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in a customized one piece jaw and chin implant. I have an existing chin implant which has held up very well with military activities. I am an infantryman so it’s the rough and tough exposure. I’ve gone through wrestling classes with it and it hasn’t given me any problems, I’m wondering if this full piece would have similar resilience to stress. Let’s say I get punched in the face, I’m not going to have a piece of loose jaw under my skin hopefully. Appreciate your feedback.
A: As a general rule the best way to avoid complications is to not change something (chin implant) that has never yet had a problem. While I think a custom jawline implant would hold up as well as your existing chin implant, there are no guarantees that it will.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 42 year old female who is considering doing a high smas face lift to help correct some mid face hypoplasia and cheeks that have dissented. Saw a surgeon for this and was about to book but my friend sent me your article about custom implants. I was told I have a recessed upper jaw by an oral surgeon.
I want to know which is a better choice for my situation – high smas, custom implants, or both. I’d like an option that lasts me at least 8-10 years that looks natural and youthful.
A: I am not sure how a midface can be effectively lifted when the bone support is lacking as there is nothing to hang the tissues onto or maintain its position. Midface tissues naturally descend prematurely when there is lack of bone support. The correction of midface hypoplasia is to add support which will naturally provide a lift. A lift without bone support is a wasted effort particularly in a young person.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in your forehead implant procedure, and I had sent you photos, I forgot to clarify a doubt I have, in relation to the photos I attached, is it possible to perform such a pronounced increase without modifying the temporal area? I would not like to enlarge that area because it is already large, if the projection of the implant is approximately 20 or 25 mm thick, how unnatural would it be without temporary implants? Would it be very marked?
I am sending you a picture of me, one of how I would like the result without temporary implants, and another of the idea I have of how it would look without the lateral implants. I thank you for your kind attention and information!
A: In answer to your forehead augmentation questions:
1) No one needs a 20 to 25mm forehead augmentation. That is way over estimating how much is needed to achieve a vertical forehead slope change. It is probably closer to 12mm to 15mm max.
2) With any forehead augmentation when the slope is lessened the width issue of the forehead is often overlooked. Small amounts of forehead slope change may not require the augmentation to go beyond the bony temporal lines. But in more major changes like the one you are considering that would be a must otherwise your forehead would look like a dolphin!. Thus the question is not whether a major forehead augmentation needs to cross the bony temporal line but how far it needs to extend into the temporal region to avoid an unnatural forehead shape.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, custom jaw implants – how does you go about making them? Is 3D imaging provided at your facility or you refer patients to a local imaging facility? If so, can imaging be provided the same day as consultation or I have to prolong my stay for a few days? What is success rate of these procedures in terms of surgery and post-surgery complications?
A: In answer to your custom facial implant questions:
1) The patient gets their 3D scan at a local facility, we provide the order for it.
2) Designing custom facial implants is a process that involves imaging goal setting using the patient pictures and online engineering with 3D Systems company.
3) Facial image goal setting can be established once patient pictures are obtained, whether that is done before a virtual or office consultation or after.
4) While custom facial implants have a high success rate, as they achieve facial changes that are not possible by any other method, it does involve an implant which has its own unique risks of potential revisional surgery. In custom facial implants my experience has been that up to 1/3 of the patients will undergo some form of revisional surgery, almost always for aesthetic reasons.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a couple of questions for that I was hoping you could answer about testicle implants:
1) You mentioned an expectation that the scrotum would initially be tight following the surgery but would “relax” or “loosen” over time. Can he provide any more detail of what I should expect in that respect? Is there anything that can be done to help along that process?
2) You mentioned a risk of wraparound implants detaching. I would be curious in knowing the actual percentage risk of detachment in cases like mine.
A: In answer to your testicle implant questions:
1) It usually takes 2 to 3 months for the scrotum to stretch and fully relax. Because the scrotum is in a gravity dependent position time is favorable for this relaxation process.
4) Up to 1/3 of wrap around implants will have the complication of detachment (separation) either in the short or long-term. Thus it is not an insignificant risk of it happening.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I’m particularly interested in if it’s possible to reduce my skull width/size to within a cis female range.
A:The answer to what is possible begs the question of what is a female skull size/shape compared to what you have now? In other words can skull reduction surgery make enough of a visible difference to achieve a head feminizing effect from your perspective? If I has a better understanding, from a visual standpoint, of what you would consider as the desired change I could then answer the question of whether it is surgically possible. My suspicion is that it would take a 360 degree circumferential approach to achieve that effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a left rib flare birth defect. My 10th rib is totally twisted outwards at its tip which hurts when rotating or bending. Audible clicking sound, but no “sleeping syndrome”. I am in GE Germany and surgeons prefer conservative methods here. I wanted to know what was your point of view on my problem and if there is another solution than acceptance.
Thanks Dr !
A: The 10th rib flare can be reduced or eliminated based on how much of the rib can be safely resected. (in which a CT scan will provide that information) I would at least get that info and then see how much improvement can be achieved by rib removal surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have deep set, low brows and small eyes. I wanted to know if there anything that could make my eyes look more open.
A:There are two procedures that would open up deep set eyes in a female, brow bone reduction and a browlift. Whether an upper blepharoplasty as well would be helpful is also consideration.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
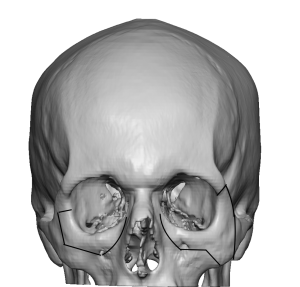
Q: Dr. Eppley, I had zygomatic bone repositioning. In the CT scan I’m wondering, why I do not see bone union in my maxillary region after zygomatic bone reposition (osteomy, delayed reposition). After surgery there is bone union on zygomatic arch, on the orbital rim, but maxillary region.
How it’s possible that gap has not reduced even a bit since surgery? Overally the whole bone complex is stabilised but I’m worried about those gaps on maxillary bone
I attached some pictured from different CTs. CT performed before miniplates removement – 2 years after surgery
I got tinnitus and ETD and I wonder if such gap can be bad for my health… maybe some bacteria from sinuses may transfer to other skull regions?
But once again, how it’s possible that gap has not reduced, like there is no bone. I marked (red line) the place where is very small distance between bone ends and still no union there
Or maybe there is a bone but too thin to be visible on CT? how to check that?
A: I don’t see any mystery here…. the thin bones of the maxilla and even the zygomatic body often heal by a fibrous union not a bony union. These are thin bones that don’t carry much functional loading forces so they are not going to heal like the thicker skull or mandible. There are no medical issues associated with this type of common midfacial bone healing pattern.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, what the risks in temporal artery ligation in stopping blood flow in this artery. In other words, what is impacted by loosing blood flow (forehead/scalp skin impacts, loose of hair, risk of stroke, other)?
A: This is a common concern that, fortunately, has no anatomic basis. The arteries that feed the scalp are not endpoints but actually connect with the arteries from the opposite side in what is called an extensive anastomotic network. Thus you really can’t shut off the blood flow to the scalp almost no matter what you do. It is these anatomic anastomoses which makes it necessary in temporal artery ligation to shut off the inflow and the backflow from the visible artery locations for it to work in decreasing their visibility.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Is an 8cm Clavicle Reduction feasible? Is it possible to get 2 Rounds Of Clavicle Width Reduction?
A: I am not sure whether with an 8cm reduction you are referring to one side or both sides combined. If you mean 8cm per side that would not be possible even with 2 rounds of clavicle reduction surgery. If you are referring to 8cms combined for both sides then it could be done with 2 rounds of the surgery.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am wondering if you could kindly advise at what age is it possible to have treatment for a brachycephalic head shape? Is it possible to treat younger patients or is it advisable to wait until adulthood?
A: Anytime after puberty would be fine for aesthetic skull reshaping procedures as the skull is fairly mature by the teenage years.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Are skull implants permanent ? Any problems after the surgery and any precautions in one’s lifetime with them?
A: Skull implants are permanent and never need to be replaced. As long as one is happy with the initial aesthetic result there is no need to do anything with the implant for the rest of one’s lifetime.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Is it possible to reshape a skull that is affected from Pagets disease?
A: I assume you are referring to reducing the exostoses or overgrowths that occur on the outer surface off the skull. Such exostoses are usually softer bone that is more vascular but they can be reduced. The more pertinent question is will they reoccur and/or are they more prone to reoccur because of the underlying pathology?
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am planning to have an approximately 2000 graft FUE scalp to beard transplant, covering basically the entire classic beard area. With you, we have met and planned for several facial cosmetic surgeries some day later this year TBD. (e.g including IOM implants and sliding genio etc)
For scheduling purposes, I am wondering if there is a number of months I should wait before or after the surgeries with you to get the beard transplant.
A: I would allow for 3 months either before or after any facial surgery for doing a beard transplant.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in undergoing reversal V-line surgery and would like to know the best approach for achieving a natural-looking jawline while still being able to participate in activities such as sparring in the future. I aware that custom jawline surgery is a common option, but I am curious if custom bone grafting would be a more natural and stronger option.
A: Onlay bone grafting is never a viable option for any form of aesthetic jaw augmentation for a number of practical and biologic reasons, most notably the high and irregular absorption of the bone grafts that will occur.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, My question is therefore whether submental placement of jaw and chin implants is to be preferred over intraoral in terms of safety and infection risk? I know Dr. Eppley has done both of these, but what are the pros and cons of going submental vs. intraoral?
A: In custom jawline implant placements, three incisions are needed….one anterior and two posterior. The two posterior incisions are always intraoral and are located way back in the mouth opposite the 2nd/3rd molars. The only ‘debate’ is whether the anterior incision at the chin area is intraoral or submental. To decrease the risk of infection and potential mental nerve injury the submental approach is preferred. In very small custom jawline implants that are used in some females the anterior intraoral approach may be able to be used but with that comes the aforementioned increased risks.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am going to “study” the custom facial implant design and get back to you on it. But I have two questions:
1) I see different measurements between the two sides, should I chose one of them or do I have an asymmetrical face?
2) Is it possible to get a computer simulation of ” my new face” with the lue implants?
Thank you very much and best regards
A: 1) When implant measurements are asymmetrical that is because the program sees an asymmetrical bone structure and that is compensated for in the implant design.
2) Custom implants are made for the bone and there is no software that can predict exactly how that will look on the outside. Thus much of the implant design is based on the surgeon’s judgment and experience of a likely aesthetic result. Knowing exactly what the aesthetic outcomes are from an implant design remains the missing part of the custom implant design process.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am currently considering getting a temporal reduction surgery, but I am wondering what the recovery process may be like for this procedure. I understand that for some surgeries, the recovery process can be quite long (a few weeks to months) and require certain types of diets, while for other surgeries, the recovery process can be very short (a few days or less). Thank you so much for your help!
A: The recovery from temporal reduction surgery is remarkably quick. Other than some expected temporal swelling there are no postoperative physical limitations. One can eat and drink immediately after surgery in an unrestricted fashion. Most of the swelling subsides by 10 to 14 days after the surgery.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I was considering getting implants for my bone brow. However i am a boxer, will these implants interfere with my boxing career and if so what can i do to prevent any damage.
A: While I have never put forehead or brow bone implants into a patient that boxes, I do not see it as a problem. You can’t break the implant and it would be hard to displace it with any force. It actually has an opposite effect…it adds a layer of protection or acts like a bumper guard for the bone.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, When would I have enough mobility to resume massage therapy work after clavicle reduction surgery? Could you also explain to me in more detail, how the recovery in mobility will evolve?
A: As a massage therapist I would think 6 to 8 weeks would be the soonest. That is fairly strenuous arm work. Whether that time period is too optimistic I can not say since I have never yet had a massage therapist.
The evolution of postop arm mobility does according to the following schedule:
1st 2 weeks = keep elbows at side as best as you can
2nd 2 weeks = arms can go out ot 45 degrees
3rd 2 weeks = arms can go out to 9- degrees.
4th 2 weeks = full range of arm motion allowed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I plan to get orthognathic surgery in the near future which will change my jaw most notably so I didn’t include a side profile but I still have some concerns with some frontal features that seem like they cause poor facial harmony. My first concern that I wanted to bring up is the width of my lips. They are quite narrow and the fullness of them exaggerates that as well. I also think I could benefit from eyelid procedures to make me eye area appear less droopy and sad and make them more awake and angular.
A:The problem with mouth widening in patients with full lips is that it not well seen…as the height of the widened lips would be so much more narrow than the natural fullness of the rest of your lips.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had otoplasty 6 months ago. Cartilage was removed from my conchal bowl and the antihelix was created by mustarde sutures (3 sutures per ear). I was very unsatisfied with the results since it was pinned too much to my head. 4 weeks ago i had a revision, and im still not very sure about the result. It got less, but still not as i wanted it to be. Is it possible you could take a look at some pictures and give me advice.
 A: I will be happy to look at your pictures but the bottom line undoubtably is…when an otoplasty is overcorrected and cartilage has been removed in doing so simply releasing it months later will make very little difference in the over correction. Effective subtotal reversal otoplasty requires some cartilage support to be put back to get a more effective and sustained change.
A: I will be happy to look at your pictures but the bottom line undoubtably is…when an otoplasty is overcorrected and cartilage has been removed in doing so simply releasing it months later will make very little difference in the over correction. Effective subtotal reversal otoplasty requires some cartilage support to be put back to get a more effective and sustained change.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, do you perform subcranial modified orbital box osteotomies?
 A: You are referring to a lower 180 degree orbital box osteotomy done through a combined lower eyelid and intraoral incisional approaches, an operation of which I am familiar and have done. It is certainly far less invasive than the transcranial 360 degree orbital box osteotomies which allows it to fall into an aesthetic operation for adults. It is, however, more limited in what it can accomplish and thus its primary indication is when 10mm or less of orbital widening (interpupillary distance increase) is needed. There are two variations of this type of limited orbital box osteotomy depending upon whether some cheek widening effect is also needed.
A: You are referring to a lower 180 degree orbital box osteotomy done through a combined lower eyelid and intraoral incisional approaches, an operation of which I am familiar and have done. It is certainly far less invasive than the transcranial 360 degree orbital box osteotomies which allows it to fall into an aesthetic operation for adults. It is, however, more limited in what it can accomplish and thus its primary indication is when 10mm or less of orbital widening (interpupillary distance increase) is needed. There are two variations of this type of limited orbital box osteotomy depending upon whether some cheek widening effect is also needed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a 23 yo female. I am actually quite satisfied with how I look from head on (I’ve no prior procedures). I’m dissatisfied with the slight nasal hump and nasal tip drooping, but am more concerned with the weakness of the profile of my chin.
I have considered going to local, domestic, and international surgeons. However I am fearful that I might go to someone who will not adequately address my concerns and that I will have limited improvement in my chin projection thus wasting my time and money. I’m impressed by your work and thoroughness and would rather travel to you for such an operation.
I anticipate a more aggressive approach to produce as much augmentation as possible. Potential through the use of multiple procedures/techniques. Sliding Genioplasty, Chin Implant, Custom Implant, and Chin fillers are all procedures that I’m open to. I don’t think I can make a well informed decision. I prefer an option that is permanent, offers significant projection to the chin, avoids severe labiomental fold, and that is within my budget. I will take your suggestion on what might be best.
A: In answer to your chin augmentation questions:
1) With the significant weakness of your chin you are only a candidate for a sliding genioplasty and not an implant. Your horizontal projection increase in the chin exceeds what any implant can do or the stretch of the soft tissues of the chin to accommodate that change over an implant.
2) The amount of chin bone movement you need is well into the double digits, probably in the 14 to 16mm range at least. (see attached imaging). In addition to coming that far forward it also needs to be vertically shortened to avoid making the chin longer which can inadvertently happen when that amount of chin bone advancement is done. The tightness of the soft tissues over the chin when it is moved this amount will preclude the use of a chin implant over it. That is best anyway as make your own natural tissues do all of the work of the augmentation.
3) The labiomental fold is going to get deeper which is unavoidable. That is the aesthetic tradeoff for any significant horizontal chin increase.
4) Patients coming in for surgery and traveling home is the norm in my practice, not the exception.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have microcephaly. My head circumference is 21cm although i have normal intelligence, this condition is psychologically distressing and has negatively impacted my self-esteem. I often stuff my wigs with clothe just to add volume to my head and give off an illusion of a semi normal sized head. Is a reconstruction possible for me that would make my head size bigger? that would be a dream since microcephaly is incurable and permanent. Thank you.
A: Skull augmentations using custom implants can provide some increases in head size based on how much the scalp can stretch to accommodate the underlying augmentation. Most significant head size increases require a two stage skull augmentation approach using a first stage scalp expansion.
To determine what can be done in your case I would need to evaluate and do some imaging using pictures of your head.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am a 45 year old man. I have desired testicle enhancement for many years, since I was in my early twenties. Now that I see that an implant that envelopes the testicles individually to enlage them is on the market, i would actually consider having such a prosedure done. I have previously had a vesectomy and I would prefer if at all possible for a potential prosedure to be done under local anasthetic.
A: In answer to your testicle implant questions:
1) I have designed and used various styles of wrap around testicular implants which is a clever concept for it. But it is plagued by a certain percent of secondary implant-testicle separations (testicle coming out of the implant) for which I have not solved how to completely prevent that postoperative risk from occurring.
2) This is not a procedure I would perform under local anesthesia.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I found you on the internet while searching for a resolution to un even butt cheeks. I’d love to have a virtual consultation if they’re offered.
A: Given the volumetric difference between the two buttocks and your lack of fat harvest sites (from a prior BBL harvest ??) the remaining treatment approach would be a small intramuscular buttock implant on the smaller side.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am scheduled to have a unilateral clavicle reduction but wanted to first understand the recovery process in more depth. I live in Montana and needed to understand the travel aspects (how long I need to be in Indianapolis), how long I will be unable to use my arm for computer office work, and whether I can manage on my own post-op since this would be a unilateral procedure. Any other pertinent info would be helpful, too.
A: In answer to your logistical surgery questions:
1) Having one good arm, which is unlike every clavicle reduction procedure I have done to date, allows for numerous advantages doing the recovery period one of which allows for a more rapid return home. Assuming you are coming by yourself you should be able to return home in 2 to 3 days after the surgery.
2) The key to the first few weeks after surgery is to keep the elbow of the affected arm near your side. While I have never used postoperative slings/garments after clavicle reductions due to their bilateral nature, you would represent the exception in which it is probably of benefit. Think of your one arm in a sling (not when showering) when determining how activities will be affected in the first few weeks after the surgery.
3) As a unilateral procedure you should be able to handle the immediate after care given that many bilateral patients do…albeit with more difficulty and requiring some nursing support.
Dr. Barry Eppley
World Renowned Plastic Surgeon